You might also like
- Acutecoronarysyndromeacs 180106041458Document82 pagesAcutecoronarysyndromeacs 180106041458Razvan SulaimanNo ratings yet
- Common Cardiovascular Diseases Often Found DailyDocument121 pagesCommon Cardiovascular Diseases Often Found Dailyandikaagus13No ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Acute Coronary Syndrome 052014Document91 pagesAcute Coronary Syndrome 052014Fatahillah NazarNo ratings yet
- ACS LectureDocument76 pagesACS Lecture21701101047 Laksmita AnggaraniNo ratings yet
- Pathophysiology Week 1Document15 pagesPathophysiology Week 1Dan HoNo ratings yet
- Acute Coronary Syndromes: Acute MI and Unstable Angina: Tintinalli Chapter 50 September 20, 2005Document62 pagesAcute Coronary Syndromes: Acute MI and Unstable Angina: Tintinalli Chapter 50 September 20, 2005Jibak MajumderNo ratings yet
- 209 Pope, B. CCRN-PCCN-CMC Review Cardiac Part 1Document14 pages209 Pope, B. CCRN-PCCN-CMC Review Cardiac Part 1peanant100% (1)
- Topic:: Unstable AnginaDocument44 pagesTopic:: Unstable AnginaApurba100% (1)
- How To Detect and To Treat EarlierDocument59 pagesHow To Detect and To Treat EarlierFaisal ShaldyNo ratings yet
- Acute Coronary Syndrome and Coronary Heart Disease GuideDocument29 pagesAcute Coronary Syndrome and Coronary Heart Disease GuideDwi Akbarina YahyaNo ratings yet
- Step Up To MedicineDocument68 pagesStep Up To MedicineAmadou N'Dow100% (1)
- Osce Notes - Myocardial InfarctionDocument10 pagesOsce Notes - Myocardial InfarctionmmmalcampoNo ratings yet
- Approach To Acute Coronary SyndromeDocument25 pagesApproach To Acute Coronary Syndromeزكريا الحسناتNo ratings yet
- Management of Acute Coronary SyndromeDocument73 pagesManagement of Acute Coronary SyndromeSantosh NaliathNo ratings yet
- Unstable Angina, STEMI, NSTEMI Diagnosis and ManagementDocument21 pagesUnstable Angina, STEMI, NSTEMI Diagnosis and ManagementNabil Mosharraf Hossain100% (2)
- PATH - Ischaemic Heart Disease (13p)Document13 pagesPATH - Ischaemic Heart Disease (13p)vikashchahal1987No ratings yet
- Acute Coronary Syndrome: Patsadee Nachom MDDocument58 pagesAcute Coronary Syndrome: Patsadee Nachom MDRachapon OngwibunwongNo ratings yet
- Acute Coronary SyndromeDocument24 pagesAcute Coronary SyndromeMuhammad Alauddin Sarwar100% (8)
- Askep Pada Acute Coronary Syndrome AcsDocument62 pagesAskep Pada Acute Coronary Syndrome Acsdefi rhNo ratings yet
- Stemi PDFDocument60 pagesStemi PDFPraveen100% (1)
- IMA Nurse KKV SaifurDocument69 pagesIMA Nurse KKV Saifureva munartyNo ratings yet
- Acs TrombolitikDocument55 pagesAcs TrombolitikDiana IswardhaniNo ratings yet
- Coronary Artery DiseaseDocument53 pagesCoronary Artery DiseaseJoel CanenciaNo ratings yet
- NSTEMIDocument29 pagesNSTEMIGeanina CreangaNo ratings yet
- Acute Coronary Syndrome: Imelva Yulviani GirsangDocument34 pagesAcute Coronary Syndrome: Imelva Yulviani GirsangAmeel BubbleeNo ratings yet
- Acute Coronary SyndromeDocument84 pagesAcute Coronary SyndromeRinkita MallickNo ratings yet
- Acute Coronary Syndrome: Deske Muhadi Departemen Penyakit Dalam Fak - Kedokteran USU/RS HAM/RS PMDocument71 pagesAcute Coronary Syndrome: Deske Muhadi Departemen Penyakit Dalam Fak - Kedokteran USU/RS HAM/RS PMsebastian1207No ratings yet
- Media 115008 en PDFDocument12 pagesMedia 115008 en PDFsukandeNo ratings yet
- Acute Choronary SyndromeDocument7 pagesAcute Choronary SyndromeSafana NazeerNo ratings yet
- Cardiac Emergency AMI GuideDocument34 pagesCardiac Emergency AMI GuideAdmin neuro-usu.idNo ratings yet
- Acute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPDocument57 pagesAcute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPrian susantoNo ratings yet
- Cardio MTB 2:3 Notes DONEDocument10 pagesCardio MTB 2:3 Notes DONESumatt KaurNo ratings yet
- ESC Guidelines for the management of Acute Coronary Syndrome patients without ST Elevation 2011Document38 pagesESC Guidelines for the management of Acute Coronary Syndrome patients without ST Elevation 2011mikaNo ratings yet
- Acute Coronary Syndrome GuideDocument50 pagesAcute Coronary Syndrome GuideWinda Ayu PurnamasariNo ratings yet
- ACSDocument54 pagesACSDidik SusetiyantoNo ratings yet
- Cardio InternetDocument46 pagesCardio InternetnaimNo ratings yet
- Acutecoronary Syndrome: Dr. Suhaemi, SPPD, FinasimDocument65 pagesAcutecoronary Syndrome: Dr. Suhaemi, SPPD, FinasimpuspayafelliNo ratings yet
- Sindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Document68 pagesSindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Dafhina Store100% (1)
- CARDIOLOGY – “PLABABLE” VALVULAR HEART DISEASE SIGNSDocument22 pagesCARDIOLOGY – “PLABABLE” VALVULAR HEART DISEASE SIGNSTirtha Taposh100% (1)
- Prof. Iwan - Kuliah RHD and VHD-1Document41 pagesProf. Iwan - Kuliah RHD and VHD-1delia rahmaNo ratings yet
- Tata Laksana Sindroma Koroner Akut: Cholid Tri TjahjonoDocument96 pagesTata Laksana Sindroma Koroner Akut: Cholid Tri TjahjonoAhmad Riva'iNo ratings yet
- ACS Guide Provides Updates on Diagnosis, TreatmentDocument72 pagesACS Guide Provides Updates on Diagnosis, TreatmentYeyen Devyanti HandokoNo ratings yet
- Acute Coronary SyndromesDocument82 pagesAcute Coronary Syndromesmidras taranNo ratings yet
- Acute Coronary Syndrome: by Ho NisaDocument58 pagesAcute Coronary Syndrome: by Ho NisaShre RanjithamNo ratings yet
- CCRN-PCCN-CMC Review Cardiac Part 1 PDFDocument14 pagesCCRN-PCCN-CMC Review Cardiac Part 1 PDFGiovanni Mictil100% (1)
- Step 2 CK Review - CardiologyDocument28 pagesStep 2 CK Review - Cardiologyrsmd1986100% (1)
- Family Med EOR Study Guide 1Document86 pagesFamily Med EOR Study Guide 1Ranjani ammuNo ratings yet
- Lapkas PP (STEMI)Document68 pagesLapkas PP (STEMI)KurbulNo ratings yet
- Anaesthetic Management of A Patient With Ischaemic Heart Disease Undergoing Non Cardiac SurgeryDocument72 pagesAnaesthetic Management of A Patient With Ischaemic Heart Disease Undergoing Non Cardiac SurgeryDebasis SahooNo ratings yet
- ST-Elevation Myocardial Infarction (Stemi) : Present byDocument29 pagesST-Elevation Myocardial Infarction (Stemi) : Present byReema AlamriNo ratings yet
- Acute Coronary SyndromeDocument42 pagesAcute Coronary SyndromeGorgieNo ratings yet
- Acute Coronary Syndrome-SignedDocument3 pagesAcute Coronary Syndrome-Signedابو الجودNo ratings yet
- Presentation On Myocardial Infarction By-Dr - Vinay VatsayanDocument32 pagesPresentation On Myocardial Infarction By-Dr - Vinay VatsayandrvinayvNo ratings yet
- Present To Mam: Sajida Zahoor Presented byDocument35 pagesPresent To Mam: Sajida Zahoor Presented byM RazzaqNo ratings yet
- Parkinson's Disease-Diagnosis & TreatmentDocument9 pagesParkinson's Disease-Diagnosis & Treatmentvivek_win95100% (1)
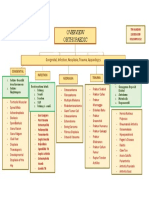
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesDocument1 pageOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsNo ratings yet
- Evaluation of The Diagnosis of Typhoid Fever UsingDocument7 pagesEvaluation of The Diagnosis of Typhoid Fever UsingHarshit KumarNo ratings yet
- Aripiprazole Drug Study - Rhuby AbenojaDocument1 pageAripiprazole Drug Study - Rhuby AbenojaRHUBY ABENOJANo ratings yet
- Lab 4 Activity 4Document4 pagesLab 4 Activity 4Abigail YoungNo ratings yet
- Eidon - Atlas Catalog WebDocument51 pagesEidon - Atlas Catalog Webefze71No ratings yet
- CATARACT History Taking and ExaminationDocument28 pagesCATARACT History Taking and ExaminationJosephNo ratings yet
- Philcare Application Form - 07302013Document6 pagesPhilcare Application Form - 07302013Jerry Barad SarioNo ratings yet
- Methamphetamine Addiction: A Review of The LiteratureDocument8 pagesMethamphetamine Addiction: A Review of The Literaturesaghita fauziahNo ratings yet
- Citrus Black Spot PDFDocument2 pagesCitrus Black Spot PDFamuronegaduNo ratings yet
- NDocument136 pagesNLove HumanNo ratings yet
- GIT ExaminationDocument134 pagesGIT ExaminationMontasir AhmedNo ratings yet
- Zuku Visual Flashnotes Distemper ExtendedDocument4 pagesZuku Visual Flashnotes Distemper ExtendedShubham HarishNo ratings yet
- Breast Examination - ADocument30 pagesBreast Examination - AAkash VermaNo ratings yet
- The Psychiatric Review of Symptoms - A Screening Tool For Family Physicians - American Family PhysicianDocument7 pagesThe Psychiatric Review of Symptoms - A Screening Tool For Family Physicians - American Family PhysicianTimothy TurscakNo ratings yet
- Drug Resistance TB Mono Drug Resistant TBDocument2 pagesDrug Resistance TB Mono Drug Resistant TBMalavath PavithranNo ratings yet
- Corosive PoisoningDocument16 pagesCorosive Poisoninglitan dasNo ratings yet
- Atsp Book 2011Document24 pagesAtsp Book 2011Chengyuan ZhangNo ratings yet
- Aiims SkinDocument85 pagesAiims SkinSagar MukherjeeNo ratings yet
- AdenovirusDocument3 pagesAdenovirustheodore_estradaNo ratings yet
- Stress - The Different Kinds of StressDocument4 pagesStress - The Different Kinds of StressbogdanNo ratings yet
- Histiocytic SarcomaDocument8 pagesHistiocytic SarcomadanishNo ratings yet
- Trematode SDocument26 pagesTrematode SothnielNo ratings yet
- Edgcse TTPP cb5 SB AnswersDocument5 pagesEdgcse TTPP cb5 SB AnswersRaijin Kaze0% (1)
- BakteriDocument8 pagesBakteriAgus SugiartoNo ratings yet
- Gineco Eu An 2016 NR 3Document60 pagesGineco Eu An 2016 NR 3GîrbovanCristinaNo ratings yet
- The 'Ins' and 'Outs' of Ureteric ObstructionDocument65 pagesThe 'Ins' and 'Outs' of Ureteric ObstructionThe Kidney ClubNo ratings yet
- HypospadiaDocument21 pagesHypospadiaShi YunNo ratings yet
- Medical History ReportDocument4 pagesMedical History ReportRacel AbulaNo ratings yet
- CUTANEOUS ALLERGY MECHANISMS AND TESTINGDocument26 pagesCUTANEOUS ALLERGY MECHANISMS AND TESTINGThiti JessadaromNo ratings yet