You might also like
- Antecipatory Postural AdjustmentsDocument9 pagesAntecipatory Postural AdjustmentsPedro FonsecaNo ratings yet
- Paper 1Document9 pagesPaper 1sbarahonacamilaNo ratings yet
- 13 Marchetti 380 384 Pullover Copia 3193891071Document5 pages13 Marchetti 380 384 Pullover Copia 3193891071Angelica GarciaNo ratings yet
- Journal of Electromyography and Kinesiology: Lucien Hackett, Darren Reed, Mark Halaki, Karen A. GinnDocument7 pagesJournal of Electromyography and Kinesiology: Lucien Hackett, Darren Reed, Mark Halaki, Karen A. GinnManuel Guillermo Martinez CifuentesNo ratings yet
- The Influence of Initial Posture On The Sit-To-Stand MovementDocument6 pagesThe Influence of Initial Posture On The Sit-To-Stand MovementshodhgangaNo ratings yet
- Mottram escápula1Document6 pagesMottram escápula1Elizabeth VivancoNo ratings yet
- Motion Analysis Study of A Scapular Orientation ExerciseDocument6 pagesMotion Analysis Study of A Scapular Orientation ExerciseCmmb FisioterapiaNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- Pullover PDFDocument5 pagesPullover PDFRosaneLacerdaNo ratings yet
- Elastico No OmbrosDocument9 pagesElastico No OmbrosallanboxeNo ratings yet
- Electromyographic Analysis of The Hip Extension Pattern in Visually Impaired AthletesDocument9 pagesElectromyographic Analysis of The Hip Extension Pattern in Visually Impaired AthletesVizaNo ratings yet
- 13 Marchetti 380 384pulloverDocument6 pages13 Marchetti 380 384pullovercderosasNo ratings yet
- Coo Rev Its 2008Document9 pagesCoo Rev Its 2008AdosotoNo ratings yet
- Dickie 2016Document28 pagesDickie 2016FranciscoNo ratings yet
- Neck Muscle Load Distribution in Lateral, Frontal, and Rear-End ImpactsDocument8 pagesNeck Muscle Load Distribution in Lateral, Frontal, and Rear-End ImpactsDaniela Leyton PezoaNo ratings yet
- 2010 - Manual Therapy PDFDocument5 pages2010 - Manual Therapy PDFYuzo IgarashiNo ratings yet
- JN 00581 2017Document10 pagesJN 00581 2017Lan NguyenNo ratings yet
- Larsson 1994Document8 pagesLarsson 1994pironicolas6996No ratings yet
- Load-Displacement Properties of The Human Triceps Surae Aponeurosis and Tendon in Runners and Non-RunnersDocument9 pagesLoad-Displacement Properties of The Human Triceps Surae Aponeurosis and Tendon in Runners and Non-RunnersbanditoszNo ratings yet
- Influence of GenderDocument10 pagesInfluence of Gendersateesh83No ratings yet
- Peak and Ave Rectified EMG Measures - Core Training Hibbs Et Al 2011Document10 pagesPeak and Ave Rectified EMG Measures - Core Training Hibbs Et Al 2011Magno FilhoNo ratings yet
- Kaip Reaguoja IAP Ir Pilvo Raumenys Į Dinaminį Darbą PDFDocument6 pagesKaip Reaguoja IAP Ir Pilvo Raumenys Į Dinaminį Darbą PDFJulijus MotiejunasNo ratings yet
- Human Shoulder Muscles The Function of Neuromuscular Compartments inDocument11 pagesHuman Shoulder Muscles The Function of Neuromuscular Compartments inMauro CracchioloNo ratings yet
- Tonus MuscularDocument12 pagesTonus MuscularRadu Cristian StuparNo ratings yet
- Gait Asymmetry in Patients With Limb Length DiscrepancyDocument8 pagesGait Asymmetry in Patients With Limb Length DiscrepancyPhooi Yee LauNo ratings yet
- 10.1007@s10072 019 03974 5Document8 pages10.1007@s10072 019 03974 5Barbara NoalNo ratings yet
- Multiparameter Electromyography Analysis of The Masticatory Muscle Activities in Patients With Brainstem Stroke at Different Head PositionsDocument10 pagesMultiparameter Electromyography Analysis of The Masticatory Muscle Activities in Patients With Brainstem Stroke at Different Head PositionsSairam PhysioNo ratings yet
- Lesion Flexores 2Document11 pagesLesion Flexores 2Carlos RiveraNo ratings yet
- Positive Force Feedback in Human WalkingDocument8 pagesPositive Force Feedback in Human Walkingfernando_a_gonzalezNo ratings yet
- Relevance of Motion Artifact in Electromyography Recordings During Vibration TreatmentDocument9 pagesRelevance of Motion Artifact in Electromyography Recordings During Vibration TreatmentShafayet HossainNo ratings yet
- GaitDocument8 pagesGaitPravin YadavNo ratings yet
- Control Cortical Del MovimientoDocument15 pagesControl Cortical Del MovimientoDelfina AjoNo ratings yet
- Exaggerated Interlimb Neural Coupling Following Stroke: Tiffany L. Kline, Brian D. Schmit and Derek G. KamperDocument11 pagesExaggerated Interlimb Neural Coupling Following Stroke: Tiffany L. Kline, Brian D. Schmit and Derek G. KamperArup KuntiNo ratings yet
- Muscle Activation and Local Muscular Fatigue During A 12-Minute Rotational BridgeDocument13 pagesMuscle Activation and Local Muscular Fatigue During A 12-Minute Rotational BridgeadindaNo ratings yet
- Force Irradiation Effect of Kinesiotaping On Contralateral Muscle ActivationDocument8 pagesForce Irradiation Effect of Kinesiotaping On Contralateral Muscle ActivationDaniel GuevaraNo ratings yet
- Jørgensen1988 Article ElectromyographyAndFatigueDuriDocument6 pagesJørgensen1988 Article ElectromyographyAndFatigueDuriChengyiNo ratings yet
- ChartogneEnglishPaper PDFDocument3 pagesChartogneEnglishPaper PDFJony AlexanderNo ratings yet
- ChartogneEnglishPaper PDFDocument3 pagesChartogneEnglishPaper PDFJony AlexanderNo ratings yet
- Análisis de Elementos Finitos Del Comportamiento Biomecánico de Toda La Columna Toracolumbar Con Efecto Ligamentoso.Document16 pagesAnálisis de Elementos Finitos Del Comportamiento Biomecánico de Toda La Columna Toracolumbar Con Efecto Ligamentoso.Alejandro Marcelo Samalvides PachecoNo ratings yet
- Aust JPhysiotherv 55 I 4 SzetoDocument6 pagesAust JPhysiotherv 55 I 4 SzetoomboNo ratings yet
- Adductor Magnus An EMG Investigation Into Proximal and Disctal Portions and Direction Specific ActionDocument9 pagesAdductor Magnus An EMG Investigation Into Proximal and Disctal Portions and Direction Specific ActionElaine CspNo ratings yet
- Dario Farina, Luigi Fattorini, Francesco Felici and Giancarlo FilligoiDocument12 pagesDario Farina, Luigi Fattorini, Francesco Felici and Giancarlo FilligoiJen PassilanNo ratings yet
- VOLUME MUSCULAR - Upper Limb Muscle Volumes in Adult Subjects - 2007 PDFDocument8 pagesVOLUME MUSCULAR - Upper Limb Muscle Volumes in Adult Subjects - 2007 PDFFernando De Oliveira SolimanNo ratings yet
- Hand Dominance and Motor Unit Firing BehaviorDocument10 pagesHand Dominance and Motor Unit Firing BehaviorErina NowshinNo ratings yet
- Rectus Femoris in Gait CycleDocument5 pagesRectus Femoris in Gait CycleanjelikaNo ratings yet
- Muscle Function Path Analysis Through Muscle ActivityDocument7 pagesMuscle Function Path Analysis Through Muscle ActivityWebster LimNo ratings yet
- HHS Public AccessDocument12 pagesHHS Public AccessPablo FonsecaNo ratings yet
- Effect of Isometric Horizontal Abduction On Pectoralis Major and Serratus AnteriorDocument7 pagesEffect of Isometric Horizontal Abduction On Pectoralis Major and Serratus AnteriorRudolfGerNo ratings yet
- Journal of BiomechanicsDocument10 pagesJournal of BiomechanicsjothiNo ratings yet
- Spinal Myo After InjuryDocument12 pagesSpinal Myo After InjuryVincentius Michael WilliantoNo ratings yet
- Leer Sí o SíDocument9 pagesLeer Sí o SíAngelika Carolina Pineda JuncoNo ratings yet
- Region Specific Patellar Tendon Hypertrophy in Humans Following Resistance TrainingDocument11 pagesRegion Specific Patellar Tendon Hypertrophy in Humans Following Resistance TrainingRosaneLacerdaNo ratings yet
- Adl Upper LimbDocument8 pagesAdl Upper LimbTirumala RaoNo ratings yet
- Van Der FitsDocument15 pagesVan Der Fitsdrodelo123No ratings yet
- Influence of The Side of Brain Damage On Postural Upper-Limb Control Including The Scapula in Stroke PatientsDocument15 pagesInfluence of The Side of Brain Damage On Postural Upper-Limb Control Including The Scapula in Stroke Patientspokharelriwaj82No ratings yet
- Effects of Scapular Taping in Young Adults With Shoulder Pain and Scapular DyskinesisDocument8 pagesEffects of Scapular Taping in Young Adults With Shoulder Pain and Scapular DyskinesisFrancisco Javier Luza RamosNo ratings yet
- 0717 9502 Ijmorphol 39 01 205Document6 pages0717 9502 Ijmorphol 39 01 205VITOR PEREZNo ratings yet
- Anatomy and Human Movement: Structure and FunctionFrom EverandAnatomy and Human Movement: Structure and FunctionRating: 3.5 out of 5 stars3.5/5 (2)
- Electromyography in CNS Disorders: Central EMGFrom EverandElectromyography in CNS Disorders: Central EMGBhagwan T. ShahaniNo ratings yet
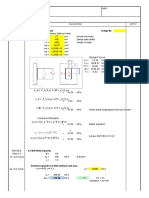
- Weld Check: I. Connection Properties Bridge IDDocument3 pagesWeld Check: I. Connection Properties Bridge IDJemicah YumenaNo ratings yet
- Mock Teaching Lesson PlanDocument2 pagesMock Teaching Lesson Planapi-354968419No ratings yet
- Lab 02-Center of The Galaxy LabDocument7 pagesLab 02-Center of The Galaxy LabBNo ratings yet
- Carlo Gavazzi Small CatDocument226 pagesCarlo Gavazzi Small CatkcraussNo ratings yet
- PT SURYA CITRA INTI SEMESTA PROJECT REFERENCE LISTDocument1 pagePT SURYA CITRA INTI SEMESTA PROJECT REFERENCE LISTAgus RiyanaNo ratings yet
- Fish Bowl Strategy: Fishbowl Is A Strategy For Organizing Medium-To Large-Group Discussions. Students AreDocument2 pagesFish Bowl Strategy: Fishbowl Is A Strategy For Organizing Medium-To Large-Group Discussions. Students AreAllysa Marie BorladoNo ratings yet
- Lesson 1 - PMP Authorized Exam Prep - V3 - Business EnvironmentDocument105 pagesLesson 1 - PMP Authorized Exam Prep - V3 - Business EnvironmentmaiyomarionneNo ratings yet
- Annex 15 QC Inspection ReportDocument2 pagesAnnex 15 QC Inspection ReportEl LlacunaNo ratings yet
- Chapter 12 PracticeDocument2 pagesChapter 12 PracticeSarah ViscoNo ratings yet
- Rising Strong: How The Ability To Reset Transforms The Way We Live, Love, Parent, and Lead - Brené BrownDocument5 pagesRising Strong: How The Ability To Reset Transforms The Way We Live, Love, Parent, and Lead - Brené Browndarupasi40% (5)
- APPLICATION OF COMPUTERS IN PHARMACY MANAGEMENT AND SERVICESDocument109 pagesAPPLICATION OF COMPUTERS IN PHARMACY MANAGEMENT AND SERVICESvarishNo ratings yet
- Lesson Plan: Industrial University of Ho Chi Minh CityDocument10 pagesLesson Plan: Industrial University of Ho Chi Minh CityNguyễn TrangNo ratings yet
- Optimization of Trig Functions Part 2: Periods, Speeds & AnglesDocument5 pagesOptimization of Trig Functions Part 2: Periods, Speeds & AnglesFaye CaiNo ratings yet
- PCS-974A-G X Instruction Manual en Domestic General X R1.10Document194 pagesPCS-974A-G X Instruction Manual en Domestic General X R1.10Hikari DewiNo ratings yet
- Map Work: Types of MapsDocument18 pagesMap Work: Types of Mapshussain korirNo ratings yet
- Redevelopment of Machhabhaudi, Dharan, Sunsari: Project ProposalDocument10 pagesRedevelopment of Machhabhaudi, Dharan, Sunsari: Project Proposaldiwas baralNo ratings yet
- JNTUK - Revised Syllabus For M. Tech Transportation EngineeringDocument20 pagesJNTUK - Revised Syllabus For M. Tech Transportation Engineeringvamsi_rsNo ratings yet
- Histogram: Nonparametric Kernel Density EstimationDocument19 pagesHistogram: Nonparametric Kernel Density Estimationsabeeh iqbalNo ratings yet
- Seismic Force CANADA Code - CNBC2005-V421Document7 pagesSeismic Force CANADA Code - CNBC2005-V421Niko NištićNo ratings yet
- Guide For The Use of Educational Resources - Software Smith V4.0Document7 pagesGuide For The Use of Educational Resources - Software Smith V4.0Sebastián Barona VélezNo ratings yet
- Unit 7 VocabularyDocument2 pagesUnit 7 VocabularyNy MenghongNo ratings yet
- YIELD STABILITYDocument7 pagesYIELD STABILITYgagaNo ratings yet
- V2k (Voice To Skull: Download Free PDFDocument43 pagesV2k (Voice To Skull: Download Free PDFLazlo SecretNo ratings yet
- Plant Pathology Curriculum Revised for BSc, MSc and PhD DegreesDocument90 pagesPlant Pathology Curriculum Revised for BSc, MSc and PhD Degreesjahangir khanNo ratings yet
- Subculture The Meaning of StyleDocument3 pagesSubculture The Meaning of StyleMandic SutomoreNo ratings yet
- Veterinary Epidemiology Study QuestionsDocument13 pagesVeterinary Epidemiology Study Questionsthechickendidwhat33% (3)
- Eltorai, Ibrahim M A Spotlight On The History of Ancient EgyptianDocument215 pagesEltorai, Ibrahim M A Spotlight On The History of Ancient EgyptianJonas PsontomfanceNo ratings yet
- Catalogo General MAGPOWRDocument16 pagesCatalogo General MAGPOWRananda.slp.admonNo ratings yet
- BQ3 - UnknownDocument3 pagesBQ3 - UnknownAnkitNo ratings yet
- FirePro Product Catalogue 2022Document91 pagesFirePro Product Catalogue 2022OMATSEYE OLUKPENo ratings yet