You might also like
- Cognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationFrom EverandCognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationMark MuseNo ratings yet
- BJP BP 115 171397 FullDocument11 pagesBJP BP 115 171397 FullWilly Kusmana Junior Part IINo ratings yet
- Effectiveness of Psychotherapy For Severe Somatoform Disorder: Meta-AnalysisDocument14 pagesEffectiveness of Psychotherapy For Severe Somatoform Disorder: Meta-AnalysisDarmawanNo ratings yet
- JURNAL 2 Augmentation Strategies For Treatment-Resistant Anxiety Disorders A Systematic Review and Meta-Analysis-dikonversiDocument15 pagesJURNAL 2 Augmentation Strategies For Treatment-Resistant Anxiety Disorders A Systematic Review and Meta-Analysis-dikonversiNixal KurniawanNo ratings yet
- A Systematic Scoping Review of Psychological Therapies For Psychosis Within Acute Psychiatric In-Patient Settings.Document8 pagesA Systematic Scoping Review of Psychological Therapies For Psychosis Within Acute Psychiatric In-Patient Settings.Eric KatškovskiNo ratings yet
- Research 3Document12 pagesResearch 3Pratxxm PatelNo ratings yet
- Cognitive Behavioral Therapy For Medication-Resistant Psychosis A Metanalytic ReviewDocument7 pagesCognitive Behavioral Therapy For Medication-Resistant Psychosis A Metanalytic Reviewjenny082600No ratings yet
- CBT Video Therapy Effective For Psychiatric DisordersDocument16 pagesCBT Video Therapy Effective For Psychiatric DisorderslaiaNo ratings yet
- Pi Is 2215036616303789Document11 pagesPi Is 2215036616303789U of T MedicineNo ratings yet
- Background: Lancet Psychiatry 2017Document11 pagesBackground: Lancet Psychiatry 2017Manya DhuparNo ratings yet
- Short-Term Psychodynamic Psychotherapy For Somatic DisordersDocument10 pagesShort-Term Psychodynamic Psychotherapy For Somatic Disordersscribd4kmhNo ratings yet
- Omj D 17 00061Document8 pagesOmj D 17 00061Riska Resty WasitaNo ratings yet
- Eca MBCT en TocDocument11 pagesEca MBCT en TocMiriam JaraNo ratings yet
- Mindfulness Training in A Heterogeneous Psychiatric Sample: Outcome Evaluation and Comparison of Different Diagnostic GroupsDocument13 pagesMindfulness Training in A Heterogeneous Psychiatric Sample: Outcome Evaluation and Comparison of Different Diagnostic Groups290971No ratings yet
- Efficacy For Treatment Anxiety DisordersDocument10 pagesEfficacy For Treatment Anxiety DisordersAnderson GaldinoNo ratings yet
- Mental DisordersDocument10 pagesMental Disordersapi-261131330No ratings yet
- Jurnal InsomiaDocument20 pagesJurnal InsomiaUtomo FemtomNo ratings yet
- Out 6Document8 pagesOut 6ayulitadewiNo ratings yet
- 128 FullDocument9 pages128 FullAhtarunnisa Fauzia HanifaNo ratings yet
- Cuijpers et al., (2021)Document11 pagesCuijpers et al., (2021)Jonathan PitreNo ratings yet
- Clinical Research Articles Assignment 4Document9 pagesClinical Research Articles Assignment 4Awais. anwarNo ratings yet
- PA y Depresión en Nepal 2017Document8 pagesPA y Depresión en Nepal 2017Alfredo PérezNo ratings yet
- The Effects of Auditory Hallucination Symptom ManagementDocument12 pagesThe Effects of Auditory Hallucination Symptom ManagementAndika FahruroziNo ratings yet
- Complementary Therapies in Clinical PracticeDocument7 pagesComplementary Therapies in Clinical PracticeBkash ShahNo ratings yet
- Disorders: Update of A Meta-Analysis Long-Term Psychodynamic Psychotherapy in Complex MentalDocument9 pagesDisorders: Update of A Meta-Analysis Long-Term Psychodynamic Psychotherapy in Complex MentalJuan Diego González BustilloNo ratings yet
- Eca MBCTDocument12 pagesEca MBCTMiriam JaraNo ratings yet
- 2.psilocybin-Assisted Therapy For Depression A Systematic Review and Dose-Response Meta-Analysis of Human StudiesDocument16 pages2.psilocybin-Assisted Therapy For Depression A Systematic Review and Dose-Response Meta-Analysis of Human StudiesMarcos MouraNo ratings yet
- Edited By: Dr. Javaid Akhtar, MCPS, FCPS, Head Of: Search StrategyDocument3 pagesEdited By: Dr. Javaid Akhtar, MCPS, FCPS, Head Of: Search StrategyKaram Ali ShahNo ratings yet
- Mindfulness-Based Stress Reduction and Health Benefits A Meta-AnalysisDocument9 pagesMindfulness-Based Stress Reduction and Health Benefits A Meta-AnalysisVladNo ratings yet
- Ecam2015 792895Document8 pagesEcam2015 792895Meri Fitria HandayaniNo ratings yet
- Effectiveness of Cognitive-Behavioural Group Therapy in Patients With Anxiety DisordersDocument9 pagesEffectiveness of Cognitive-Behavioural Group Therapy in Patients With Anxiety DisordersCris NavaNo ratings yet
- Chu y Vieta 2018Document12 pagesChu y Vieta 2018290971No ratings yet
- Does Mindfulness Improve Outcomes in Patients With Chronic PainDocument14 pagesDoes Mindfulness Improve Outcomes in Patients With Chronic Painiker1303No ratings yet
- BMC PsychiatryDocument7 pagesBMC Psychiatryyeremias setyawanNo ratings yet
- Grepmair Et Al. (2007) Promoting Mindfulness in PsychoterapyDocument7 pagesGrepmair Et Al. (2007) Promoting Mindfulness in PsychoterapyVania Aguilera ArriagadaNo ratings yet
- A Randomized Controlled Trial of A Mindfulness-Based Intervention Program For People With Schizophrenia: 6-Month Follow-UpDocument14 pagesA Randomized Controlled Trial of A Mindfulness-Based Intervention Program For People With Schizophrenia: 6-Month Follow-UpOrion OriNo ratings yet
- Resmume Jurnal JiwaDocument3 pagesResmume Jurnal Jiwaanj arNo ratings yet
- Psych TestsDocument27 pagesPsych TestsMada MadalinuNo ratings yet
- Jurnal 6Document13 pagesJurnal 6dewi pspta sriNo ratings yet
- Kayo 2020Document3 pagesKayo 2020Jauhari AttabraniNo ratings yet
- Acta Psychiatr Scand 2011Document10 pagesActa Psychiatr Scand 2011Toon ToonannNo ratings yet
- May 09 Journals (Mostly) : 63 AbstractsDocument14 pagesMay 09 Journals (Mostly) : 63 AbstractssunkissedchiffonNo ratings yet
- 2000 MICHAEL SPECA - A Randomized, Wait-List Controlled Clinical Trial The Effect of A MindfulnessDocument10 pages2000 MICHAEL SPECA - A Randomized, Wait-List Controlled Clinical Trial The Effect of A Mindfulnessnermal93No ratings yet
- Zhou 2020Document8 pagesZhou 2020Rosalía PattyNo ratings yet
- Efficacy of Psychological Intervention For Patients With Psoriasis Vulgaris: A Prospective StudyDocument8 pagesEfficacy of Psychological Intervention For Patients With Psoriasis Vulgaris: A Prospective StudyTeuku FadhliNo ratings yet
- Efecto de Programa de 12 Sesiones de Psicoeducación, Mindfulness Basada en Terapia Cognitiva, Remediación Funcional para Trastornos BipolararesDocument9 pagesEfecto de Programa de 12 Sesiones de Psicoeducación, Mindfulness Basada en Terapia Cognitiva, Remediación Funcional para Trastornos BipolararesGiorgio AgostiniNo ratings yet
- Treating Somatization: A Multimodal ApproachDocument7 pagesTreating Somatization: A Multimodal ApproachDr. Ranjan KumarNo ratings yet
- Pharmacophore: Nazanin Farrokhi, Fatemeh Yousefzadeh, Mir Majid Saeedi, Leila Behnam, Shahrbanoo GhahariDocument8 pagesPharmacophore: Nazanin Farrokhi, Fatemeh Yousefzadeh, Mir Majid Saeedi, Leila Behnam, Shahrbanoo GhahariDestri DhelianaNo ratings yet
- Zanelloetal 2006Document15 pagesZanelloetal 2006jk rNo ratings yet
- Review ArticleDocument9 pagesReview ArticleMuhammad YanazNo ratings yet
- Meta Analysis On The Efficacy of Psychological Treatments For Anorexia NervosaDocument21 pagesMeta Analysis On The Efficacy of Psychological Treatments For Anorexia NervosaGanellNo ratings yet
- Intro:: Chapter 6 - Clinical Trials in Substance Using PopulationsDocument4 pagesIntro:: Chapter 6 - Clinical Trials in Substance Using PopulationsVanNo ratings yet
- Lynch Et Al (2013)Document17 pagesLynch Et Al (2013)Valerie Walker LagosNo ratings yet
- StubbsDocument15 pagesStubbsjasonNo ratings yet
- Cognitive-Behavioral Therapy For Somatization Disorder: A Randomized Controlled TrialDocument7 pagesCognitive-Behavioral Therapy For Somatization Disorder: A Randomized Controlled TrialMuhammad Bayu WNo ratings yet
- Physiotherapy Improves Eating Disorders and Quality of Life in Bulimia and Anorexia NervosaDocument3 pagesPhysiotherapy Improves Eating Disorders and Quality of Life in Bulimia and Anorexia NervosaAzul MarinoNo ratings yet
- Metaanalisis CBT Vs TauDocument14 pagesMetaanalisis CBT Vs TauIndrawaty SuhuyanliNo ratings yet
- Physical Exercise and iCBT in Treatment of DepressionDocument9 pagesPhysical Exercise and iCBT in Treatment of DepressionCarregan AlvarezNo ratings yet
- Efficacy of Cognitive Behaviour Therapy in ManagementDocument5 pagesEfficacy of Cognitive Behaviour Therapy in ManagementIrfan FauziNo ratings yet
- La Rehabilitación Integral Del Paciente Esquizofrénico en México El Modelo Del Instituto Nacional de Psiquiatría Ramón de La FuenteDocument11 pagesLa Rehabilitación Integral Del Paciente Esquizofrénico en México El Modelo Del Instituto Nacional de Psiquiatría Ramón de La FuenteLuisVicenteJimenezGarciaNo ratings yet
- Grade 11 - Final Exam PDDocument3 pagesGrade 11 - Final Exam PDGomez Agustin LeslieNo ratings yet
- 1023 3581 1 PBDocument4 pages1023 3581 1 PBfitriNo ratings yet
- Components of Argumentative EssayDocument13 pagesComponents of Argumentative EssaySheia Jinx75% (4)
- The Hall Technique 10 Years On: Questions and Answers: GeneralDocument6 pagesThe Hall Technique 10 Years On: Questions and Answers: GeneralamilescoNo ratings yet
- AugustDocument6 pagesAugustchathurika dulanjaliNo ratings yet
- Lecture 3.2.3: Erection III: Steel Construction: Fabrication and ErectionDocument4 pagesLecture 3.2.3: Erection III: Steel Construction: Fabrication and ErectionMihajloDjurdjevicNo ratings yet
- 18.20.04 - BSSL Seafarers Health Self Declaration With COVID 19 Test And... (1) - 3Document3 pages18.20.04 - BSSL Seafarers Health Self Declaration With COVID 19 Test And... (1) - 3Dean IL RE JamesNo ratings yet
- End of Life Care GuideDocument79 pagesEnd of Life Care GuideAbcd TolibasNo ratings yet
- SPTL Ohs&e 40 Ohse MPR AbrarDocument22 pagesSPTL Ohs&e 40 Ohse MPR AbrarRanjeet Kumar SinghNo ratings yet
- Marie Stopes International ReportDocument8 pagesMarie Stopes International ReportAustin DeneanNo ratings yet
- Yahoo News You Gov Health Poll 3.11.24Document13 pagesYahoo News You Gov Health Poll 3.11.24AndrewNo ratings yet
- Pharmacology Course IntroductionDocument2 pagesPharmacology Course IntroductionHassen ZabalaNo ratings yet
- HS ConsultantDocument2 pagesHS Consultantdeeman4yahNo ratings yet
- Course Outline PBH 101 MW 18Document7 pagesCourse Outline PBH 101 MW 18FAYAZ AHMEDNo ratings yet
- Decision Making and Situational Awareness in Neonatal Resuscitation in Low Resource SettingsDocument8 pagesDecision Making and Situational Awareness in Neonatal Resuscitation in Low Resource SettingsJessica MatosNo ratings yet
- Clinical Handbook of Psychotropic Drugs, 25e (May 8, 2023)_(0889376328)_(Hogrefe Publishing) ( Etc.) (Z-Library)Document555 pagesClinical Handbook of Psychotropic Drugs, 25e (May 8, 2023)_(0889376328)_(Hogrefe Publishing) ( Etc.) (Z-Library)Dragutin PetrićNo ratings yet
- 2 NdresearchpaperDocument5 pages2 Ndresearchpaperapi-356685046No ratings yet
- Personal Values, Beliefs and AttitudesDocument10 pagesPersonal Values, Beliefs and Attitudesapi-282066793No ratings yet
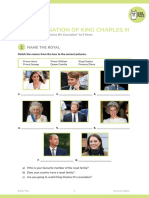
- SV The Coronation of King Charles IIIDocument9 pagesSV The Coronation of King Charles IIIMaria GromovaNo ratings yet
- How To Negotiate With Nursing Authority Figures (Rough)Document2 pagesHow To Negotiate With Nursing Authority Figures (Rough)Meet DandiwalNo ratings yet
- Best Body FitnessDocument3 pagesBest Body FitnessLavinia Chirila-StefanutNo ratings yet
- Welfare and Development Section (WDS)Document6 pagesWelfare and Development Section (WDS)Darwin Patricio100% (1)
- JIDMR SCOPUS Ke 4 Anwar MallongiDocument4 pagesJIDMR SCOPUS Ke 4 Anwar Mallongiadhe yuniarNo ratings yet
- Teenage Pregnancy Refers To The Adolescent Girls, Usually With in The AgesDocument6 pagesTeenage Pregnancy Refers To The Adolescent Girls, Usually With in The Agesmarina abanNo ratings yet
- ItDocument4 pagesItNguyễn Duy HuânNo ratings yet
- Presentation 1Document6 pagesPresentation 1Joarlin BianesNo ratings yet
- Cattle Annual Cow Cost SpreadsheetDocument4 pagesCattle Annual Cow Cost SpreadsheetSushil JangirNo ratings yet
- January 2022 BehavioursDocument8 pagesJanuary 2022 Behavioursdhopat kalpeshNo ratings yet
- Unit 6 Progress Test - Key Vocabulary and Grammar ConceptsDocument2 pagesUnit 6 Progress Test - Key Vocabulary and Grammar ConceptsKatren OrobchukNo ratings yet
- HSE and SOP ON EMBARKATIONDocument5 pagesHSE and SOP ON EMBARKATIONNajmirzan IsraNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (1)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItFrom EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (84)
- Call of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodFrom EverandCall of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodNo ratings yet
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- The Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressFrom EverandThe Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressNo ratings yet
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Emotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyFrom EverandEmotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyRating: 5 out of 5 stars5/5 (6)
- The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk: Key Takeaways, Summary & AnalysisFrom EverandThe Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (2)