You might also like
- OVPR FY20Q1 Proposal List PDFDocument45 pagesOVPR FY20Q1 Proposal List PDFtsuregiNo ratings yet
- Topical Reviews in Neurosurgery: Volume 1From EverandTopical Reviews in Neurosurgery: Volume 1J. M. Rice EdwardsNo ratings yet
- Barangay Staff Accomplishment Report New LHDocument2 pagesBarangay Staff Accomplishment Report New LHUy HenryNo ratings yet
- MARS2 ProjectDocument9 pagesMARS2 ProjectuniportalvatsmexicoNo ratings yet
- Limited Resection For Early-Stage Thymoma - Minimally Invasive Resection Does Not Mean Limited ResectionDocument7 pagesLimited Resection For Early-Stage Thymoma - Minimally Invasive Resection Does Not Mean Limited ResectionJason HuangNo ratings yet
- Aesculap Ds Appendectomy ClipDocument12 pagesAesculap Ds Appendectomy ClipdoniNo ratings yet
- 1 s2.0 S1015958421002621 MainDocument6 pages1 s2.0 S1015958421002621 MainLuiz Antônio PeratoneNo ratings yet
- Minimal Invasiveness in Soft Tissue Augmentation at Dental Implants A Systematic Review and Meta-Analysis of Patient-Reported OutcomeDocument17 pagesMinimal Invasiveness in Soft Tissue Augmentation at Dental Implants A Systematic Review and Meta-Analysis of Patient-Reported Outcomemahesh kumarNo ratings yet
- Endoscopic Submucosal Dissection For Early Gastric Cancer: Are Expanded Resection Criteria Safe For Western Patients?Document11 pagesEndoscopic Submucosal Dissection For Early Gastric Cancer: Are Expanded Resection Criteria Safe For Western Patients?Mayra Camila PerezNo ratings yet
- Evaluating The Impact of Technique and Mesh Type in Complicated Ventral Hernia Repair: A Prospective Randomized Multicenter Controlled TrialDocument14 pagesEvaluating The Impact of Technique and Mesh Type in Complicated Ventral Hernia Repair: A Prospective Randomized Multicenter Controlled TrialDaniela Cortez RojasNo ratings yet
- Surgical Approaches To Colonic and Rectal Anastomosis: Systematic Review and Meta AnalysisDocument24 pagesSurgical Approaches To Colonic and Rectal Anastomosis: Systematic Review and Meta AnalysisCamilla FariasNo ratings yet
- 268 2013 Article 2080Document13 pages268 2013 Article 2080Carlos HernándezNo ratings yet
- Long-Term Results of a Randomized Trial on Prophylactic Intraperitoneal Mesh for Midline Incisional Hernia PreventionDocument7 pagesLong-Term Results of a Randomized Trial on Prophylactic Intraperitoneal Mesh for Midline Incisional Hernia PreventiondrpklalNo ratings yet
- Research ArticleDocument6 pagesResearch Articlepolomska.kmNo ratings yet
- Tang 2021Document8 pagesTang 2021Erick JaenNo ratings yet
- Video-Assisted Thoracoscopic Surgery For Early Evacuation of Traumatic Clotted HemothoracesDocument6 pagesVideo-Assisted Thoracoscopic Surgery For Early Evacuation of Traumatic Clotted Hemothoracesdella oktavianiNo ratings yet
- Short Term Outcomes D3 VS D2 LRHDocument11 pagesShort Term Outcomes D3 VS D2 LRHJoaquin Martinez HernandezNo ratings yet
- Analyzing Contraction of Full Thickness Skin Grafts in Time: Choosing The Donor Site Does MatterDocument6 pagesAnalyzing Contraction of Full Thickness Skin Grafts in Time: Choosing The Donor Site Does MatterFelix Hadi NainggolanNo ratings yet
- Small Intestine Anastomosis by Full Thickness, Single Layer and Interrupted Suture Technique: Results of A Comparative StudyDocument4 pagesSmall Intestine Anastomosis by Full Thickness, Single Layer and Interrupted Suture Technique: Results of A Comparative StudyS3V4_9154No ratings yet
- 10 1016@j Jamcollsurg 2020 02 031Document34 pages10 1016@j Jamcollsurg 2020 02 031Residentes Cirugia Udea 2016No ratings yet
- International Journal of Surgery Case ReportsDocument5 pagesInternational Journal of Surgery Case Reportscarlos javier andraadeNo ratings yet
- Tsaco 2022 000980Document6 pagesTsaco 2022 000980Dani AlfariziNo ratings yet
- armijo2020Document7 pagesarmijo2020Yeudiel SuroNo ratings yet
- Terapia de Vacio en TraumaDocument11 pagesTerapia de Vacio en TraumaImha MikanersandsmashblastNo ratings yet
- Pancreatic SurgeryDocument5 pagesPancreatic SurgeryFlaviu Ionuț FaurNo ratings yet
- 2018 Article 6554Document8 pages2018 Article 6554Raíla SoaresNo ratings yet
- Mesh Fixation Technique in Totally Extraperitoneal Inguinal Hernia Repair e A Network Meta-AnalysisDocument10 pagesMesh Fixation Technique in Totally Extraperitoneal Inguinal Hernia Repair e A Network Meta-AnalysisFatahNo ratings yet
- Homemade Mitral RingDocument4 pagesHomemade Mitral Ringadel husseinNo ratings yet
- Comparison of The Short-Term Outcomes of Using DST and PPH Staplers in The Treatment of Grade Iii and Iv HemorrhoidsDocument7 pagesComparison of The Short-Term Outcomes of Using DST and PPH Staplers in The Treatment of Grade Iii and Iv HemorrhoidsdianisaindiraNo ratings yet
- Clamping Trials Prior To Thoracostomy Tube Removal and The Need For Subsequent Invasive Pleural DrainageDocument6 pagesClamping Trials Prior To Thoracostomy Tube Removal and The Need For Subsequent Invasive Pleural Drainagelutfor rahmanNo ratings yet
- Comparing Erector Spinae Plane Block With Serratus Anterio - 2020 - British JourDocument9 pagesComparing Erector Spinae Plane Block With Serratus Anterio - 2020 - British JourtasyadelizaNo ratings yet
- Laparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceDocument5 pagesLaparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceMudassar SattarNo ratings yet
- Fendo 13 921812Document8 pagesFendo 13 921812ivan dario hernandez erazoNo ratings yet
- To Drain or Not To Drain 1700829907Document13 pagesTo Drain or Not To Drain 1700829907qpv5pfz2bkNo ratings yet
- JPM 12 00512Document16 pagesJPM 12 00512Muhammad RifkiNo ratings yet
- Swanson 2007Document5 pagesSwanson 2007Giancarlo Maruri MunarettoNo ratings yet
- f194 DikonversiDocument5 pagesf194 DikonversiFarizka Dwinda HNo ratings yet
- Choi et al., 2020Document8 pagesChoi et al., 2020NyomantrianaNo ratings yet
- Efficacy of Minimally Invasive Surgery On Giant Cell Tumor of The Bone: A Systematic ReviewDocument14 pagesEfficacy of Minimally Invasive Surgery On Giant Cell Tumor of The Bone: A Systematic ReviewAnonymous MLXWLzNo ratings yet
- Immobilisation FFFDocument8 pagesImmobilisation FFFSrinivas VenkataramanNo ratings yet
- A Comparative Study of Complic PDFDocument6 pagesA Comparative Study of Complic PDFBeatrice TanudjajaNo ratings yet
- Is Surgical Treatment Based On A 1-Step or 2-Step Protocol Effective in Managing The Odontogenic Keratocyst?Document7 pagesIs Surgical Treatment Based On A 1-Step or 2-Step Protocol Effective in Managing The Odontogenic Keratocyst?shehla khanNo ratings yet
- E041797 FullDocument11 pagesE041797 FullDewi Purnama SariNo ratings yet
- Decision Algỏithm and Surgical Strategies For Managing Trachecutaneous FistulaDocument9 pagesDecision Algỏithm and Surgical Strategies For Managing Trachecutaneous Fistulahai1No ratings yet
- Comparing TH Staple LineDocument4 pagesComparing TH Staple LineJulio Adan Campos BadilloNo ratings yet
- Impact of Time To Surgery After Neoadjuvant Chemotherapy in Operable Breast Cancer PatientsDocument6 pagesImpact of Time To Surgery After Neoadjuvant Chemotherapy in Operable Breast Cancer PatientsPani lookyeeNo ratings yet
- Eano GlioblastomaDocument10 pagesEano GlioblastomaMEILYN MEDINA FAÑANo ratings yet
- Influence of Kinesiologic Tape On Post-Operative Swelling After Orthognathic SurgeryDocument7 pagesInfluence of Kinesiologic Tape On Post-Operative Swelling After Orthognathic SurgeryGisele DiasNo ratings yet
- Safety of Robotic Thyroidectomy Approaches: Meta-Analysis and Systematic ReviewDocument7 pagesSafety of Robotic Thyroidectomy Approaches: Meta-Analysis and Systematic Reviewcabeza y cuello incNo ratings yet
- PD Catheter Insertion Technique OutcomesDocument7 pagesPD Catheter Insertion Technique OutcomesRocci Jack ParseNo ratings yet
- Reconstruccion MamariaDocument9 pagesReconstruccion MamariadiogenesNo ratings yet
- Does Elastic Therapeutic Tape ReduceDocument10 pagesDoes Elastic Therapeutic Tape ReducegreynerNo ratings yet
- 10.1186@s12891 020 03579 6Document6 pages10.1186@s12891 020 03579 6Han's OfficialNo ratings yet
- 1 s2.0 S2468294221000605 MainDocument7 pages1 s2.0 S2468294221000605 MainVishal BasuNo ratings yet
- Casali 2009Document6 pagesCasali 2009Giancarlo Maruri MunarettoNo ratings yet
- Comparing Robotic and Trans-Sternal Thymectomy For Early-Stage Thymoma - A Propensity Score-Matching Study.Document6 pagesComparing Robotic and Trans-Sternal Thymectomy For Early-Stage Thymoma - A Propensity Score-Matching Study.Jason HuangNo ratings yet
- Antibiotic-Impregnated PMMA Hip Spacers: Current StatusDocument10 pagesAntibiotic-Impregnated PMMA Hip Spacers: Current StatusChrysi TsiouriNo ratings yet
- Impact of Surgical Margins On Overall Survival After Gastrectomy For Gastric Cancer: A Validation of Japanese Gastric Cancer Association Guidelines On A Western SeriesDocument13 pagesImpact of Surgical Margins On Overall Survival After Gastrectomy For Gastric Cancer: A Validation of Japanese Gastric Cancer Association Guidelines On A Western SeriesХулан ХүрэлбаатарNo ratings yet
- PDF JTN 2170Document9 pagesPDF JTN 2170RathavishwarajNo ratings yet
- Bae et al., 2018Document12 pagesBae et al., 2018NyomantrianaNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024Document4 pagesVolume: 05 Issue: 01 - Jan-Feb 2024Central Asian StudiesNo ratings yet
- Ca Thyroid Papilary Total Tiroidektomi Atau Istmolobektomi SajaDocument6 pagesCa Thyroid Papilary Total Tiroidektomi Atau Istmolobektomi Sajaahmad iffa maududyNo ratings yet
- PASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceDocument2 pagesPASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceJhigo Villar Franco PascualNo ratings yet
- Rizal To Paris To GermanyDocument48 pagesRizal To Paris To Germanybenj panganibanNo ratings yet
- Clobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023Document51 pagesClobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023veerraju tvNo ratings yet
- Laporan Jaga Perina Selasa Malam EditDocument15 pagesLaporan Jaga Perina Selasa Malam EditmuhammadrikiNo ratings yet
- Guidelines for diagnosing and treating hypothyroidismDocument43 pagesGuidelines for diagnosing and treating hypothyroidismJoseAbdalaNo ratings yet
- Clinical Efficiency of Three Caries Removal Systems: Rotary Excavation, Carisolv, and PapacarieDocument8 pagesClinical Efficiency of Three Caries Removal Systems: Rotary Excavation, Carisolv, and PapacarieVianney Guadalupe González ElizaldeNo ratings yet
- Skilled Birth Attendant (SBA) : State Institute of Health & Family Welfare JaipurDocument32 pagesSkilled Birth Attendant (SBA) : State Institute of Health & Family Welfare JaipurDurga NaikNo ratings yet
- A Survey On Data Mining Techniques For COVID PredictionDocument6 pagesA Survey On Data Mining Techniques For COVID PredictionWARSE Journals100% (2)
- Primary Sclerosing Cholangitis-JR KrisnaDocument16 pagesPrimary Sclerosing Cholangitis-JR Krisnamerlyn angelinaNo ratings yet
- Child Health COURSE PLAN M.SC 2 YEARDocument49 pagesChild Health COURSE PLAN M.SC 2 YEARSanthosh.S.UNo ratings yet
- Understand the Difference Between Omega-3 EPA and DHADocument7 pagesUnderstand the Difference Between Omega-3 EPA and DHASutanto TanakaNo ratings yet
- Material Safety Data Sheet - NITRIC ACID PDFDocument9 pagesMaterial Safety Data Sheet - NITRIC ACID PDFJunaid AhmadNo ratings yet
- Surgical SeiveDocument28 pagesSurgical SeiveSumeet PratapNo ratings yet
- Anti - HyperlipidemiaDocument18 pagesAnti - HyperlipidemiaZakarie Abdullahi Hussein100% (1)
- Fast Weight Loss TipsDocument2 pagesFast Weight Loss TipsLenny AnsirNo ratings yet
- Nauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewDocument19 pagesNauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewMichael Kwesi BaahNo ratings yet
- 1167 1864 1 SMDocument5 pages1167 1864 1 SMMujahid FajrulNo ratings yet
- Viastar Blue Oral Dissolving Film 50 MG - Sildenafil Sitrat - DKI1953300196A1 - 2019Document17 pagesViastar Blue Oral Dissolving Film 50 MG - Sildenafil Sitrat - DKI1953300196A1 - 2019RIRINo ratings yet
- Rabbithematology PDFDocument12 pagesRabbithematology PDFHuda HudaNo ratings yet
- Does Masturbation Cause Acne in Men?Document3 pagesDoes Masturbation Cause Acne in Men?AndyJenkinsNo ratings yet
- Resume About NoiseDocument5 pagesResume About NoiseElsa MutiaraNo ratings yet
- SAS 6 - Abapo, Aquea B.Document5 pagesSAS 6 - Abapo, Aquea B.Aquea Bernardo AbapoNo ratings yet
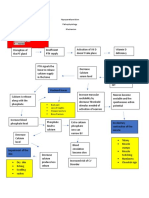
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Khatib2017 PDFDocument14 pagesKhatib2017 PDFluxmansrikanthaNo ratings yet
- PBL Modul 2 TropisDocument31 pagesPBL Modul 2 TropiskasmaNo ratings yet
- Acute GlomerulonephritisDocument1 pageAcute GlomerulonephritisAyrheen FornolesNo ratings yet
- Etiology and Pathogenesis of The Congenital Pneumonia in Newborns Literature Review Part 1 PDFDocument4 pagesEtiology and Pathogenesis of The Congenital Pneumonia in Newborns Literature Review Part 1 PDFGolden DawnNo ratings yet
- Eat Yourself Smart: Britain Faces Airlift DeadlineDocument64 pagesEat Yourself Smart: Britain Faces Airlift DeadlineNidhi BhartiNo ratings yet