You might also like
- Evidence-Based LaryngologyFrom EverandEvidence-Based LaryngologyDavid E. RosowNo ratings yet
- 10 1002@gps 3787Document7 pages10 1002@gps 3787Gabriel VelozoNo ratings yet
- Crane 2012Document15 pagesCrane 2012Hugo Salomão F. G. MirôNo ratings yet
- Using Temporal Orientation, Category Uency, and Word Recall For Detecting Cognitive Impairment: The 10-Point Cognitive Screener (10-CS)Document10 pagesUsing Temporal Orientation, Category Uency, and Word Recall For Detecting Cognitive Impairment: The 10-Point Cognitive Screener (10-CS)Camila VelosoNo ratings yet
- Psychiatry Research: Tsuo-Hung Lan, Bo-Jian Wu, Hsing-Kang Chen, Hsun-Yi Liao, Shin-Min Lee, Hsiao-Ju SunDocument7 pagesPsychiatry Research: Tsuo-Hung Lan, Bo-Jian Wu, Hsing-Kang Chen, Hsun-Yi Liao, Shin-Min Lee, Hsiao-Ju Sunnermal93No ratings yet
- A Pediatric FOUR Score Coma Scale: Interrater Reliability and Predictive ValidityDocument9 pagesA Pediatric FOUR Score Coma Scale: Interrater Reliability and Predictive ValidityrachmadyNo ratings yet
- Validity of The Minimal Assessment of Cognitive Function in Multiple Sclerosis (MACFIMS)Document10 pagesValidity of The Minimal Assessment of Cognitive Function in Multiple Sclerosis (MACFIMS)Sarah Miryam CoffanoNo ratings yet
- Dementia: Alternate-Form Reliability of The Montreal Cognitive Assessment Screening Test in A Clinical SettingDocument7 pagesDementia: Alternate-Form Reliability of The Montreal Cognitive Assessment Screening Test in A Clinical SettingamatneeksNo ratings yet
- General Hospital Psychiatry: Review ArticleDocument10 pagesGeneral Hospital Psychiatry: Review Articlehevi_tarsumNo ratings yet
- Validación en Mexico 2022Document8 pagesValidación en Mexico 2022juanpaNo ratings yet
- Attention and Working Memory Deficits in Mild Cognitive ImpairmentDocument9 pagesAttention and Working Memory Deficits in Mild Cognitive ImpairmentsoniaNo ratings yet
- Chapman2019 MoCA OnlineDocument9 pagesChapman2019 MoCA OnlineJuan José Figueroa ValdiviezoNo ratings yet
- Does The Clock Drawing Test Have Focal Neuroanatomical CorrelatesDocument10 pagesDoes The Clock Drawing Test Have Focal Neuroanatomical CorrelatesIcaroNo ratings yet
- MSE Research 1Document11 pagesMSE Research 1kuro hanabusaNo ratings yet
- Magee 2016 MatadocDocument27 pagesMagee 2016 MatadocdougNo ratings yet
- 2008 - Feigin - Long Term Neuropsychological Functional Outcomes StrokeDocument8 pages2008 - Feigin - Long Term Neuropsychological Functional Outcomes StrokeLourdes CFNo ratings yet
- Test Performance and Classification Statistics For The Rey Auditory Verbal Learning Test in Selected Clinical SamplesDocument11 pagesTest Performance and Classification Statistics For The Rey Auditory Verbal Learning Test in Selected Clinical SamplesPatriciaNo ratings yet
- Moca ReviewDocument4 pagesMoca ReviewLuthfi IndiwirawanNo ratings yet
- RH Del MS en ACV PDFDocument12 pagesRH Del MS en ACV PDFDiego VolattiNo ratings yet
- If It: ProblemDocument9 pagesIf It: ProblemMafe SanchezNo ratings yet
- WNL 0000000000207740 FullDocument22 pagesWNL 0000000000207740 Fulllmra89No ratings yet
- Baremos Españoles TMTDocument15 pagesBaremos Españoles TMTMarta Olivera AymerichNo ratings yet
- Comparison of The Greek Version of The Quick Mild Cognitive Impairment Screen and Standardised Mini-Mental State ExaminationDocument9 pagesComparison of The Greek Version of The Quick Mild Cognitive Impairment Screen and Standardised Mini-Mental State Examinationmakis000No ratings yet
- Cognitive Reserve and Long-Term Change in Cognition in Aging and Preclinical Alzheimer's DiseaseDocument9 pagesCognitive Reserve and Long-Term Change in Cognition in Aging and Preclinical Alzheimer's Diseasechepin ChangNo ratings yet
- Medidas Cognitivas en EM Revisión 2021Document19 pagesMedidas Cognitivas en EM Revisión 2021juanpaNo ratings yet
- REvisión Sistemática 2023Document38 pagesREvisión Sistemática 2023juanpaNo ratings yet
- Prognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesDocument12 pagesPrognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesYan Sheng HoNo ratings yet
- Trail Making Test Errors in Normal Aging, Mild Cognitive Impairment, and DementiaDocument9 pagesTrail Making Test Errors in Normal Aging, Mild Cognitive Impairment, and DementiaCatarinaSilva97No ratings yet
- Estudo de Viabilidade 1Document4 pagesEstudo de Viabilidade 1ilcorpoliberoyogaNo ratings yet
- Assessment of Sleep Quality and Related Factors in Stroke PatientsDocument8 pagesAssessment of Sleep Quality and Related Factors in Stroke PatientsajmrdNo ratings yet
- Liu 2021Document8 pagesLiu 2021Instituto Integrado em PsicologiaNo ratings yet
- 2019 Damico PROs and PROMs in MSDocument6 pages2019 Damico PROs and PROMs in MSMaría Pía BalmacedaNo ratings yet
- Schmahmann Syndrome ScaleDocument23 pagesSchmahmann Syndrome ScaleLuna Begines FernándezNo ratings yet
- A New Age-Related Cutoff of Medial Temporal Atrophy Scale On MRI Improving The Diagnostic Accuracy of Neurodegeneration Due To Alzheimer's Disease in A Chinese PopulationDocument8 pagesA New Age-Related Cutoff of Medial Temporal Atrophy Scale On MRI Improving The Diagnostic Accuracy of Neurodegeneration Due To Alzheimer's Disease in A Chinese PopulationMuhammad Naqvi Al FarisiNo ratings yet
- Prevalen of DDocument8 pagesPrevalen of DĐỗ Văn ĐứcNo ratings yet
- Jurnal Syifa 4Document9 pagesJurnal Syifa 4cornelia cindy SRDNo ratings yet
- Texto 10-CSDocument9 pagesTexto 10-CSHenrique SalmazoNo ratings yet
- Assessing The Current State of Cognitive Frailty: Measurement PropertiesDocument9 pagesAssessing The Current State of Cognitive Frailty: Measurement PropertiesCarlos CarrilloNo ratings yet
- Acta Neuro Scandinavica - 2018 - Mani - Efficacy of Group Cognitive Rehabilitation Therapy in Multiple SclerosisDocument9 pagesActa Neuro Scandinavica - 2018 - Mani - Efficacy of Group Cognitive Rehabilitation Therapy in Multiple Sclerosismadalena limaNo ratings yet
- Comparison of ICD-10 and DSM-IV Criteria For Postconcussion SyndromedisorderDocument19 pagesComparison of ICD-10 and DSM-IV Criteria For Postconcussion Syndromedisorderneoraymix blackNo ratings yet
- CAMDEX. A Standardised Instrument For The Diagnosis of MentalDocument13 pagesCAMDEX. A Standardised Instrument For The Diagnosis of MentalLeila CamilaNo ratings yet
- Compens Memory 2003Document10 pagesCompens Memory 2003RuiNo ratings yet
- SuccessfulImplementationNIHSS2006 PDFDocument7 pagesSuccessfulImplementationNIHSS2006 PDFMaryoma HabibyNo ratings yet
- Deterioro Cognitivo LeveDocument7 pagesDeterioro Cognitivo LeveWicho DíazNo ratings yet
- Are Knowledge Gaps An Expected Result of The Current Culture of Neurosurgical Resident TrainingDocument3 pagesAre Knowledge Gaps An Expected Result of The Current Culture of Neurosurgical Resident Trainingghcabsb87No ratings yet
- Impact of Cognitive Impairment On MildDocument12 pagesImpact of Cognitive Impairment On MildCristina MPNo ratings yet
- Journal of Clinical and Experimental Neuropsychology: Merve Çebi, Gülsen Babacan, Öget Öktem Tanör & Hakan GürvitDocument10 pagesJournal of Clinical and Experimental Neuropsychology: Merve Çebi, Gülsen Babacan, Öget Öktem Tanör & Hakan GürvitDR RISKA WAHYUNo ratings yet
- Brief International Cognitive Assessment For MS (BICAMS) : International Standards For ValidationDocument8 pagesBrief International Cognitive Assessment For MS (BICAMS) : International Standards For ValidationandreapalmapNo ratings yet
- Middleton 2006Document8 pagesMiddleton 2006Nagy DaherNo ratings yet
- Mrazik, 2010 - TMT OralDocument8 pagesMrazik, 2010 - TMT OralMica Ballito de TroyaNo ratings yet
- Cognitive Assement - Woodford PDFDocument16 pagesCognitive Assement - Woodford PDFAnang MurdiatmokoNo ratings yet
- Katzan Et AlDocument9 pagesKatzan Et Alemsutton02No ratings yet
- The Impact of Anxiety On The Progression of Mild Cognitive Impairment To DementiaDocument10 pagesThe Impact of Anxiety On The Progression of Mild Cognitive Impairment To DementiaAnais UrdanetaNo ratings yet
- Bipolar Disorders - 2014 - Cholet - Using The Brief Assessment of Cognition in Schizophrenia BACS To Assess CognitiveDocument11 pagesBipolar Disorders - 2014 - Cholet - Using The Brief Assessment of Cognition in Schizophrenia BACS To Assess CognitiveLu LopezNo ratings yet
- Attention and Executive Functions in Microsurgically Treated Patients After Subarachnoid HemorrhageDocument6 pagesAttention and Executive Functions in Microsurgically Treated Patients After Subarachnoid HemorrhageDURRAH FARARESANo ratings yet
- MediterraneanDash Intervention For Neurodegenerative DelayDocument14 pagesMediterraneanDash Intervention For Neurodegenerative DelayMariNo ratings yet
- Neuropronostico en TceDocument29 pagesNeuropronostico en Tcejorge suarezNo ratings yet
- Cognitive DeclineDocument7 pagesCognitive DeclineSaul MorenoNo ratings yet
- Physical Health Assessment and Cardiometabolic Monitoring Practices Across Three Adult Mental Health Inpatient Units - A Retrospective Cohort StudyDocument13 pagesPhysical Health Assessment and Cardiometabolic Monitoring Practices Across Three Adult Mental Health Inpatient Units - A Retrospective Cohort StudyEshetu WondimuNo ratings yet
- Evaluation of Executive Functioning in People With Intellectual DisabilitiesDocument15 pagesEvaluation of Executive Functioning in People With Intellectual DisabilitiesNicol Mariana V. FernándezNo ratings yet
- VanVleet DeGutis Nons-Spatial SideDocument23 pagesVanVleet DeGutis Nons-Spatial Siderichard LemieuxNo ratings yet
- 2014 - Lees R. Et Al - Test Accuracy of Cognitive Screening Tests For Diagnosis of Dementia and Cognitive Impairment in StrokeDocument11 pages2014 - Lees R. Et Al - Test Accuracy of Cognitive Screening Tests For Diagnosis of Dementia and Cognitive Impairment in Strokerichard LemieuxNo ratings yet
- 2015 - Pendlebury S.T. Et Al - Methodological Facteors in Determining Risk of Dementia After Tia Ans StrokeDocument13 pages2015 - Pendlebury S.T. Et Al - Methodological Facteors in Determining Risk of Dementia After Tia Ans Strokerichard LemieuxNo ratings yet
- INECO Rehabilitación Clase3 Stroke PDFDocument3 pagesINECO Rehabilitación Clase3 Stroke PDFLuciana RocchiaNo ratings yet
- 2013 - Loetscher T & Lincold N.B. - Cotnivie Rehabilitation For Attention Deficits Following StrokeDocument58 pages2013 - Loetscher T & Lincold N.B. - Cotnivie Rehabilitation For Attention Deficits Following Strokerichard LemieuxNo ratings yet
- 2003 - Kawas Et Al - Visual Memory Predicts Alzheimer's DiseaseDocument5 pages2003 - Kawas Et Al - Visual Memory Predicts Alzheimer's Diseaserichard LemieuxNo ratings yet
- Stricker20et20al 202002Document12 pagesStricker20et20al 202002richard LemieuxNo ratings yet
- CIU5 L - Fabry Neuropsychologique Patient Alcoolique 1Document46 pagesCIU5 L - Fabry Neuropsychologique Patient Alcoolique 1richard LemieuxNo ratings yet
- Auditory Consonant Trigrams: Construct and Criterion Validity UpdateUpdateDocument96 pagesAuditory Consonant Trigrams: Construct and Criterion Validity UpdateUpdaterichard LemieuxNo ratings yet
- Ubc 2016 November Upshaw JenniferDocument75 pagesUbc 2016 November Upshaw Jenniferrichard LemieuxNo ratings yet
- Tele-Neuropsychological Assessment Using Video-ConferencingDocument33 pagesTele-Neuropsychological Assessment Using Video-Conferencingrichard LemieuxNo ratings yet
- Thibaudeau Achim 2018 PRDocument7 pagesThibaudeau Achim 2018 PRrichard LemieuxNo ratings yet
- California Verbal Learning Test: Performance by Patients With Focal Frontal and Non-Frontal LesionsDocument11 pagesCalifornia Verbal Learning Test: Performance by Patients With Focal Frontal and Non-Frontal LesionsAngela Bibiana Cañon OrtizNo ratings yet
- Canadian Stroke Best Practice RecommendationsDocument31 pagesCanadian Stroke Best Practice Recommendationsrichard LemieuxNo ratings yet
- Achim 2012 PR (MTZ-FEP)Document7 pagesAchim 2012 PR (MTZ-FEP)richard LemieuxNo ratings yet
- (Lab13) Uniaxial Interference Figures F12Document51 pages(Lab13) Uniaxial Interference Figures F12praveenbabu100% (1)
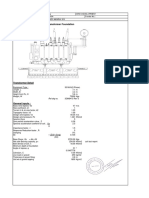
- 30 MVA Transformer Foundation DesignDocument19 pages30 MVA Transformer Foundation DesignSagun KatuwalNo ratings yet
- Module 8 - Activities AssessmentsDocument5 pagesModule 8 - Activities AssessmentsDark AxcsNo ratings yet
- Coordinate SystemsDocument43 pagesCoordinate SystemsDragan LazicNo ratings yet
- FMEA - Diesel GeneratorDocument42 pagesFMEA - Diesel GeneratorAhmed67% (3)
- Grade 2Document14 pagesGrade 2alicewongNo ratings yet
- 5s Office ImplementationDocument30 pages5s Office ImplementationHerry PrakosoNo ratings yet
- Easy CaptureDocument12 pagesEasy CaptureAndrea Sandoval RiquelmeNo ratings yet
- DSAT Practice Test 3Document56 pagesDSAT Practice Test 3hkg.cp2019No ratings yet
- A Pragmatic Legal Expert SystemDocument406 pagesA Pragmatic Legal Expert SystemJames Popple0% (1)
- Personal Project Assessment CriteriaDocument5 pagesPersonal Project Assessment Criteriaapi-345579662No ratings yet
- Thermodynamic CyclesDocument32 pagesThermodynamic CyclessunitbhaumikNo ratings yet
- OBIA Overview PDFDocument13 pagesOBIA Overview PDFDilip Kumar AluguNo ratings yet
- Project SchedulingDocument13 pagesProject SchedulingNikita Sarangpuriya100% (1)
- Taylor. ASI3 PDFDocument13 pagesTaylor. ASI3 PDFpaofrancoNo ratings yet
- Appendix A SolutionsDocument126 pagesAppendix A Solutionstechsengo100% (1)
- StsDocument8 pagesStsEdward Dimabuyu50% (10)
- Design and Simulation of DAC On The Basis of Capacitor ArrayDocument4 pagesDesign and Simulation of DAC On The Basis of Capacitor ArrayAmitNo ratings yet
- Using Matlab in Mutual Funds EvaluationDocument16 pagesUsing Matlab in Mutual Funds EvaluationMuhammad KashifNo ratings yet
- Multiple IntelligencesDocument5 pagesMultiple Intelligencesapi-278669827No ratings yet
- Community Oriented Primary Care: Book TitleDocument2 pagesCommunity Oriented Primary Care: Book Titlexxxxyyyyy1234No ratings yet
- Sample CH 4 For Experimental ResearchDocument42 pagesSample CH 4 For Experimental ResearchDennis Esik MaligayaNo ratings yet
- Car Sharing Report - Airbnb Business ModelDocument34 pagesCar Sharing Report - Airbnb Business Modelandra_36ukNo ratings yet
- CFD OpenfoamDocument4 pagesCFD OpenfoamKush VermaNo ratings yet
- A Medical Error To Disclose or Not To Disclose 2155 9627-5-174Document3 pagesA Medical Error To Disclose or Not To Disclose 2155 9627-5-174Aduda Ruiz BenahNo ratings yet
- Tans - Aqueous Ammonium Sulfate - 1958Document2 pagesTans - Aqueous Ammonium Sulfate - 1958Yulia KurniawatiNo ratings yet
- ProjectDocument44 pagesProjectewmdoNo ratings yet
- Functions of Art Lesson 4: (Source:)Document5 pagesFunctions of Art Lesson 4: (Source:)Alhaisa BejemilNo ratings yet
- Brunnstrom's Movement Therapy in Hemiplegic Patient (Lower Limb)Document71 pagesBrunnstrom's Movement Therapy in Hemiplegic Patient (Lower Limb)Barney Cordova100% (1)
- Good and Bad GraphsDocument23 pagesGood and Bad GraphsJaydee Joyce MercadoNo ratings yet