You might also like
- Occlusal Considerations in Implant Therapy Clinical Guidelines With Biomechanical Rationale PDFDocument10 pagesOcclusal Considerations in Implant Therapy Clinical Guidelines With Biomechanical Rationale PDFSoares MirandaNo ratings yet
- Outlook Group Written AssignmentDocument34 pagesOutlook Group Written Assignmentashish9dubey-1680% (10)
- The Effects Induced by Spinal Manipulative Therapy On The Immune and Endocrine SystemDocument12 pagesThe Effects Induced by Spinal Manipulative Therapy On The Immune and Endocrine SystemCésar EscalanteNo ratings yet
- Obstructive Sleep ApneaDocument21 pagesObstructive Sleep ApneaIJAR JOURNALNo ratings yet
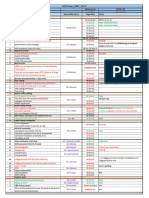
- Hach - MWP (Plan Vs Actual) Status - 22 Oct-1Document1 pageHach - MWP (Plan Vs Actual) Status - 22 Oct-1ankit singhNo ratings yet
- American History 2017-10 PDFDocument76 pagesAmerican History 2017-10 PDFCristian OvanisofNo ratings yet
- TAM Poster 17 5 PRINTDocument1 pageTAM Poster 17 5 PRINTtonywiharjitoNo ratings yet
- Orofacial Musculoskeletal Pain. An Evidence-Based Bio-Psycho-Social Matrix ModelDocument27 pagesOrofacial Musculoskeletal Pain. An Evidence-Based Bio-Psycho-Social Matrix ModelAMBAR JOSEFA ALEJANDRA MORAGA VALENZUELANo ratings yet
- Signs and Symptoms of Temporomandibular Joint Disorders Related To The Degree of Mouth Opening and Hearing LossDocument9 pagesSigns and Symptoms of Temporomandibular Joint Disorders Related To The Degree of Mouth Opening and Hearing LossFelipeSanzNo ratings yet
- 2021 Auriculo e ZumbidoDocument12 pages2021 Auriculo e ZumbidoNáthaly de MoraesNo ratings yet
- Deep Brain Stimulation For Refractory Tinnitus: Pilot Study Protocol For A Randomized Double-Blinded Crossover TrialDocument14 pagesDeep Brain Stimulation For Refractory Tinnitus: Pilot Study Protocol For A Randomized Double-Blinded Crossover TrialdgdgfgfNo ratings yet
- Therapeutic Approaches in BruxismDocument9 pagesTherapeutic Approaches in BruxismIlinca LupuNo ratings yet
- Y-S A 3.0PL: Organization of Multi-Specialist Medical Care and Physiotherapy For Patients With TinnitusDocument13 pagesY-S A 3.0PL: Organization of Multi-Specialist Medical Care and Physiotherapy For Patients With TinnitusPaulomds1991No ratings yet
- Effects of Emg Biofeedback On Pain and Quality of Life in Cervical Dystonia 2329 6895.1000144Document6 pagesEffects of Emg Biofeedback On Pain and Quality of Life in Cervical Dystonia 2329 6895.1000144danishmujibNo ratings yet
- The Role of Cytokines in Pulp Inflammation PDFDocument18 pagesThe Role of Cytokines in Pulp Inflammation PDFDiana Fitri MuslimahNo ratings yet
- Sleep, Health and Wellness at Work: A Scoping ReviewDocument18 pagesSleep, Health and Wellness at Work: A Scoping ReviewDhanaNo ratings yet
- Cognitive Behavioural Therapy For Insomnia (CBTi) As A Treatment For Tinnitus-Related Insomnia: Protocol For A Randomised Controlled TrialDocument11 pagesCognitive Behavioural Therapy For Insomnia (CBTi) As A Treatment For Tinnitus-Related Insomnia: Protocol For A Randomised Controlled Trialnatalia.kubickaNo ratings yet
- Coppieters IDocument15 pagesCoppieters Ihelenlamlam200011No ratings yet
- Fnins 17 1092537Document18 pagesFnins 17 1092537Helena OliveiraNo ratings yet
- Manual Therapy Combined With Functional Exercise in The Treatment of The Main Pathologies of Aging A QuantitativequalitaDocument2 pagesManual Therapy Combined With Functional Exercise in The Treatment of The Main Pathologies of Aging A QuantitativequalitaHas SimNo ratings yet
- 1 s2.0 S0022510X01005858 MainDocument9 pages1 s2.0 S0022510X01005858 MainAmbar Dani SyuhadaNo ratings yet
- Cervical Trigger Point Acupuncture For Trea - 2019 - Journal of Acupuncture andDocument4 pagesCervical Trigger Point Acupuncture For Trea - 2019 - Journal of Acupuncture andMatias DamiánNo ratings yet
- Original Article: Rizkiditia Nugraha Hadian, Renaldi Prasetia, Ahmad FariedDocument4 pagesOriginal Article: Rizkiditia Nugraha Hadian, Renaldi Prasetia, Ahmad FariedEka PutriNo ratings yet
- 201705gillespie 1Document9 pages201705gillespie 1Jose PerezNo ratings yet
- 19 Neurobehavioral Alterations in Occupational Noise Exposure A Systematic ReviewDocument22 pages19 Neurobehavioral Alterations in Occupational Noise Exposure A Systematic ReviewLeonardoMartínezNo ratings yet
- Ef Fect of Manual Approaches With Osteopathic Modality On Brain Correlates of Interoception: An fMRI StudyDocument12 pagesEf Fect of Manual Approaches With Osteopathic Modality On Brain Correlates of Interoception: An fMRI StudyTameemNo ratings yet
- Ef Fect of Manual Approaches With Osteopathic Modality On Brain Correlates of Interoception: An fMRI StudyDocument12 pagesEf Fect of Manual Approaches With Osteopathic Modality On Brain Correlates of Interoception: An fMRI StudyTameemNo ratings yet
- Analyzing Abstracts in Journal Articles - Adiwira A.W (H1A022016)Document5 pagesAnalyzing Abstracts in Journal Articles - Adiwira A.W (H1A022016)ADIWIRA AYDIN WIBOWONo ratings yet
- Acupuncture Facial ParalysisDocument9 pagesAcupuncture Facial ParalysisHaryono zhuNo ratings yet
- Physical Therapy For Adolescents With Idiopathic Scoliosis: April 2012Document39 pagesPhysical Therapy For Adolescents With Idiopathic Scoliosis: April 2012painfree888No ratings yet
- Tinnitus Heterogeneity On Auditory and Psychological Characteristics An EditorialDocument4 pagesTinnitus Heterogeneity On Auditory and Psychological Characteristics An EditorialMateus NicacioNo ratings yet
- Association of Menstrual Cycle Related Symptoms With Mood ChangesDocument2 pagesAssociation of Menstrual Cycle Related Symptoms With Mood ChangesFajar YanuarNo ratings yet
- Tinitus 4Document6 pagesTinitus 4SiFa Imah RhieshaNo ratings yet
- How Effective Are Physiotherapy Interventions in Treating People With Sciatica? A Systematic Review and Meta AnalysisDocument18 pagesHow Effective Are Physiotherapy Interventions in Treating People With Sciatica? A Systematic Review and Meta AnalysisXavi MartinezNo ratings yet
- Genicular Nerve Ablation Zeitlinger2019Document7 pagesGenicular Nerve Ablation Zeitlinger2019drjorgewtorresNo ratings yet
- On The Relationship Between Functional Hearing and DepressionDocument13 pagesOn The Relationship Between Functional Hearing and DepressionmeiciliabahariNo ratings yet
- Noise 4Document34 pagesNoise 4NIKOLAOS CHATZAKISNo ratings yet
- Noise-Induced Hearing LossDocument34 pagesNoise-Induced Hearing LossKiswah YohanaNo ratings yet
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Best Practice & Research Clinical Rheumatology: Fiona M. Blyth, Naomi NoguchiDocument9 pagesBest Practice & Research Clinical Rheumatology: Fiona M. Blyth, Naomi NoguchiGufron MustofaNo ratings yet
- Sandrine 2642023 Jabb 100168Document14 pagesSandrine 2642023 Jabb 100168Emmanuel OwonaNo ratings yet
- Bone Growth StimulationDocument13 pagesBone Growth StimulationPeter HuntNo ratings yet
- S180886941530673XDocument8 pagesS180886941530673XErick PiñerosNo ratings yet
- NFB and AnxietyDocument41 pagesNFB and AnxietyguizzocaroNo ratings yet
- Articulo Audiologia (5)Document12 pagesArticulo Audiologia (5)carolayayalaNo ratings yet
- Ijerph 17 08011Document13 pagesIjerph 17 08011AnisNo ratings yet
- Stroth 09 NeuropsycholRehabilDocument23 pagesStroth 09 NeuropsycholRehabilNicușor NeaguNo ratings yet
- Understanding The Relationship Between Cognitive Performance and Function in Daily Life After Traumatic Brain InjuryDocument11 pagesUnderstanding The Relationship Between Cognitive Performance and Function in Daily Life After Traumatic Brain InjuryKatia DjerroudNo ratings yet
- Effect of Diabetes On The Prognosis of Sudden Sensorineural Hearing Loss: Propensity Score Matching AnalysisDocument8 pagesEffect of Diabetes On The Prognosis of Sudden Sensorineural Hearing Loss: Propensity Score Matching AnalysisRizki AdhinugrohoNo ratings yet
- Muscle-Brain Communication in Pain The Key Role of MyokinesDocument11 pagesMuscle-Brain Communication in Pain The Key Role of MyokinesGrossl Schorr FernandoNo ratings yet
- 2021 Bookmatter NeuropathologySimplifiedDocument8 pages2021 Bookmatter NeuropathologySimplifiedKourosh PourramezanNo ratings yet
- Temporomandibular Disorders and Oral ParafunctionsDocument3 pagesTemporomandibular Disorders and Oral Parafunctionsd.diazNo ratings yet
- Tactile Thermal Oral Stimulation Increases The Cortical Representation of SwallowingDocument11 pagesTactile Thermal Oral Stimulation Increases The Cortical Representation of SwallowingFabiola Cerda VargasNo ratings yet
- Artigo Relação Da Microbiota e CefaleiaDocument12 pagesArtigo Relação Da Microbiota e CefaleiaJanaina Cunha Barbosa DalloNo ratings yet
- The Relationship Between Physical and Mental Health: A Mediation AnalysisDocument9 pagesThe Relationship Between Physical and Mental Health: A Mediation AnalysisFeiga MaharaniNo ratings yet
- 2013 - Kettensthoth - Six Months of Dance InterventionDocument16 pages2013 - Kettensthoth - Six Months of Dance InterventionElisabet Rodriguez BiesNo ratings yet
- Jurnal GB MeDocument4 pagesJurnal GB MeFarra JansyeNo ratings yet
- Efficacyofamulticomponent Ijerph 17 00634Document16 pagesEfficacyofamulticomponent Ijerph 17 00634peplNo ratings yet
- Biofotonica. Gonçalves 2017 J. Breath Res. 11 046006Document6 pagesBiofotonica. Gonçalves 2017 J. Breath Res. 11 046006Denise RoferNo ratings yet
- Temporomandibular Disorders and Oral Parafunctions: Mechanism, Diagnostics, and TherapyDocument118 pagesTemporomandibular Disorders and Oral Parafunctions: Mechanism, Diagnostics, and TherapyMilton quisbert paredesNo ratings yet
- Interdisciplinary Diagnostic Research For Identification of BrushismDocument6 pagesInterdisciplinary Diagnostic Research For Identification of BrushismViviane MarquesNo ratings yet
- Fphys 13 943108Document21 pagesFphys 13 943108proiectepsihologiceNo ratings yet
- Epidemiology, Diagnosis, and Treatment of Temporomandibular DisordersDocument16 pagesEpidemiology, Diagnosis, and Treatment of Temporomandibular DisordersMarwaAmerNo ratings yet
- Fnagi 09 00080Document14 pagesFnagi 09 00080loh dtrNo ratings yet
- PE-3-badminton ModuleDocument24 pagesPE-3-badminton ModuleBob Dominic DolunaNo ratings yet
- IFAS - Presentation - S2Document21 pagesIFAS - Presentation - S2Abinash BiswalNo ratings yet
- Faculty of Education: Dr. Ghanshyam Singh P.G. College, Soyepur, Lalpur, VaranasiDocument4 pagesFaculty of Education: Dr. Ghanshyam Singh P.G. College, Soyepur, Lalpur, VaranasiRajeshKumarJainNo ratings yet
- Levy - Chapter 4Document48 pagesLevy - Chapter 4ANUPAMA RAMACHANDRANNo ratings yet
- Week 1Document15 pagesWeek 1Jamaica AlejoNo ratings yet
- SnapManual PDFDocument77 pagesSnapManual PDFnaser150No ratings yet
- ASA 105: Coastal Cruising Curriculum: Prerequisites: NoneDocument3 pagesASA 105: Coastal Cruising Curriculum: Prerequisites: NoneWengerNo ratings yet
- Elite MindsDocument1 pageElite MindsShivaNo ratings yet
- Vibration Control Technology Industry (Freudenberg Schwab)Document111 pagesVibration Control Technology Industry (Freudenberg Schwab)ismailNo ratings yet
- Gian Jyoti Institute of Management and Technology, Mohali Assignment No-1 Academic Session January-May 202Document4 pagesGian Jyoti Institute of Management and Technology, Mohali Assignment No-1 Academic Session January-May 202Isha aggarwalNo ratings yet
- Intelligent Platform Management Interface Firmware, Upgrade: Operational InstructionDocument23 pagesIntelligent Platform Management Interface Firmware, Upgrade: Operational InstructionLayth WaellNo ratings yet
- APU CSLLT - 6 - Introduction To Assembly LanguageDocument23 pagesAPU CSLLT - 6 - Introduction To Assembly LanguageAli AtifNo ratings yet
- Music For BandDocument143 pagesMusic For BandTedTerroux604No ratings yet
- The Wise Old WomenDocument2 pagesThe Wise Old WomenLycoris FernandoNo ratings yet
- Attention and Effort. (1973)Document253 pagesAttention and Effort. (1973)Robert C. CasasNo ratings yet
- Anchoring BiasDocument2 pagesAnchoring Biassara collinNo ratings yet
- Present Perfect TestDocument6 pagesPresent Perfect TestMárta FábiánNo ratings yet
- Friday HeatsDocument29 pagesFriday HeatsTGrasley6273No ratings yet
- ObliCon Reviewer SMDocument111 pagesObliCon Reviewer SMJessa Marie BrocoyNo ratings yet
- Screenshot 2024-02-14 at 11.35.01 PMDocument32 pagesScreenshot 2024-02-14 at 11.35.01 PMemaantejani10No ratings yet
- Syllabus Integrated Skill 3 - k63Document8 pagesSyllabus Integrated Skill 3 - k63Lê Hồng NhungNo ratings yet
- Comp2-Cause-Effect EssayDocument4 pagesComp2-Cause-Effect Essayapi-316060728No ratings yet
- Tugas BingDocument10 pagesTugas BingAmelasNo ratings yet
- Containers For Every Need: Maersk Equipment GuideDocument12 pagesContainers For Every Need: Maersk Equipment GuideSharath RadhakrishnanNo ratings yet
- Business Income Calculation UdomDocument23 pagesBusiness Income Calculation UdomMaster Kihimbwa100% (1)