You might also like
- Zygomatic Implants: Optimization and InnovationFrom EverandZygomatic Implants: Optimization and InnovationJames ChowNo ratings yet
- Implant OlogyDocument14 pagesImplant OlogyAya M RashidiNo ratings yet
- Cad. Aided Contacts Computer.Document7 pagesCad. Aided Contacts Computer.DrAla MohamedNo ratings yet
- What Is Occ Computer.Document7 pagesWhat Is Occ Computer.DrAla MohamedNo ratings yet
- Ijss Feb Ra01Document5 pagesIjss Feb Ra01Ruxandra FitaNo ratings yet
- Radiological Templates and Cad/Cam Surgical Guides-A Literature ReviewDocument37 pagesRadiological Templates and Cad/Cam Surgical Guides-A Literature ReviewMaqbul AlamNo ratings yet
- BMC Oral Health. 2022 Feb 10 22 1 33Document10 pagesBMC Oral Health. 2022 Feb 10 22 1 33brookortontiaNo ratings yet
- Accuracy of Digital Predictions With CAD CAM Labial and L - 2018 - Seminars in O PDFDocument14 pagesAccuracy of Digital Predictions With CAD CAM Labial and L - 2018 - Seminars in O PDFOmy J. CruzNo ratings yet
- Efficacy of Implant Placement With Surgical Guides in T 2022 Advances in OraDocument6 pagesEfficacy of Implant Placement With Surgical Guides in T 2022 Advances in OraГне ДзжNo ratings yet
- Customized CAD-CAM Healing Abutment For Delayed Loaded ImplantsDocument4 pagesCustomized CAD-CAM Healing Abutment For Delayed Loaded Implantsbeautopia reviewsNo ratings yet
- Jurid GTL PDFDocument6 pagesJurid GTL PDFLutfi MabrurohNo ratings yet
- Journal Prosto PDFDocument6 pagesJournal Prosto PDFdifaNo ratings yet
- Accuracy of Miniscrew ImplantDocument8 pagesAccuracy of Miniscrew ImplantShaivi ShrivastavaNo ratings yet
- A New Bend in The Road To Successful Implant PlacementDocument9 pagesA New Bend in The Road To Successful Implant Placementerica984No ratings yet
- Types of Implant Surgical Guides in Dentistry A ReviewDocument10 pagesTypes of Implant Surgical Guides in Dentistry A Reviewmax100% (2)
- Aligner Fem1Document10 pagesAligner Fem1smhosNo ratings yet
- CAD CAM Hybrid Hyrax, AJO - PDF - BenedictDocument6 pagesCAD CAM Hybrid Hyrax, AJO - PDF - BenedictCassiana SilvaNo ratings yet
- Comparison of Digital Surface Displacements of Maxillary Dentures Based On Noninvasive Anatomic LandmarksDocument9 pagesComparison of Digital Surface Displacements of Maxillary Dentures Based On Noninvasive Anatomic LandmarksDrAhmed HamzaNo ratings yet
- Avadent Article Loma LindaDocument8 pagesAvadent Article Loma LindaRoxana LupuNo ratings yet
- Dentistry Journal: Accuracy of Digitally Fabricated Wax Denture Bases and Conventional Completed Complete DenturesDocument9 pagesDentistry Journal: Accuracy of Digitally Fabricated Wax Denture Bases and Conventional Completed Complete DenturesAruna WijayaNo ratings yet
- Marginal and Internal Fit of CAD/CAM Crowns Fabricated Over Reverse Tapered PreparationsDocument7 pagesMarginal and Internal Fit of CAD/CAM Crowns Fabricated Over Reverse Tapered PreparationsJorge HernándezNo ratings yet
- RSGDocument5 pagesRSGHugoMoralesTecnicoDentalNo ratings yet
- Implant Planning and Placement Using Optical Scanning and Cone Beam CT TechnologyDocument6 pagesImplant Planning and Placement Using Optical Scanning and Cone Beam CT TechnologyPraveen Raj ThakurNo ratings yet
- Digital Bar Prototype Technique For Full-Arch Rehabilitation On ImplantsDocument7 pagesDigital Bar Prototype Technique For Full-Arch Rehabilitation On ImplantsDragos CiongaruNo ratings yet
- PatintspecificmotionDocument8 pagesPatintspecificmotionchorv0No ratings yet
- Orentlicher 2011Document30 pagesOrentlicher 2011OctavioJose DuarteFrenkyNo ratings yet
- Three Dimensional Imaging in DentistryDocument26 pagesThree Dimensional Imaging in Dentistrydorasani99No ratings yet
- Digital WorkflowsDocument14 pagesDigital Workflowsmoji_puiNo ratings yet
- The Use The Occlusogram in Planning Orthodontic TreatnaentDocument13 pagesThe Use The Occlusogram in Planning Orthodontic TreatnaentAna Molina Coral100% (1)
- Design of A Virtual Articulator For The Simulation and Analysis of Mandibular Movements in Dental CAD-CAM-2009Document8 pagesDesign of A Virtual Articulator For The Simulation and Analysis of Mandibular Movements in Dental CAD-CAM-2009Ashish SatpathyNo ratings yet
- Rcs 2115Document21 pagesRcs 2115Kim Chi NguyễnNo ratings yet
- Guia Quirurgica 2013 ADocument10 pagesGuia Quirurgica 2013 AAlexNo ratings yet
- Movimientos Menores Con Ap EsteticosDocument6 pagesMovimientos Menores Con Ap EsteticosCATALINA VASQUEZ LOPEZNo ratings yet
- Journal of Prosthodontics - 2021 - He - The Accuracy of Transferring Casts in Maximal Intercuspal Position to a Virtual_db1e0e9921ef0b9ed0fb9bbee0d8afe9Document7 pagesJournal of Prosthodontics - 2021 - He - The Accuracy of Transferring Casts in Maximal Intercuspal Position to a Virtual_db1e0e9921ef0b9ed0fb9bbee0d8afe9kikapretty.sdNo ratings yet
- 6 - Fabrication of An Implant-Supported Overdenture Using CAD-CAM Technology A Clinical ReportDocument8 pages6 - Fabrication of An Implant-Supported Overdenture Using CAD-CAM Technology A Clinical ReportkochikaghochiNo ratings yet
- Implant DentistryDocument196 pagesImplant DentistryAkanksha MahajanNo ratings yet
- Digital Work Ow For Image-Guided Immediate Implant Placement by Using The Socket-Shield Technique and Custom Abutment in The Esthetic AreaDocument5 pagesDigital Work Ow For Image-Guided Immediate Implant Placement by Using The Socket-Shield Technique and Custom Abutment in The Esthetic AreaEduin GiraldoNo ratings yet
- Implant Surgical Guides From The Past To The PresentDocument6 pagesImplant Surgical Guides From The Past To The Presentwaf51No ratings yet
- Imp 1Document5 pagesImp 1pradeepgade1No ratings yet
- Digital Dentures A Protocol Based On Intraoral SCDocument6 pagesDigital Dentures A Protocol Based On Intraoral SCirfan dNo ratings yet
- A New Concept in Maintaining The Emergence ProfileDocument8 pagesA New Concept in Maintaining The Emergence ProfileankitaNo ratings yet
- Referensi 6Document5 pagesReferensi 6adistiharahapNo ratings yet
- Digital Work Flow of Custom AbutmentDocument10 pagesDigital Work Flow of Custom AbutmentmustafaNo ratings yet
- S - 2019 - Influence of Implant Macrodesign and Insertion Connection Technology On The Accuracy of Static Computer-Assisted Implant SurgeryDocument7 pagesS - 2019 - Influence of Implant Macrodesign and Insertion Connection Technology On The Accuracy of Static Computer-Assisted Implant SurgeryVõHoàngThủyTiênNo ratings yet
- Digital vs Elastic Impression Accuracy StudyDocument6 pagesDigital vs Elastic Impression Accuracy StudyBavilonia K PaolaNo ratings yet
- A New Concept For Implant-Borne Dental PDFDocument5 pagesA New Concept For Implant-Borne Dental PDFHélio AlvesNo ratings yet
- Digital Face Bow Transfer Technique Using The Dentofacial Analyzer For Dental Esthetics and 2 D 3 D Smile Design A Clinical ReportDocument9 pagesDigital Face Bow Transfer Technique Using The Dentofacial Analyzer For Dental Esthetics and 2 D 3 D Smile Design A Clinical ReportPaula DiazNo ratings yet
- Computational Design and Engineering of Polymeric Orthodontic AlignersDocument15 pagesComputational Design and Engineering of Polymeric Orthodontic AlignerslauNo ratings yet
- PROCERA: A New Way To Achieve An All-Ceramic CrownDocument12 pagesPROCERA: A New Way To Achieve An All-Ceramic CrownCúc Phương TrầnNo ratings yet
- Implant Placement Accuracy Using Dynamic NavigationDocument9 pagesImplant Placement Accuracy Using Dynamic NavigationMrinmayee ThakurNo ratings yet
- 10 1016@j Prosdent 2017 06 019-2Document6 pages10 1016@j Prosdent 2017 06 019-2Paulina Vargas DíazNo ratings yet
- Virtual Planning of ImplantDocument6 pagesVirtual Planning of ImplantChekkarraj Sharanya KeshapurNo ratings yet
- Analysis of Variability in The Manufacture of Cr-Co Fixed Partial Dentures by Geometric ComparisonDocument8 pagesAnalysis of Variability in The Manufacture of Cr-Co Fixed Partial Dentures by Geometric ComparisonNovita RNo ratings yet
- Literature Review on Rapid Prototyping for Surgical PlanningDocument13 pagesLiterature Review on Rapid Prototyping for Surgical PlanningvadianonymousNo ratings yet
- Background (500 Characters Max.)Document2 pagesBackground (500 Characters Max.)Stanislav StrîșcaNo ratings yet
- Digital ArticulatorDocument3 pagesDigital Articulatorshabeer hassimNo ratings yet
- JCM 09 03984Document8 pagesJCM 09 03984Zaharia NedealcovNo ratings yet
- Journal of Prosthodontics - 2019 - Hsu - Accuracy of Dynamic Virtual Articulation Trueness and Precision_5c058948bbae5731bb540176e9087ca8Document8 pagesJournal of Prosthodontics - 2019 - Hsu - Accuracy of Dynamic Virtual Articulation Trueness and Precision_5c058948bbae5731bb540176e9087ca8kikapretty.sdNo ratings yet
- Personalized Implants Restore Smiles - EDRMedesoDocument7 pagesPersonalized Implants Restore Smiles - EDRMedesovivekanandNo ratings yet
- Thanasrisuebwong - Influence of The Residual Ridge Widths and Implant Thread Designs OnDocument7 pagesThanasrisuebwong - Influence of The Residual Ridge Widths and Implant Thread Designs OnGustavo IsmaelNo ratings yet
- Torsen General Frequently Asked Questions PageDocument4 pagesTorsen General Frequently Asked Questions PagedromakiNo ratings yet
- Vigilohm System: XD301 and XD312 Automatic Insulation Fault DetectorsDocument2 pagesVigilohm System: XD301 and XD312 Automatic Insulation Fault DetectorsTeo BrăescuNo ratings yet
- ABSTRACTDocument8 pagesABSTRACTMark Benecito BoñgolNo ratings yet
- Visual Studio & C# Lecture 5: Understanding ADO.NET and Entity FrameworkDocument21 pagesVisual Studio & C# Lecture 5: Understanding ADO.NET and Entity FrameworkFarrukh zamanNo ratings yet
- Islamic States in Java 1500-1700 Eight Dutch Books and Articles by Dr. H.J. de GraafDocument90 pagesIslamic States in Java 1500-1700 Eight Dutch Books and Articles by Dr. H.J. de GraafEwinNo ratings yet
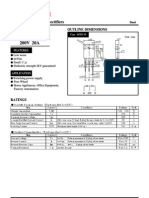
- S20LC20U S20LC20U: Shindengen ShindengenDocument6 pagesS20LC20U S20LC20U: Shindengen ShindengendaocongdablNo ratings yet
- LM5068 Negative Voltage Hot Swap Controller: General Description FeaturesDocument26 pagesLM5068 Negative Voltage Hot Swap Controller: General Description FeaturesRohit SinghNo ratings yet
- ANPR Transaction ReportDocument5 pagesANPR Transaction Reportarnab adhikariNo ratings yet
- Chap014 - JIT and Lean OperationsDocument31 pagesChap014 - JIT and Lean OperationsAgentSkySkyNo ratings yet
- Backdoors CT Case Negative - DDI 2015 SWSDocument304 pagesBackdoors CT Case Negative - DDI 2015 SWSseNo ratings yet
- Parts Manual: Generator SetDocument90 pagesParts Manual: Generator SetZez SamuelNo ratings yet
- SMC2012 CFPDocument1 pageSMC2012 CFP馮介川No ratings yet
- ARCH684 Velikov Theory Since 1989Document6 pagesARCH684 Velikov Theory Since 1989mlparedes2No ratings yet
- ZXG10 B8018 (V1.00) In-Door Base Transceiver Station Technical ManualDocument128 pagesZXG10 B8018 (V1.00) In-Door Base Transceiver Station Technical ManualPrashant MaraNo ratings yet
- L1 - 34241 - en - B - UV 420 TTR-C H4 - Pul - en - hb5Document1 pageL1 - 34241 - en - B - UV 420 TTR-C H4 - Pul - en - hb5Kara WhiteNo ratings yet
- Shielded vs Non-Shielded Cables: Changes in the NECDocument20 pagesShielded vs Non-Shielded Cables: Changes in the NECJuan AraqueNo ratings yet
- DataDocument87 pagesDataRavi KanheNo ratings yet
- Fluid Mechanics Revised ManualDocument57 pagesFluid Mechanics Revised ManualQuenNo ratings yet
- CCDP ARCH 300-320, 4th Edition-2016 PDFDocument902 pagesCCDP ARCH 300-320, 4th Edition-2016 PDFCarlos Trujillo Rojas100% (2)
- 2010-12 CR DensoDocument9 pages2010-12 CR DensoLuisCarlosKovalchukNo ratings yet
- Nebosh D guide report structureDocument2 pagesNebosh D guide report structureNorman AinomugishaNo ratings yet
- LAUSD List of AB 300 BuildingsDocument21 pagesLAUSD List of AB 300 BuildingsDennis RomeroNo ratings yet
- Instructions To Connect Database in DerbyDocument17 pagesInstructions To Connect Database in DerbyRebekkaNo ratings yet
- SMOOTH OPERATOR: How hydrostatic bearings improve cryogenic pump performanceDocument4 pagesSMOOTH OPERATOR: How hydrostatic bearings improve cryogenic pump performanceAlbertoNo ratings yet
- Kawasaki JetSki Watercraft ULTRA LX (JT1500-C7.8.9F) '07 A '09 - Service ManualDocument479 pagesKawasaki JetSki Watercraft ULTRA LX (JT1500-C7.8.9F) '07 A '09 - Service ManualGrzegorz Miąsko100% (2)
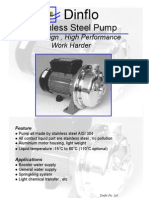
- Dinflo DFCSDocument2 pagesDinflo DFCSvictorharijantoNo ratings yet
- Master Your Network in Minutes with PRTG Network MonitorDocument6 pagesMaster Your Network in Minutes with PRTG Network MonitortranduongtinhNo ratings yet
- Sylvania KatalogDocument2 pagesSylvania KatalogCk_psihNo ratings yet
- UltraTech Cement's Kotputli Plant Wins CII Award for Energy EfficiencyDocument61 pagesUltraTech Cement's Kotputli Plant Wins CII Award for Energy EfficiencyJacky Karuppaiah100% (1)