You might also like
- MESOTHERAPYDocument11 pagesMESOTHERAPYimec_coordinator7353100% (3)
- Small Molecule Drug Design PDFDocument20 pagesSmall Molecule Drug Design PDFDORA ROJASNo ratings yet
- CHAPTER 1 Hospital PharmacyDocument25 pagesCHAPTER 1 Hospital PharmacyMurtaza Haider100% (2)
- Clinical Pharmacokinetics and Pharmacodynamics: Dr. Abaasi KabogoDocument52 pagesClinical Pharmacokinetics and Pharmacodynamics: Dr. Abaasi KabogoNina100% (1)
- Hanoo 2Document20 pagesHanoo 2mr samoNo ratings yet
- 81635793Document13 pages81635793Brock TernovNo ratings yet
- Running Head: 1: Drug Formulation & PerformanceDocument8 pagesRunning Head: 1: Drug Formulation & PerformanceKhadejah StewartNo ratings yet
- An Open-Label, Phase 1 Study To Evaluate The Effects of Hepatic Impairment On Edoxaban Pharmacokinetics and PharmacodynamicsDocument11 pagesAn Open-Label, Phase 1 Study To Evaluate The Effects of Hepatic Impairment On Edoxaban Pharmacokinetics and PharmacodynamicsHendrawan RahmanNo ratings yet
- Acos y 17b Estradiol PDFDocument22 pagesAcos y 17b Estradiol PDFAli de RoNo ratings yet
- Design Synthesis Characterization and in Vivo Antidiabetic Activity Evaluation of Some Chalcone DerivativesDocument12 pagesDesign Synthesis Characterization and in Vivo Antidiabetic Activity Evaluation of Some Chalcone DerivativesSami ZiaNo ratings yet
- Clinical Pharmacokinetics and Pharmacodynamics of Opioid Analgesics in Infants and ChildrenDocument20 pagesClinical Pharmacokinetics and Pharmacodynamics of Opioid Analgesics in Infants and ChildrenmaryNo ratings yet
- Biowaiver Monographs For Immediate-Release Solid Oral Dosage Forms: KetoprofenDocument11 pagesBiowaiver Monographs For Immediate-Release Solid Oral Dosage Forms: KetoprofendyanNo ratings yet
- Antiepileptic Drug Interactions - Principles and Clinical ImplicationsDocument14 pagesAntiepileptic Drug Interactions - Principles and Clinical ImplicationsErkan KirkNo ratings yet
- US Food and DrugDocument100 pagesUS Food and Drugomega1966No ratings yet
- Bioequivalence Study of Two Loperamide HydrochloriDocument5 pagesBioequivalence Study of Two Loperamide HydrochloriLoRna Nu'aNo ratings yet
- Toxicophores: Groups and Metabolic Routes Associated With Increased Safety RiskDocument13 pagesToxicophores: Groups and Metabolic Routes Associated With Increased Safety RiskMercedes ArmijosNo ratings yet
- The Potential For Interaction of Tolbutamide With Pomegranate Juice Against Diabetic Induced Complications in RatsDocument7 pagesThe Potential For Interaction of Tolbutamide With Pomegranate Juice Against Diabetic Induced Complications in RatsNurul Rizqan SeptimaNo ratings yet
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- Effects of Platinum Compounds Viz Cisplatin, Carboplatin & Oxaliplatin On Renal Parameters: A Comparative StudyDocument11 pagesEffects of Platinum Compounds Viz Cisplatin, Carboplatin & Oxaliplatin On Renal Parameters: A Comparative Study9460106212No ratings yet
- 03 PharmacometabolomicsDocument11 pages03 PharmacometabolomicsVanessa CarreraNo ratings yet
- Tamoxifeno AdDocument12 pagesTamoxifeno AdLeonardo Avila MirandaNo ratings yet
- Barber 1997 - Validation of A Questionnaire For Comparing The Tolerability of Ophthalmic MedicationsDocument9 pagesBarber 1997 - Validation of A Questionnaire For Comparing The Tolerability of Ophthalmic Medicationsflavio1No ratings yet
- RingwormDocument324 pagesRingwormRizky GumelarNo ratings yet
- Neurourology and Urodynamics - 2024 - Herschorn - Safety and Efficacy of An 1 Blocker Plus Mirabegron Compared With AnDocument16 pagesNeurourology and Urodynamics - 2024 - Herschorn - Safety and Efficacy of An 1 Blocker Plus Mirabegron Compared With Andr.yogaNo ratings yet
- NIH Public Access: Alterations of Chemotherapeutic Pharmacokinetic Profiles by Drug-Drug InteractionsDocument30 pagesNIH Public Access: Alterations of Chemotherapeutic Pharmacokinetic Profiles by Drug-Drug InteractionsGaby ValenzuelaNo ratings yet
- Pediatric PharmacotherapyDocument4 pagesPediatric PharmacotherapyRiriNo ratings yet
- Featured Article: Is Dextromethorphan A Concern For Causing A False Positive During Urine Drug Screening?Document4 pagesFeatured Article: Is Dextromethorphan A Concern For Causing A False Positive During Urine Drug Screening?Cut Nyak Ilma AsyuraNo ratings yet
- Chimica Farmaceutica Proteins As Drug TargetsDocument40 pagesChimica Farmaceutica Proteins As Drug TargetsGiuliano SchiediNo ratings yet
- BDDCS Predictions, Self-Correcting Aspects of BDDCS Assignments, BDDCS Assignment Corrections, and Classification For More Than 175 Additional DrugsDocument10 pagesBDDCS Predictions, Self-Correcting Aspects of BDDCS Assignments, BDDCS Assignment Corrections, and Classification For More Than 175 Additional DrugsBagoes AsNo ratings yet
- 2015 Article 9845Document10 pages2015 Article 9845FelixNo ratings yet
- My JournalDocument10 pagesMy JournalFelixNo ratings yet
- Jurnal Efficacy and Tolerability of Adjunctive Lacosamide in Pediatric Patients With Focal SeizuresDocument15 pagesJurnal Efficacy and Tolerability of Adjunctive Lacosamide in Pediatric Patients With Focal SeizuresAnida HasnaNo ratings yet
- Environmental Science-2Document33 pagesEnvironmental Science-2NEELKANTH MARANDINo ratings yet
- Bcs Classification of DrugsDocument12 pagesBcs Classification of Drugsjigarpatel5No ratings yet
- A Systematic Review and Meta Analysis of The Adverse Effects of Levonorgestrel Emergency Oral ContraceptiveDocument26 pagesA Systematic Review and Meta Analysis of The Adverse Effects of Levonorgestrel Emergency Oral ContraceptiveperezhuertalexieNo ratings yet
- AndrzejowskiPandCarrollW2016 BMJADCPharmacyUpdate CodeineinpaediatricsDocument5 pagesAndrzejowskiPandCarrollW2016 BMJADCPharmacyUpdate CodeineinpaediatricsKhairul AmryNo ratings yet
- Fortuna 2013Document14 pagesFortuna 2013amaliaNo ratings yet
- Fphar 14 1260599Document11 pagesFphar 14 1260599mimi.mca.1921No ratings yet
- Bioequivalence Evaluation CelecoxibDocument7 pagesBioequivalence Evaluation Celecoxib0yukitenshi0No ratings yet
- Did Pfizer Do Any Safety StudiesDocument20 pagesDid Pfizer Do Any Safety StudiesJindřich CieślickiNo ratings yet
- Pharmaceutics 13 00401Document17 pagesPharmaceutics 13 00401Nikita jainNo ratings yet
- Inhibition and Induction of CYP Enzymes in Humans: An UpdateDocument52 pagesInhibition and Induction of CYP Enzymes in Humans: An UpdateNurul Kamilah SadliNo ratings yet
- Honk R7Document10 pagesHonk R7fitri asymidaNo ratings yet
- Pharmacogenetics and The Concept of Individualized Medicine: BS ShastryDocument6 pagesPharmacogenetics and The Concept of Individualized Medicine: BS Shastrykunalprabhu148No ratings yet
- OlanzapinePlusSamidorphanSchizophreniaAUDProtocol CITROME InnovClinNeurosci2019Document7 pagesOlanzapinePlusSamidorphanSchizophreniaAUDProtocol CITROME InnovClinNeurosci2019Leslie CitromeNo ratings yet
- Dosing Antibiotics in Neonates - Review of The Pharmacokinetic DataDocument16 pagesDosing Antibiotics in Neonates - Review of The Pharmacokinetic DataMyOnlyZiboNo ratings yet
- Cleaning Validation Hbel Calculation by IspeDocument26 pagesCleaning Validation Hbel Calculation by IspeBhaskar Napte100% (1)
- Van Erp Et Al, 2009, Clinical Pharmacokinetics of Tyrosine Kinase InhibitorsDocument15 pagesVan Erp Et Al, 2009, Clinical Pharmacokinetics of Tyrosine Kinase Inhibitorsdhania novitasariNo ratings yet
- 2010 Strategies in The Design of Nanoparticles For Therapeutic ApplicationsDocument13 pages2010 Strategies in The Design of Nanoparticles For Therapeutic ApplicationsGeorge Michael Alvarado LopezNo ratings yet
- FDA Nanoparticle Therapeutics Review FinalDocument42 pagesFDA Nanoparticle Therapeutics Review FinalMinh Đặng NhậtNo ratings yet
- Faught Et Al-2015-British Journal of Clinical PharmacologyDocument9 pagesFaught Et Al-2015-British Journal of Clinical PharmacologyHendra Wana Nur'aminNo ratings yet
- Effect of Dietary Proteins On Isoniazid Induced Subchronic Hepatotoxicity in SD RatsDocument27 pagesEffect of Dietary Proteins On Isoniazid Induced Subchronic Hepatotoxicity in SD RatsHasitha Shilpa AnantharajuNo ratings yet
- Drug Discovery Paper m1Document6 pagesDrug Discovery Paper m1Aditi ShimpiNo ratings yet
- Metabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsDocument33 pagesMetabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsAndi wahyuniNo ratings yet
- Comparative Steady-State Bioavailability of Sustained-Release Theophylline Prep Arations: Theo-Dur®, Uni-Dur® and Xan Thium®Document10 pagesComparative Steady-State Bioavailability of Sustained-Release Theophylline Prep Arations: Theo-Dur®, Uni-Dur® and Xan Thium®Windy Gigiers SeptianiNo ratings yet
- KejangDocument6 pagesKejangKijang 2018No ratings yet
- Ropivacaine Vs Bupivacaine PDFDocument6 pagesRopivacaine Vs Bupivacaine PDFJessica LawrenceNo ratings yet
- Journal of Clinical Medicine-7 April 2023 PublicationDocument21 pagesJournal of Clinical Medicine-7 April 2023 PublicationNARESHNo ratings yet
- Epilepsi TreatmentDocument11 pagesEpilepsi Treatmentakak74831No ratings yet
- The Journal of Clinical Pharma - 2018 - Den Anker - Developmental Changes in Pharmacokinetics and PharmacodynamicsDocument16 pagesThe Journal of Clinical Pharma - 2018 - Den Anker - Developmental Changes in Pharmacokinetics and Pharmacodynamicsnoviantyramadhani12No ratings yet
- Sumber Kasus 3 No 3Document12 pagesSumber Kasus 3 No 3meutia salsabilaNo ratings yet
- The Use of Aromatase Inhibitors in Infertility and GynecologyDocument9 pagesThe Use of Aromatase Inhibitors in Infertility and Gynecologyalan lowusNo ratings yet
- Food and Drug Interactions A General ReviewDocument15 pagesFood and Drug Interactions A General ReviewDaniela AndreiNo ratings yet
- Instructions To Author-REACH2020Document2 pagesInstructions To Author-REACH2020pharma xlNo ratings yet
- Resume of Shannon43613Document2 pagesResume of Shannon43613api-29418893No ratings yet
- Avances en Los Sistemas Transdermicos para La Administracion de FarmacosDocument26 pagesAvances en Los Sistemas Transdermicos para La Administracion de FarmacosAlfonso LuisNo ratings yet
- Factsheet of AGP ProjectDocument20 pagesFactsheet of AGP ProjectRij GurungNo ratings yet
- The Concept of Social PharmacyDocument3 pagesThe Concept of Social PharmacyAsmaa AbdelatyNo ratings yet
- 2021 FPH Admission RegisterDocument37 pages2021 FPH Admission Registerums synovNo ratings yet
- Royal MarketingDocument12 pagesRoyal MarketingIsmail MustafaNo ratings yet
- Albendazole Drug InteractionsDocument2 pagesAlbendazole Drug InteractionssonypardeepNo ratings yet
- Medical Representative Interview QuestionsDocument5 pagesMedical Representative Interview QuestionsVishal parasharNo ratings yet
- FDA Foia Log - October 2020Document152 pagesFDA Foia Log - October 2020Corey WarrenbrandNo ratings yet
- Drug StudyDocument5 pagesDrug StudyTracy Malingin QuimqueNo ratings yet
- Pharmacophore 2011 2 2 32Document18 pagesPharmacophore 2011 2 2 32Michael FreudigerNo ratings yet
- Chapter 4 Pharmacotherapeutics, Dynamics & KineticsDocument47 pagesChapter 4 Pharmacotherapeutics, Dynamics & KineticsAshaNo ratings yet
- Features and Uses of Rectal PreparationDocument4 pagesFeatures and Uses of Rectal Preparationhira khanNo ratings yet
- Fluids Quiz 2Document6 pagesFluids Quiz 2Monika DeviNo ratings yet
- January 2009 Room Assignments For Pharmacy Licensure ExaminationDocument35 pagesJanuary 2009 Room Assignments For Pharmacy Licensure ExaminationdericNo ratings yet
- Tablet and Capsule To Be Crushed (Mah Sue Lyn, Zaid)Document8 pagesTablet and Capsule To Be Crushed (Mah Sue Lyn, Zaid)khangsiean89No ratings yet
- Pharmacology Notes #1Document2 pagesPharmacology Notes #1JUSTINE ALLYSA MAY CASTILLONo ratings yet
- Report - University of Santo Tomas HospitalDocument16 pagesReport - University of Santo Tomas HospitalMikee MeladNo ratings yet
- Mulnopiravir-FDA EUADocument10 pagesMulnopiravir-FDA EUAJaz ButuyanNo ratings yet
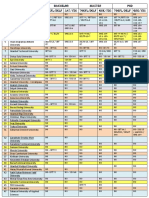
- NO University Name Bachelor Master PHD Toefl/Delf Sat/Yds Toefl/Delf Gre/Yds Toefl/Delf Gre/YdsDocument15 pagesNO University Name Bachelor Master PHD Toefl/Delf Sat/Yds Toefl/Delf Gre/Yds Toefl/Delf Gre/YdsU ConceptsNo ratings yet
- D Pharm.Document20 pagesD Pharm.Gaurav AgarwalNo ratings yet
- Rs Pena 98 Jl. Pemuda Pengasinan N0.36 Kec Gn. Sindur Bogor Telp: (021) 7587 4401,-FaxDocument61 pagesRs Pena 98 Jl. Pemuda Pengasinan N0.36 Kec Gn. Sindur Bogor Telp: (021) 7587 4401,-Faxrichard fernandoNo ratings yet
- Roin Solving The Problem of New UsesDocument77 pagesRoin Solving The Problem of New Usessushaantb400No ratings yet
- Practice of PharmacyDocument12 pagesPractice of PharmacyMycaela Archivido De AlvaNo ratings yet
- Asia3 Product List 2 PDFDocument17 pagesAsia3 Product List 2 PDFYoussef KaidNo ratings yet
- ProposalDocument4 pagesProposalM Imran SajidNo ratings yet