You might also like
- Loan-Level Price Adjustment (LLPA) MatrixDocument8 pagesLoan-Level Price Adjustment (LLPA) MatrixLashon SpearsNo ratings yet
- Obstructive Disease of Lung and Physiotherapy ManagementDocument76 pagesObstructive Disease of Lung and Physiotherapy Managementphysio43100% (1)
- IT ParksDocument12 pagesIT ParksDivam Goyal0% (1)
- Creative Writers and Daydreaming by Sigmund Freud To Print.Document7 pagesCreative Writers and Daydreaming by Sigmund Freud To Print.Robinhood Pandey82% (11)
- Perofrmance Task in Science: Renzo Anjelo Sison Mr. Wilson Vicente T. Gomez Grade 9 Bonicfacio ADocument17 pagesPerofrmance Task in Science: Renzo Anjelo Sison Mr. Wilson Vicente T. Gomez Grade 9 Bonicfacio AAnjelo SisonNo ratings yet
- Jzdinglasan@bpsu - Edu.ph: Joben Zamora Dinglasan Bs Psych - 1ADocument4 pagesJzdinglasan@bpsu - Edu.ph: Joben Zamora Dinglasan Bs Psych - 1ACogie PeraltaNo ratings yet
- Lung ConditionsDocument1 pageLung ConditionsAbhijeet SingareNo ratings yet
- Lung Volumes and CapacitiesDocument9 pagesLung Volumes and CapacitiesMukesh YadavNo ratings yet
- NCM 118 FinalDocument2 pagesNCM 118 FinalAddah, Dhenaraiza H.No ratings yet
- Bronchiectasis PathophysiologyDocument4 pagesBronchiectasis PathophysiologyBrunhild BangayanNo ratings yet
- Lower Respiratory System GlossaryDocument2 pagesLower Respiratory System GlossaryLarissa ShevchenkoNo ratings yet
- Activity-11-Respiratory-System - PERALTADocument3 pagesActivity-11-Respiratory-System - PERALTACogie PeraltaNo ratings yet
- Pathology of The Respiratory System 2Document76 pagesPathology of The Respiratory System 2Fabian ChapimaNo ratings yet
- Human LungsDocument2 pagesHuman Lungsvrtihik rajNo ratings yet
- 2 - CopdDocument40 pages2 - CopdFathima MulthazimaNo ratings yet
- Atelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Document10 pagesAtelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Gan BangNo ratings yet
- Obstructive Airway DiseasesDocument56 pagesObstructive Airway Diseaseskalanakariyawasam99No ratings yet
- Pulmonary PathologyDocument46 pagesPulmonary PathologyMuostafa KamelNo ratings yet
- Respiratory Diseases TypesDocument4 pagesRespiratory Diseases TypesDjdjjd SiisusNo ratings yet
- 7 6sistresp2Document46 pages7 6sistresp2Anto GorlaaNo ratings yet
- CopdDocument30 pagesCopdsalmanhabeebekNo ratings yet
- Case Study On AtelectasisDocument14 pagesCase Study On AtelectasisSanhati Ghosh BanerjeeNo ratings yet
- Pathology Disease ProcessesDocument11 pagesPathology Disease ProcessesprtemnNo ratings yet
- Copd NotesDocument11 pagesCopd NotesAgnes Jeane EnriquezNo ratings yet
- List of Diseases of The Respiratory System: Central Sleep ApneaDocument4 pagesList of Diseases of The Respiratory System: Central Sleep ApneaPaola ParkerNo ratings yet
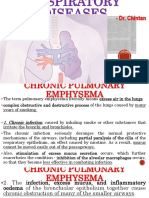
- Dr. ChintanDocument26 pagesDr. ChintanArshad KhanNo ratings yet
- The Lungs: Lung ConditionsDocument8 pagesThe Lungs: Lung ConditionsnandaNo ratings yet
- Lung PathologyDocument68 pagesLung PathologyJohn LloydNo ratings yet
- EmphysemaDocument2 pagesEmphysemaGeorley LobridoNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument3 pagesChronic Obstructive Pulmonary DiseaseJessica Corona - MarianoNo ratings yet
- 109 - Obstructive Lung DiseasesDocument8 pages109 - Obstructive Lung DiseasesCharisa Antonette HuelvaNo ratings yet
- COPDDocument7 pagesCOPDarminmercado7406No ratings yet
- Drugs RespiratoryDocument15 pagesDrugs RespiratoryLuiciaNo ratings yet
- Pneumothorax (Collapsed Lung)Document34 pagesPneumothorax (Collapsed Lung)james garcia100% (3)
- Cough: by Dr. Meghana Patil (Intern Batch 2016)Document24 pagesCough: by Dr. Meghana Patil (Intern Batch 2016)Meghana PatilNo ratings yet
- The Respiratory SystemDocument8 pagesThe Respiratory SystemJane Rose SuperadaNo ratings yet
- Materi Kelainan ParuDocument72 pagesMateri Kelainan ParuDebiNingtyasDwiKusumaWardaniNo ratings yet
- Diseases of The Respiratory System and Circulatory SystemDocument7 pagesDiseases of The Respiratory System and Circulatory SystemMaria Teresa GimenoNo ratings yet
- Past Year RespiDocument5 pagesPast Year RespiThulasi tootsieNo ratings yet
- COPDDocument52 pagesCOPDSoySauceNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument9 pagesChronic Obstructive Pulmonary DiseaseRouwi DesiatcoNo ratings yet
- Recognizing Interstitial Versus Airspace Disease: in Slide Show Mode, Advance The Slides by Pressing The SpacebarDocument32 pagesRecognizing Interstitial Versus Airspace Disease: in Slide Show Mode, Advance The Slides by Pressing The SpacebarCheska TumulakNo ratings yet
- Respiratory SystemDocument85 pagesRespiratory SystemDr:-Ustaad Aakass Ahmed Junejo SahabNo ratings yet
- Walang Pamagat Na DokumentoDocument3 pagesWalang Pamagat Na Dokumentobenedict cruz DevianaNo ratings yet
- hệ hô hấpDocument3 pageshệ hô hấpGianggNo ratings yet
- Onchi & CopdDocument8 pagesOnchi & CopdAngellene GraceNo ratings yet
- Bronchopneumonia or Bronchial Pneumonia or "Bronchogenic Pneumonia" (Not To BeDocument3 pagesBronchopneumonia or Bronchial Pneumonia or "Bronchogenic Pneumonia" (Not To Beverniejhoy09No ratings yet
- Respiratory: Welcome!Document119 pagesRespiratory: Welcome!Majo ParagasNo ratings yet
- PneumothoraxDocument7 pagesPneumothoraxKareliya ChiragNo ratings yet
- Pathology of Airway DiseasesDocument42 pagesPathology of Airway DiseasesZijieNo ratings yet
- Laporan Pendahuluan TBC Paru (Tuberculosis Paru) Di Rs. Tentara Dr. Soepraoen MalangDocument18 pagesLaporan Pendahuluan TBC Paru (Tuberculosis Paru) Di Rs. Tentara Dr. Soepraoen MalangalviraleaNo ratings yet
- Physiological Overview in Relation To PracticeDocument52 pagesPhysiological Overview in Relation To PracticedrkhaledassemNo ratings yet
- Health Issue Related To The Human Respiratory SystemDocument4 pagesHealth Issue Related To The Human Respiratory SystemKit Ying TanNo ratings yet
- "Bronchitis": Respiratory DisorderDocument40 pages"Bronchitis": Respiratory Disorderaswin379No ratings yet
- Anatomi Fisiologi Sistem Pernafasan - Id.enDocument7 pagesAnatomi Fisiologi Sistem Pernafasan - Id.enCindy Ari SantiNo ratings yet
- Approach To The Patient With Disease of The Respiratory SystemDocument3 pagesApproach To The Patient With Disease of The Respiratory SystemIsabel CastilloNo ratings yet
- Respi PathophysioDocument31 pagesRespi PathophysioIsmael JaaniNo ratings yet
- AtelectasisDocument30 pagesAtelectasisashoaib0313No ratings yet
- Lung AbcessDocument12 pagesLung AbcessABI OFFICIALNo ratings yet
- Respiratory System1Document5 pagesRespiratory System1Ombati StephenNo ratings yet
- What Is EmphysemaDocument8 pagesWhat Is EmphysemaHadibah MokhtarNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesFrom EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo ratings yet
- Henri Fayol A StrategistDocument13 pagesHenri Fayol A StrategistTerence DeluNo ratings yet
- Deed of Donation BicycleDocument2 pagesDeed of Donation BicycleCharlemagne PapioNo ratings yet
- Message From The School Head, Roy G. CrawfordDocument6 pagesMessage From The School Head, Roy G. Crawfordapi-22065138No ratings yet
- My Day: Reading Materials I CourseDocument7 pagesMy Day: Reading Materials I CourseZeynab BagirovaNo ratings yet
- ELT Catalog Secondary PDFDocument26 pagesELT Catalog Secondary PDFRafael Cruz IsidoroNo ratings yet
- House Bill 4208Document1 pageHouse Bill 4208Sinclair Broadcast Group - EugeneNo ratings yet
- Team2 - Rizal's Life in Paris and GermanyDocument26 pagesTeam2 - Rizal's Life in Paris and Germanydreianne26No ratings yet
- Forrester Hybrid Integration PlatformDocument17 pagesForrester Hybrid Integration PlatformrtNo ratings yet
- Political Law Reviewer Bar 2019 Part 1 V 20 by Atty. Alexis Medina ACADEMICUSDocument27 pagesPolitical Law Reviewer Bar 2019 Part 1 V 20 by Atty. Alexis Medina ACADEMICUSalyamarrabeNo ratings yet
- First Conditional Advice Interactive WorksheetDocument2 pagesFirst Conditional Advice Interactive WorksheetMurilo BaldanNo ratings yet
- ACS880 IGBT Supply Control Program: Firmware ManualDocument254 pagesACS880 IGBT Supply Control Program: Firmware ManualGopinath PadhiNo ratings yet
- Soni Musicae Diato K2 enDocument2 pagesSoni Musicae Diato K2 enknoNo ratings yet
- 7 P's of McDonaldsDocument11 pages7 P's of McDonaldsdd1684100% (4)
- 6 - Cash Flow StatementDocument42 pages6 - Cash Flow StatementBhagaban DasNo ratings yet
- Operating BudgetDocument38 pagesOperating BudgetRidwan O'connerNo ratings yet
- Ganendra Art House: 8 Lorong 16/7B, 46350 Petaling Jaya, Selangor, MalaysiaDocument25 pagesGanendra Art House: 8 Lorong 16/7B, 46350 Petaling Jaya, Selangor, MalaysiaFiorela Estrella VentocillaNo ratings yet
- PET ScanDocument3 pagesPET ScanChim PalmarioNo ratings yet
- Snail Production Techniques in Nigeria (Extension No. 108, Forestry Series No. 12) BulletinDocument23 pagesSnail Production Techniques in Nigeria (Extension No. 108, Forestry Series No. 12) BulletinGbenga AgunbiadeNo ratings yet
- Legalese and Legal EnglishDocument16 pagesLegalese and Legal English667yhNo ratings yet
- Kitty GenoveseDocument2 pagesKitty GenoveseRachael BartlettNo ratings yet
- Book 1Document30 pagesBook 1uday sonawaneNo ratings yet
- Cloud Assignment 2Document4 pagesCloud Assignment 2tiraNo ratings yet
- PAL v. CIR (GR 198759)Document2 pagesPAL v. CIR (GR 198759)Erica Gana100% (1)
- Art of CharacterizationDocument4 pagesArt of CharacterizationAli RazaNo ratings yet
- Masculine Ideal in The Old Man and The SeaDocument5 pagesMasculine Ideal in The Old Man and The Seaapi-295869808No ratings yet
- LRD Waiting ListDocument209 pagesLRD Waiting ListPrince PatelNo ratings yet
- Ele Unit5 Revision PDFDocument2 pagesEle Unit5 Revision PDFNatalia ZapataNo ratings yet