You might also like
- Pathophysiology/Epidemiology of Acute Coronary Syndromes: 1 2 November 2019Document15 pagesPathophysiology/Epidemiology of Acute Coronary Syndromes: 1 2 November 2019anasNo ratings yet
- Acute Coronary SyndromeDocument5 pagesAcute Coronary SyndromeLuis OportoNo ratings yet
- Topic:: Unstable AnginaDocument44 pagesTopic:: Unstable AnginaApurba100% (1)
- Acute Coronary Syndrome: Patsadee Nachom MDDocument58 pagesAcute Coronary Syndrome: Patsadee Nachom MDRachapon OngwibunwongNo ratings yet
- Acute Coronary SyndromeDocument57 pagesAcute Coronary SyndromePreety ShresthaNo ratings yet
- Diagnosis and Management of Myocardial InfarctionDocument69 pagesDiagnosis and Management of Myocardial InfarctionSanjana GkNo ratings yet
- Step 2 CK Review - CardiologyDocument28 pagesStep 2 CK Review - Cardiologyrsmd1986100% (1)
- Acute Coronary SyndromesDocument82 pagesAcute Coronary Syndromesmidras taranNo ratings yet
- Tatalaksana Sindrom Koroner Akut Dengan Elevasi Segmen STDocument77 pagesTatalaksana Sindrom Koroner Akut Dengan Elevasi Segmen STQueenta SariNo ratings yet
- Anaesthetic Management of A Patient With Ischaemic Heart Disease Undergoing Non Cardiac SurgeryDocument72 pagesAnaesthetic Management of A Patient With Ischaemic Heart Disease Undergoing Non Cardiac SurgeryDebasis SahooNo ratings yet
- Acute Myocardial InfarctionDocument13 pagesAcute Myocardial InfarctionSajjad KabirNo ratings yet
- ACS: Acute Coronary SyndromeDocument48 pagesACS: Acute Coronary SyndromeAchmad ulil Albab100% (1)
- Media 115008 en PDFDocument12 pagesMedia 115008 en PDFsukandeNo ratings yet
- Manajement Acut Coronary Syndroma (Acs) : Lalu Aries FahroziDocument77 pagesManajement Acut Coronary Syndroma (Acs) : Lalu Aries FahroziJanuar MardaniNo ratings yet
- Ekg PJKDocument113 pagesEkg PJKdevipuspaNo ratings yet
- Ischemic Heart Disease: Causes, Types, Diagnosis and TreatmentDocument67 pagesIschemic Heart Disease: Causes, Types, Diagnosis and TreatmentDylan KremerNo ratings yet
- Step Up To MedicineDocument68 pagesStep Up To MedicineAmadou N'Dow100% (1)
- Cardiology-6 CADDocument20 pagesCardiology-6 CADMahmoud RamadanNo ratings yet
- Approach To The Patient With A Heart MurmurDocument103 pagesApproach To The Patient With A Heart MurmurDarawan MirzaNo ratings yet
- ACS LectureDocument76 pagesACS Lecture21701101047 Laksmita AnggaraniNo ratings yet
- DR Rahul VarshneyDocument64 pagesDR Rahul VarshneyIMNo ratings yet
- Overview of Acute Coronary Syndromes (ACS) : MSD Manual Professional VersionDocument11 pagesOverview of Acute Coronary Syndromes (ACS) : MSD Manual Professional VersionSuhadak DrsNo ratings yet
- Common Cardiovascular Diseases Often Found DailyDocument121 pagesCommon Cardiovascular Diseases Often Found Dailyandikaagus13No ratings yet
- د.عبدالكريم العثمان VHD Murmur With AnssDocument110 pagesد.عبدالكريم العثمان VHD Murmur With AnssBashar KhaleelNo ratings yet
- Satjit Bhusri, MD Cardiologist Lenox Hill Hospital: Jeff Chianfagna Rpa-CDocument76 pagesSatjit Bhusri, MD Cardiologist Lenox Hill Hospital: Jeff Chianfagna Rpa-CAjaz JunachNo ratings yet
- Tatalaksana Sindrom Koroner Akut Dengan Elevasi Segmen ST: Saharman Leman, Rony Y SyarifDocument77 pagesTatalaksana Sindrom Koroner Akut Dengan Elevasi Segmen ST: Saharman Leman, Rony Y SyarifSigit_Rokhmadi100% (1)
- Lapkas PP (STEMI)Document68 pagesLapkas PP (STEMI)KurbulNo ratings yet
- Pulmonary Embolism: Diagnosis, Treatment, and Prevention Philip Keith March 26, 2008Document24 pagesPulmonary Embolism: Diagnosis, Treatment, and Prevention Philip Keith March 26, 2008Fahd Abdullah Al-refaiNo ratings yet
- Acute Coronary Syndrome 052014Document91 pagesAcute Coronary Syndrome 052014Fatahillah NazarNo ratings yet
- Lecture 7Document11 pagesLecture 7Grafu Andreea AlexandraNo ratings yet
- Acute Coronary Syndrome: by Ho NisaDocument58 pagesAcute Coronary Syndrome: by Ho NisaShre RanjithamNo ratings yet
- How To Detect and To Treat EarlierDocument59 pagesHow To Detect and To Treat EarlierFaisal ShaldyNo ratings yet
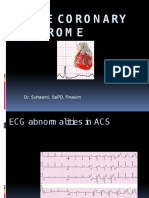
- Acutecoronary Syndrome: Dr. Suhaemi, SPPD, FinasimDocument65 pagesAcutecoronary Syndrome: Dr. Suhaemi, SPPD, FinasimpuspayafelliNo ratings yet
- Acute Coronary Syndrome: Kingdom of Saudi Arabia Ministry of Health King Fahad Hofuf Hospital Nursing EducationDocument33 pagesAcute Coronary Syndrome: Kingdom of Saudi Arabia Ministry of Health King Fahad Hofuf Hospital Nursing EducationAqeelNo ratings yet
- AnginaDocument43 pagesAnginaMuhammad Ashraf AhmadNo ratings yet
- Coronary Arterial Disease: S Chapter 60 1657Document26 pagesCoronary Arterial Disease: S Chapter 60 1657Staen KisNo ratings yet
- Mitral RegurgitationDocument43 pagesMitral Regurgitationraissasafitry100% (1)
- Cardio InternetDocument46 pagesCardio InternetnaimNo ratings yet
- Acute Coronary Syndrome GuideDocument57 pagesAcute Coronary Syndrome Guideendah100% (1)
- Treatment of Acute Coronary Syndrome: Part 1: Non-ST-segment Acute Coronary SyndromeDocument8 pagesTreatment of Acute Coronary Syndrome: Part 1: Non-ST-segment Acute Coronary SyndromeTiago SouzaNo ratings yet
- Acute Coronary Syndrome: Mini LectureDocument44 pagesAcute Coronary Syndrome: Mini LectureJayden WaveNo ratings yet
- Chest PainDocument50 pagesChest PainGrafu Andreea AlexandraNo ratings yet
- Acute Coronary Syndrome (G4)Document6 pagesAcute Coronary Syndrome (G4)Francis Josh DagohoyNo ratings yet
- Askep Pada Acute Coronary Syndrome AcsDocument62 pagesAskep Pada Acute Coronary Syndrome Acsdefi rhNo ratings yet
- Acute Coronary Syndrome: Imelva Yulviani GirsangDocument34 pagesAcute Coronary Syndrome: Imelva Yulviani GirsangAmeel BubbleeNo ratings yet
- Acute Coronary Syndromes: Acute MI and Unstable Angina: Tintinalli Chapter 50 September 20, 2005Document62 pagesAcute Coronary Syndromes: Acute MI and Unstable Angina: Tintinalli Chapter 50 September 20, 2005Jibak MajumderNo ratings yet
- Unstable Angina (UAP) and non-STEMIDocument66 pagesUnstable Angina (UAP) and non-STEMIIddrisu Abdul-AzizNo ratings yet
- CCRN-PCCN-CMC Review Cardiac Part 1 PDFDocument14 pagesCCRN-PCCN-CMC Review Cardiac Part 1 PDFGiovanni Mictil100% (1)
- ACS LectureDocument74 pagesACS Lecturekarin amalia sabrinaNo ratings yet
- Acute Miocard InfarkDocument32 pagesAcute Miocard InfarkhansNo ratings yet
- ACS Guide Provides Updates on Diagnosis, TreatmentDocument72 pagesACS Guide Provides Updates on Diagnosis, TreatmentYeyen Devyanti HandokoNo ratings yet
- Acute Coronary SyndromeDocument30 pagesAcute Coronary SyndromeEndar EszterNo ratings yet
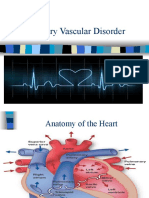
- Coronary Artery Disorder Student 2014Document92 pagesCoronary Artery Disorder Student 2014Roa'a KanakriNo ratings yet
- Acute Limb Ischemia Acute Limb Ischemia Acute Limb Ischemia Acute Limb IschemiaDocument34 pagesAcute Limb Ischemia Acute Limb Ischemia Acute Limb Ischemia Acute Limb Ischemiahasratku100% (1)
- Present To Mam: Sajida Zahoor Presented byDocument35 pagesPresent To Mam: Sajida Zahoor Presented byM RazzaqNo ratings yet
- Alshammari Cards CRDocument314 pagesAlshammari Cards CRSimonNo ratings yet
- Department of Internal Medicine Ii and Phthysiatry: - Rajkumar Subasaravanan Subgroup "12"Document57 pagesDepartment of Internal Medicine Ii and Phthysiatry: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- SoalDocument4 pagesSoalkurikulum man2wonosoboNo ratings yet
- Weekly Capital Market Report Week Ending 22.07.2022 2022-07-22Document2 pagesWeekly Capital Market Report Week Ending 22.07.2022 2022-07-22Fuaad DodooNo ratings yet
- 6 Fsiqiatria-1524041346Document48 pages6 Fsiqiatria-1524041346მირანდა გიორგაშვილიNo ratings yet
- Bruce MoenDocument4 pagesBruce MoenGeorge Stefanakos100% (5)
- 2013 KTM 350 EXC Shop-Repair ManualDocument310 pages2013 KTM 350 EXC Shop-Repair ManualTre100% (7)
- Review of Esu Yoruba God Power and The IDocument7 pagesReview of Esu Yoruba God Power and The IBoris MilovicNo ratings yet
- Written Work 1 Q1 Science 10Document6 pagesWritten Work 1 Q1 Science 10JOEL MONTERDENo ratings yet
- 100 Answers To Common English QuestionsDocument9 pages100 Answers To Common English Questionsflemus_1No ratings yet
- Using Facebook Groups To Support Teachers' Professional DevelopmentDocument22 pagesUsing Facebook Groups To Support Teachers' Professional DevelopmentLilmal SihamNo ratings yet
- Bipolar DisorderDocument9 pagesBipolar Disorderapi-306929216No ratings yet
- Target products to meet 20% demandDocument12 pagesTarget products to meet 20% demandAlma Dela PeñaNo ratings yet
- Types of Companies Classified by Incorporation, Membership, Liability and ControlDocument11 pagesTypes of Companies Classified by Incorporation, Membership, Liability and ControlPrasad BulbuleNo ratings yet
- Water As A Weapon - Israel National NewsDocument11 pagesWater As A Weapon - Israel National NewsJorge Yitzhak Pachas0% (1)
- Skills Test Unit 1 Test A EmailDocument4 pagesSkills Test Unit 1 Test A EmailЛиза ОмельченкоNo ratings yet
- Emerson Field Tools Quick Start GuideDocument48 pagesEmerson Field Tools Quick Start Guidepks_2410No ratings yet
- Dell in India Targeting SMB Markets - The Differentiation Strategy PDFDocument16 pagesDell in India Targeting SMB Markets - The Differentiation Strategy PDFJatinNo ratings yet
- Motor-Catalog English 2013 PDFDocument80 pagesMotor-Catalog English 2013 PDFILham Dwi PutraNo ratings yet
- Thesis Chapter 123Document15 pagesThesis Chapter 123Chesca Mae PenalosaNo ratings yet
- Down Syndrome Research PaperDocument11 pagesDown Syndrome Research Paperapi-299871292100% (1)
- Criteria For Judging MR and Ms UNDocument9 pagesCriteria For Judging MR and Ms UNRexon ChanNo ratings yet
- Sivas Doon LecturesDocument284 pagesSivas Doon LectureskartikscribdNo ratings yet
- Ky203817 PSRPT 2022-05-17 14.39.33Document8 pagesKy203817 PSRPT 2022-05-17 14.39.33Thuy AnhNo ratings yet
- Zambia Budget 2010Document26 pagesZambia Budget 2010Chola Mukanga100% (3)
- ISL201-Solved MCQs 100 - Correct For Mid Term Papers (WWW - Virtualstudysolutions.blogspot - Com)Document70 pagesISL201-Solved MCQs 100 - Correct For Mid Term Papers (WWW - Virtualstudysolutions.blogspot - Com)bc190200669 BUSHRANo ratings yet
- 100-Word Replacement PDFDocument14 pages100-Word Replacement PDFTheodore Vijay100% (1)
- Baltimore County IG ReportDocument35 pagesBaltimore County IG ReportChris BerinatoNo ratings yet
- Ume Mri GuideDocument1 pageUme Mri GuideHiba AhmedNo ratings yet
- Chapter 3 Professional Practices in Nepal ADocument20 pagesChapter 3 Professional Practices in Nepal Amunna smithNo ratings yet
- RetailMarketinginIndia 1Document158 pagesRetailMarketinginIndia 1RamanNo ratings yet
- Update in Living Legal Ethics - Justice Dela CruzDocument13 pagesUpdate in Living Legal Ethics - Justice Dela CruzRobert F Catolico IINo ratings yet