You might also like
- Cholecystitis Concept MapDocument4 pagesCholecystitis Concept Mapnursing concept maps100% (7)
- Sample Internal Medicine Admission NoteDocument4 pagesSample Internal Medicine Admission NoteMayer Rosenberg100% (8)
- Sample Request For Judicial Notice For CaliforniaDocument3 pagesSample Request For Judicial Notice For CaliforniaStan Burman87% (15)
- Gastric Outlet ObstructionDocument9 pagesGastric Outlet ObstructionVivek AhanthemNo ratings yet
- DC Power Source EPU05A-03 - HuaweiDocument11 pagesDC Power Source EPU05A-03 - HuaweiKozics Tibi0% (1)
- Exemplar - Inflammatory Bowel DiseaseDocument1 pageExemplar - Inflammatory Bowel DiseaseMary GiuntiniNo ratings yet
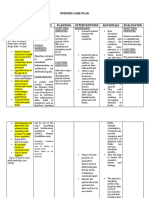
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrahNo ratings yet
- Intussuception Is A Condition in Which Part of The Intestine Folds Into The Section Next To ItDocument3 pagesIntussuception Is A Condition in Which Part of The Intestine Folds Into The Section Next To ItEduard GarchitorenaNo ratings yet
- Dolor y Distensión Abdominal. Abordaje Diagnóstico A Distintas EdadesDocument5 pagesDolor y Distensión Abdominal. Abordaje Diagnóstico A Distintas Edadesmarian martinezNo ratings yet
- Irritable Bowel SyndromeDocument8 pagesIrritable Bowel Syndromea_chiekaNo ratings yet
- Cholecystitis Case StudyDocument7 pagesCholecystitis Case StudyElle MongeNo ratings yet
- Kervin Jude D. Manahan-Written-RevalidaDocument10 pagesKervin Jude D. Manahan-Written-RevalidaKervin Jude D. ManahanNo ratings yet
- Abdominal PainDocument23 pagesAbdominal PainVajirawit PetchsriNo ratings yet
- Assignment GiDocument14 pagesAssignment GiVoid LessNo ratings yet
- Practice: Ulcerative Colitis: Diagnosis and ManagementDocument4 pagesPractice: Ulcerative Colitis: Diagnosis and ManagementBryan NguyenNo ratings yet
- Cap 15Document167 pagesCap 15Saul RivasNo ratings yet
- Celiac Disease Who Should I Test, and HowDocument4 pagesCeliac Disease Who Should I Test, and HowtheriversongsNo ratings yet
- Coeliac DiseaseDocument1 pageCoeliac DiseaseNarelle HuettNo ratings yet
- Inside StoryDocument3 pagesInside StoryAutismeyeNo ratings yet
- 97438-Article Text-254324-1-10-20131121Document2 pages97438-Article Text-254324-1-10-20131121June Faith HacheroNo ratings yet
- Ladja, Irish V. BSN 3-C Laboratory ResultsDocument13 pagesLadja, Irish V. BSN 3-C Laboratory ResultsEzra LambarteNo ratings yet
- Irritable Bowel SyndromeDocument2 pagesIrritable Bowel Syndromei can always make u smile :DNo ratings yet
- IBS ResearchDocument6 pagesIBS ResearchDrHassan Ahmed ShaikhNo ratings yet
- 116 - Alterations in GI EliminationDocument12 pages116 - Alterations in GI EliminationGino-o, KyleNo ratings yet
- Clinical Management: Chronic DiarrheaDocument7 pagesClinical Management: Chronic DiarrheaAnonymous ce3S6XFdwUNo ratings yet
- Irritable Bowel Syndrome: 10-Minute ConsultationDocument1 pageIrritable Bowel Syndrome: 10-Minute ConsultationdrsadafrafiNo ratings yet
- 23 Correspondence Abdominal Pain in PDFDocument2 pages23 Correspondence Abdominal Pain in PDFSebastian Bernal GalloNo ratings yet
- Practical-Algorithms-Diare KronisDocument20 pagesPractical-Algorithms-Diare KronisTiwi QiraNo ratings yet
- 2015 Colectomy Brochure FINALDocument8 pages2015 Colectomy Brochure FINALAnghelo Aldair Velásquez CarrilloNo ratings yet
- Abdominal Pain MARS 2.0 - Dr. Siswidiyati, SP - RadDocument34 pagesAbdominal Pain MARS 2.0 - Dr. Siswidiyati, SP - RadarifdeathsciethNo ratings yet
- Calculous Biliary Disease: Current DiagnosisDocument5 pagesCalculous Biliary Disease: Current DiagnosisFernanda Copete YolianisNo ratings yet
- Gastrointestinal Manifestations of Systemic Lupus ErythematosusDocument5 pagesGastrointestinal Manifestations of Systemic Lupus ErythematosusDaniela Constanta SirbuNo ratings yet
- Constipation. Definition and ClassificationDocument4 pagesConstipation. Definition and ClassificationMiguel RuizNo ratings yet
- Peptic Ulcer & Ulcerative ColitisDocument56 pagesPeptic Ulcer & Ulcerative ColitisZi MeiNo ratings yet
- Diagnosis and Management of Acute Pancreatitis andDocument11 pagesDiagnosis and Management of Acute Pancreatitis andMarcelitaTaliaDuwiriNo ratings yet
- Jejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of LiteratureDocument6 pagesJejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of Literatureellya theresiaNo ratings yet
- Critical Thinking Exercise - Gastrointestinal System: Dan Melton Anthony A. Hizon 3/2/21 Bsn3B NCM116Document8 pagesCritical Thinking Exercise - Gastrointestinal System: Dan Melton Anthony A. Hizon 3/2/21 Bsn3B NCM116Dan HizonNo ratings yet
- Cólica em Neonatos - 2005Document4 pagesCólica em Neonatos - 2005thiago.veterinariaNo ratings yet
- Update in Inflammatory Bowel Disease: Graham MorrisonDocument6 pagesUpdate in Inflammatory Bowel Disease: Graham MorrisonJesse Helmut Hansen-BartelNo ratings yet
- Clinical Approach To A Case of Obstructive JaundiceDocument22 pagesClinical Approach To A Case of Obstructive JaundiceEsraa SalemNo ratings yet
- Evaluation and Treatment of Dyspepsia: ReviewDocument6 pagesEvaluation and Treatment of Dyspepsia: ReviewNurul Afifah MunayaNo ratings yet
- Colitis IndeterminadaDocument6 pagesColitis IndeterminadaMaria FannyNo ratings yet
- Irritable Bowel Syndrome With Diarrhea Treatment Is A Work in ProgressDocument11 pagesIrritable Bowel Syndrome With Diarrhea Treatment Is A Work in ProgressCamila CharryNo ratings yet
- 40768-Article Text-143534-1-10-20190327Document3 pages40768-Article Text-143534-1-10-20190327nakibosmanNo ratings yet
- Crohn's Disease Seminar FinalDocument27 pagesCrohn's Disease Seminar Finalshahad alshareefNo ratings yet
- Table 1. Location of Crohn's Disease and Associated SymptomsDocument11 pagesTable 1. Location of Crohn's Disease and Associated SymptomsKyal OwenNo ratings yet
- (06-02-23) GI System - ContinuationDocument8 pages(06-02-23) GI System - ContinuationMarcus Andrei J RamosNo ratings yet
- Histopathology of Crohn's Disease and Ulcerative Colitis: Section 3Document22 pagesHistopathology of Crohn's Disease and Ulcerative Colitis: Section 3HumoraNo ratings yet
- IBD - Crohns ColitisDocument4 pagesIBD - Crohns ColitisBunga NestapaNo ratings yet
- 10 1053@j Gastro 2019 03 053Document2 pages10 1053@j Gastro 2019 03 053Novara Qus'nul LuvfiantiNo ratings yet
- Funda Sample ScenarioDocument2 pagesFunda Sample ScenarioGadez JeanpelNo ratings yet
- Colico Diagnostico - CirugiaDocument8 pagesColico Diagnostico - CirugiaDana UrueñaNo ratings yet
- NCP FinalDocument18 pagesNCP FinalHelen GonzalesNo ratings yet
- Related Learning Experience Fundamentals in Nursing 4 RotationDocument3 pagesRelated Learning Experience Fundamentals in Nursing 4 RotationMark Eliezer CulasingNo ratings yet
- Evaluation of ConstipationDocument8 pagesEvaluation of ConstipationAndrea GallegoNo ratings yet
- CEG 67233 Optimal Management of Collagenous Colitis A Review - 021016Document9 pagesCEG 67233 Optimal Management of Collagenous Colitis A Review - 021016ricardoatejassNo ratings yet
- Decelos ColostomyDocument7 pagesDecelos ColostomyCharlene Sumba DecelosNo ratings yet
- Irritable Bowel SXDocument13 pagesIrritable Bowel SXjennifer.hd.mfNo ratings yet
- MALABSORPTIONDocument3 pagesMALABSORPTIONZyra LagatNo ratings yet
- DCR 2016 Constipation, Evaluation and Management ofDocument14 pagesDCR 2016 Constipation, Evaluation and Management ofrisewfNo ratings yet
- Methotrexate Induced Apoptotic Colopathy In.17Document2 pagesMethotrexate Induced Apoptotic Colopathy In.17william lozaNo ratings yet
- Bowel StatisticsDocument2 pagesBowel StatisticsbillpaparounisNo ratings yet
- A Simple Guide to Acalculous Cholecystopathy, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Acalculous Cholecystopathy, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Sic 2Document4 pagesSic 2Ezra Miguel DarundayNo ratings yet
- Sic Fracture AgainDocument5 pagesSic Fracture AgainEzra Miguel DarundayNo ratings yet
- DARUNDAY SICwatDocument12 pagesDARUNDAY SICwatEzra Miguel DarundayNo ratings yet
- Surgical Procedure and Instruments Used - DARUNDAYDocument6 pagesSurgical Procedure and Instruments Used - DARUNDAYEzra Miguel DarundayNo ratings yet
- Darunday Sic (Repaired)Document16 pagesDarunday Sic (Repaired)Ezra Miguel DarundayNo ratings yet
- Ezra Miguel. Darunday - NCM For Final Google ExamDocument3 pagesEzra Miguel. Darunday - NCM For Final Google ExamEzra Miguel DarundayNo ratings yet
- Darunday, Ezra M. Rot II (Final)Document16 pagesDarunday, Ezra M. Rot II (Final)Ezra Miguel DarundayNo ratings yet
- Darunday NCP Rotation 6Document3 pagesDarunday NCP Rotation 6Ezra Miguel DarundayNo ratings yet
- Darunday, Ezra M. Study of Illness ConditionDocument4 pagesDarunday, Ezra M. Study of Illness ConditionEzra Miguel DarundayNo ratings yet
- Drug Study Darunday Rotation 3 - DarundayDocument5 pagesDrug Study Darunday Rotation 3 - DarundayEzra Miguel DarundayNo ratings yet
- Darunday Rotation IIDocument16 pagesDarunday Rotation IIEzra Miguel DarundayNo ratings yet
- DARUNDAY LOGIC-101-long-quizDocument3 pagesDARUNDAY LOGIC-101-long-quizEzra Miguel DarundayNo ratings yet
- Device and Network Design: Part 1: Canopen Physical LayerDocument7 pagesDevice and Network Design: Part 1: Canopen Physical Layeryomismo garciaNo ratings yet
- WJ200 Dynamic Braking Selection TableDocument1 pageWJ200 Dynamic Braking Selection TableSandiRuwiyantoNo ratings yet
- Glass MarbleDocument11 pagesGlass MarblesunilkmrrNo ratings yet
- Manganese RailsDocument41 pagesManganese RailsKacper KoniarskiNo ratings yet
- Lesson 18 elementary-english-review-2-units-10-17LPDocument11 pagesLesson 18 elementary-english-review-2-units-10-17LPcinkapankaNo ratings yet
- Maths Text Book ReviewDocument15 pagesMaths Text Book ReviewJigna Khoyani100% (1)
- Einstein Mirror and Fermat's Principle of Least TimeDocument3 pagesEinstein Mirror and Fermat's Principle of Least TimeHanan RosenthalNo ratings yet
- Tax Invoice: IXIFT00004369863: Fare (Incl of All Taxes) 4765.00 Net Other Service Charges & Fees (A) 0.00Document1 pageTax Invoice: IXIFT00004369863: Fare (Incl of All Taxes) 4765.00 Net Other Service Charges & Fees (A) 0.00Manjit raushanNo ratings yet
- Radio FRS Cobra 110 ManualDocument14 pagesRadio FRS Cobra 110 ManualshulistNo ratings yet
- Principle and StrategiesDocument5 pagesPrinciple and StrategiesHanna Grace Honrade100% (1)
- Meniscopexy For Internal Derangement of Temporomandibular JointDocument5 pagesMeniscopexy For Internal Derangement of Temporomandibular Jointmehak malhotraNo ratings yet
- Tabela de Equivalencia de Graxas PDFDocument1 pageTabela de Equivalencia de Graxas PDFJonhNo ratings yet
- B1 Creativity Money Love Can Creativity Be TaughtDocument64 pagesB1 Creativity Money Love Can Creativity Be TaughtAdalto ParadaNo ratings yet
- Tanuj Kumar Majumdar (Optical) Roll-03Document24 pagesTanuj Kumar Majumdar (Optical) Roll-03Tanuj MajumdarNo ratings yet
- Managerial Accounting:: An Introduction To Concepts, Methods, and UsesDocument22 pagesManagerial Accounting:: An Introduction To Concepts, Methods, and UsesamitbaggausNo ratings yet
- Coast 2016 Products CatalogDocument116 pagesCoast 2016 Products CatalogAmmoLand Shooting Sports NewsNo ratings yet
- Proof of The Lagrange Inversion FormulaDocument4 pagesProof of The Lagrange Inversion FormulaVictor MarchantNo ratings yet
- Design of Auxiliary Power Unit (APU) For Co-Operation With Turboshaft EngineDocument61 pagesDesign of Auxiliary Power Unit (APU) For Co-Operation With Turboshaft EngineAnonymous o1NYRvU100% (3)
- Arts - Lesson 1Document5 pagesArts - Lesson 1AQUINO MARVINNo ratings yet
- Coriolis ForceDocument3 pagesCoriolis ForceDipanjan ChaudhuriNo ratings yet
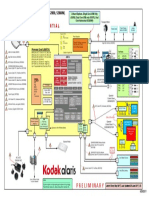
- S 205060 W 7080 Wservicesysteminterconnectdiagramprelimv 228 Jun 171628381144100Document1 pageS 205060 W 7080 Wservicesysteminterconnectdiagramprelimv 228 Jun 171628381144100estiven zapata garciaNo ratings yet
- Physiology FinalADocument18 pagesPhysiology FinalAvaegmundig100% (1)
- S-1 RevisedDocument1 pageS-1 Revisedbernard1agoncillioNo ratings yet
- Reading On Brugada SyndromeDocument10 pagesReading On Brugada SyndromeDonald BidenNo ratings yet
- 6400 - File - LATIHAN SOAL FORM TEKS PURCHASE ORDER X IPA IPSDocument3 pages6400 - File - LATIHAN SOAL FORM TEKS PURCHASE ORDER X IPA IPSKayla SimphonyNo ratings yet
- Formal Report in BioChem LabDocument6 pagesFormal Report in BioChem LabmegmayorNo ratings yet
- 103723-Sandiat West Es Action Plan For Preparatory Activities For Sy 2020-2021Document4 pages103723-Sandiat West Es Action Plan For Preparatory Activities For Sy 2020-2021Divine Grace SamortinNo ratings yet