Professional Documents
Culture Documents
Bilateral Deep Brain Stimulation Vs Best Medical Therapy For Patients With Advanced Parkinson Disease
Uploaded by
Ricardo GarciaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Bilateral Deep Brain Stimulation Vs Best Medical Therapy For Patients With Advanced Parkinson Disease
Uploaded by
Ricardo GarciaCopyright:
Available Formats
ORIGINAL CONTRIBUTION
Bilateral Deep Brain Stimulation vs
Best Medical Therapy for Patients
With Advanced Parkinson Disease
A Randomized Controlled Trial
Frances M. Weaver, PhD Context Deep brain stimulation is an accepted treatment for advanced Parkinson
Kenneth Follett, MD, PhD disease (PD), although there are few randomized trials comparing treatments, and most
Matthew Stern, MD studies exclude older patients.
Kwan Hur, PhD Objective To compare 6-month outcomes for patients with PD who received deep
brain stimulation or best medical therapy.
Crystal Harris, PharmD
Design, Setting, and Patients Randomized controlled trial of patients who re-
William J. Marks Jr, MD ceived either deep brain stimulation or best medical therapy, stratified by study site
Johannes Rothlind, PhD and patient age (⬍70 years vs ⱖ70 years) at 7 Veterans Affairs and 6 university hos-
pitals between May 2002 and October 2005. A total of 255 patients with PD (Hoehn
Oren Sagher, MD and Yahr stage ⱖ2 while not taking medications) were enrolled; 25% were aged 70
Domenic Reda, PhD years or older. The final 6-month follow-up visit occurred in May 2006.
Claudia S. Moy, PhD Intervention Bilateral deep brain stimulation of the subthalamic nucleus (n=60) or
globus pallidus (n = 61). Patients receiving best medical therapy (n = 134) were ac-
Rajesh Pahwa, MD
tively managed by movement disorder neurologists.
Kim Burchiel, MD
Main Outcome Measures The primary outcome was time spent in the “on” state
Penelope Hogarth, MD (good motor control with unimpeded motor function) without troubling dyskinesia,
Eugene C. Lai, MD, PhD using motor diaries. Other outcomes included motor function, quality of life, neuro-
cognitive function, and adverse events.
John E. Duda, MD
Results Patients who received deep brain stimulation gained a mean of 4.6 h/d of
Kathryn Holloway, MD on time without troubling dyskinesia compared with 0 h/d for patients who received
Ali Samii, MD best medical therapy (between group mean difference, 4.5 h/d [95% CI, 3.7-5.4 h/d];
P⬍.001). Motor function improved significantly (P⬍.001) with deep brain stimula-
Stacy Horn, DO tion vs best medical therapy, such that 71% of deep brain stimulation patients and
Jeff Bronstein, MD, PhD 32% of best medical therapy patients experienced clinically meaningful motor func-
Gatana Stoner, RN, CCRC tion improvements (ⱖ5 points). Compared with the best medical therapy group, the
deep brain stimulation group experienced significant improvements in the summary
Jill Heemskerk, PhD measure of quality of life and on 7 of 8 PD quality-of-life scores (P⬍.001). Neuro-
Grant D. Huang, PhD cognitive testing revealed small decrements in some areas of information processing
for patients receiving deep brain stimulation vs best medical therapy. At least 1 seri-
for the CSP 468 Study Group ous adverse event occurred in 49 deep brain stimulation patients and 15 best medical
therapy patients (P⬍.001), including 39 adverse events related to the surgical pro-
D
EEP BRAIN STIMULATION IS
cedure and 1 death secondary to cerebral hemorrhage.
the surgical intervention of
choice when Parkinson dis- Conclusion In this randomized controlled trial of patients with advanced PD, deep
ease (PD) motor complica- brain stimulation was more effective than best medical therapy in improving on time
without troubling dyskinesias, motor function, and quality of life at 6 months, but was
tions are inadequately managed with
associated with an increased risk of serious adverse events.
medications. Ideal candidates have fluc-
tuating motor symptoms or medication- Trial Registration clinicaltrials.gov Identifier: NCT00056563
related adverse effects, few comorbidi- JAMA. 2009;301(1):63-73 www.jama.com
ties, and no cognitive or behavioral
Author Affiliations and Members of the CSP 468 VA Hospital, Center for Management of Complex
For editorial comment see p 104. Study Group are listed at the end of this article. Chronic Care, 5000 S Fifth Ave (151H), Hines, IL 60141
Corresponding Author: Frances M. Weaver, PhD, Hines (Frances.Weaver@va.gov).
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 63
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
disorders. 1 This younger, healthier METHODS pharmacological therapy (eg, physical,
population reflects a selection bias ob- Study Sites and Patients occupational, and speech therapy) as
served in most deep brain stimulation Seven Veterans Affairs and 6 affiliated needed to achieve best symptom con-
studies.2,3 The typical patient with PD university medical centers enrolled 255 trol and optimal functioning.
is older and has other medical condi- patients between May 2002 and Octo- Patients who received deep brain
tions. ber 2005. Study sites were selected on stimulation were further randomized to
Deep brain stimulation for PD en- a competitive basis and required the subthalamic nucleus or globus palli-
tered widespread clinical use in the late participation of a movement disorder dus targets and underwent surgery
1990s and acceptance of this therapy neurologist, a surgeon with expertise within 1 month. Patients were blinded
has increased over the past 15 years. in globus pallidus and subthalamic to the target. The study was con-
The attractiveness of deep brain stimu- nucleus deep brain stimulation im- ducted under an investigational de-
lation is related in part to the fact that plants and microelectrode recording, vice exemption because the deep brain
stimulation is adjustable and revers- and appropriate supportive services (eg, stimulation system (Kinetra system,
ible.4 However, recent reports high- neuropsychologists). Patients with id- Medtronic Inc, Minneapolis, Minne-
lighting unexpected behavioral effects iopathic PD were eligible if they were sota) was not approved for use by the
of stimulation suggest that deep brain classified as Hoehn and Yahr stage 2 or US Food and Drug Administration
stimulation, while improving motor greater while not taking medication8; when the study began. Patients under-
function, may have other less desir- were responsive to levodopa; had per- went bilateral deep brain stimulation
able consequences.5,6 The popularity of sistent disabling symptoms (eg, motor lead implantation while awake, dur-
deep brain stimulation belies the fact fluctuations, dyskinesia) despite medi- ing 1 procedure whenever possible;
that its utility relative to medical therapy cation; experienced 3 or more hours per however, some patients returned for
has been studied only in uncontrolled 24-hour period with poor motor func- the second lead implant due to patient
studies, with 1 recent exception.7 tion or symptom control; were receiv- fatigue or technical issues. Lead im-
Deuschl et al7 reported significant im- ing stable medical therapy for 1 month plantation was accomplished using
provement in patient outcomes follow- or longer; and were aged 21 years or stereotactic frames (Leksell, Elekta,
ing deep brain stimulation of the sub- older. Exclusion criteria included atypi- Stockholm, Sweden or CRW, Integra
thalamic nucleus, but also pointed out cal syndromes, previous surgery for PD, Radionics, Burlington, Massachu-
that not all patients who received deep surgical contraindications, active alco- setts) with magnetic resonance imaging,
brain stimulation improved. Quality- hol or drug abuse, dementia,9 or preg- computed tomographic guidance, or
of-life outcomes favored deep brain nancy. Patients were not required to both. Initial targets were based on stan-
stimulation for 64% and favored medi- have a caregiver. The study was ap- dard coordinates for subthalamic
cal therapy in 36% of PD pairs random- proved by each site’s institutional re- nucleus and globus pallidus.
ized to deep brain stimulation or medi- view board and patients provided writ- Intraoperative microelectrode re-
cal therapy. Similarly, although deep ten informed consent. Race/ethnicity cording and test stimulation were man-
brain stimulation resulted in im- information was collected to deter- datory to optimize uniformity of im-
proved motor functioning in 71% of mine what proportion of study partici- plant technique and target localization.
pairs, the functioning was better in 27% pants were in minority groups. Microelectrode recording was ex-
of the cases for the medically treated pected to demonstrate neuronal activ-
patients. Randomization and Blinding ity stereotypical for subthalamic nucleus
The present study is, to our knowl- Randomization to deep brain stimula- or globus pallidus targets. Intraopera-
edge, the first large, multicenter, moni- tion or best medical therapy included tive test stimulation was performed to
tored, randomized controlled, blinded stratification by study site and patient assess improvement of parkinsonian
assessment trial to compare the ben- age (⬍70 years vs ⱖ70 years). Motor signs and occurrence of stimulation-
efits and risks of deep brain stimula- function assessments were conducted induced adverse effects.
tion with those of best medical therapy by raters blinded to treatment. All surgeons had significant pre-
for patients with PD who span a wide study expertise with deep brain stimu-
age range. It is the first phase of an on- Interventions lation surgery and microelectrode re-
going study that also will compare out- Patients who received best medical cording involving the subthalamic
comes based on a surgical target for therapy were managed actively by nucleus and globus pallidus and used
deep brain stimulation (subthalamic study movement disorder neurologists their clinical judgment to identify the
nucleus vs globus pallidus) over 2 years. after randomization. Neurologists best location for lead implantation. Lead
For the present study, the target sites applied state-of-the-art care, including position was revised from the original
were combined into a single group to adjuvant medication, and made target at the discretion of the surgeon
address the question of the surgical vs adjustments to the dosages, frequency, based on the results of microelectrode
the medical intervention. or timing of medication, and to non- recording and test stimulation. The neu-
64 JAMA, January 7, 2009—Vol 301, No. 1 (Reprinted) ©2009 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
rostimulator was usually implanted A neurocognitive test battery was ad- complete for 2 consecutive days prior
(under general anesthesia) on the same ministered by a neuropsychologist, usu- to the visit.
day immediately following lead implan- ally on a different day than the motor Abbreviated motor function and
tation. Once the stimulator was turned assessments to reduce patient burden. quality-of-life assessments were con-
on, patients in the deep brain stimula- Measures included the Mattis Demen- ducted at 3 months. The entire base-
tion group received continuous stimu- tia Rating Scale9 and standardized tests line assessment was repeated at 6
lation. Patients returned as needed for of attention, working memory, visuo- months. Study neurologists and blinded
stimulation-parameter adjustments motor speed taken from the Wechsler neurologists independently assessed
using a standardized protocol to maxi- Adult Intelligence Scales III, verbal as- patients’ UPDRS motor scores while
mize symptom control and minimize sociative fluency, other aspects of ex- patients were not taking medication.
adverse effects. Stimulation and medi- ecutive functioning (Stroop Test, Wis- Patients receiving deep brain stimula-
cation adjustments were conducted by consin Card Sorting Test) and language tion kept their stimulators on for the
clinicians unblinded to treatment. (Boston Naming Test), learning and first assessment, then had them deac-
memory (Brief Visuospatial Memory tivated for return 1 hour later for assess-
Study Procedures Test and Hopkins Verbal Learning Test, ment off medication, off stimulation.
Recruitment included referrals to study with alternate forms at each assess- Patients receiving best medical therapy
neurologists and patient self-referral. In- ment), manual tapping speed, and remained off medication and returned
formed consent and baseline assess- mood. for a second assessment to equalize
ments were obtained if initial review by Patients with advanced PD often ex- assessments in each group. After the
the study nurse indicated the patient was perience motor function fluctuations second assessment, the deep brain
eligible. Patients came to the clinic hav- throughout the day, resulting in peri- stimulation systems were reactivated.
ing stopped their PD medications the ods of good symptom control or un- All patients took their medications and
night before.10 Patients completed the impeded motor function (classified as returned 1 hour later for a third blinded
Mini-Mental State Examination11 and “on” time), and periods of poor symp- and unblinded assessment. Patients
those who scored less than 25 were ex- tom control and impaired motor func- completed the remaining assessments,
cluded from the trial. The movement dis- tion (classified as “off” time). On time including the UPDRS and neurocogni-
order neurologist completed the Uni- may include involuntary movements tive tests, while taking medication.
fied Parkinson Disease Rating Scale (dyskinesia). Self-report motor dia- Adverse events were collected and
(UPDRS)12 motor subscale while the pa- ries are a validated method to capture coded as to whether they were caus-
tient was not taking medication. A sec- this information.15 Training on diary ally related to the study device, PD pro-
ond neurologist, blinded to treatment, completion was conducted by the nurse gression, PD medication, stimulation
independently completed the motor sub- and included instructions and ex- therapy, or surgical procedure. Each ad-
scale. To ensure blinded assessments ample diaries, review of a motor fluc- verse event was recorded as being mild,
during follow-up, all patients wore caps tuation videotape,16 and completion of moderate, or severe. Grading of the se-
to cover evidence of possible cranial sur- practice diaries. Patients recorded verity of the adverse event was de-
gery and clothing to cover any incision which of 4 categories (on, on with trou- cided by the site primary investigator.
for the neurostimulator. Patients then bling dyskinesia, off, or asleep) best re- In post hoc analyses conducted to iden-
took their PD medications, and assess- flected their predominant functioning tify events due to early effects of sur-
ments were repeated 1 hour later by 1 for the prior 30 minutes in half-hour gery and stimulation adjustment, ad-
neurologist. If patients had not at- intervals for 2 days.15 Total time spent verse events were divided into those
tained their best functioning, addi- in each category was summed and av- that occurred within 3 months posten-
tional medications could be taken to eraged over 2 days to determine study rollment and those occurring at 4 to 6
reach optimum functioning. eligibility. Patients were unaware of the months. Some adverse events were fur-
When the patient was taking medi- 3-hour off time and/or on time with ther categorized as serious, defined as
cation, the movement disorder neu- troubling dyskinesia per day eligibil- any event that was life-threatening, re-
rologist assessed the patient using the ity requirement when completing the sulted in prolonged or new hospital-
Hoehn and Yahr8 and Schwab and En- diaries. ization, disability or congenital anomaly
gland13 scales. The patient performed or birth defect, death, or required medi-
the stand-walk-sit test 10 and com- Follow-up cal or surgical intervention to prevent
pleted the other UPDRS subscales12 and Patients returned to their study site at 1 of the above outcomes.
the Parkinson Disease Questionnaire 3 and 6 months for this phase of the
39.14 The nurse recorded usual medi- study. The final follow-up visits for this Statistical Analysis
cations taken and assessed the pa- phase of the study occurred in May Analyses were based on the intent-to-
tient’s physical health status and PD 2006. Ten days prior to each visit, pa- treat principle. For patients with at
symptoms. tients were mailed motor diaries to least 1 follow-up visit but incomplete
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 65
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
follow-up, the last observation was calculated. Statistical significance was The target sample size of 316 individu-
carried forward and treated as the based on the 95% confidence interval als included an anticipated 10% drop-
6-month observation. For patients (CI) for the incidence risk ratio. Analy- out in the best medical therapy group.
without baseline data, follow-up data, ses were performed using SAS soft- To recruit the target sample size
or both, the change score was set to ware version 9.1 (SAS Institute Inc, needed for the phase 2 comparison of
zero. A second analysis excluded those Cary, North Carolina). All statistical globus pallidus and subthalamic nucleus
without follow-up or baseline data. tests were 2-sided. deep brain stimulation without further
The primary outcome was the baseline The sample size calculation was based extending the study timeline, the data
to 6-month change in time spent in on the primary outcome, which was the and safety monitoring board requested
the on state without troubling dyski- time spent in the on state without dys- an interim analysis for efficacy on the first
nesia. The mean group change was kinesia. The Cohen effect size was used 214 patients. Results indicated that ran-
compared between treatment groups to compare the difference in the aver- domization to the best medical therapy
using a 2-sample t test. Secondary out- age number of on hours between the group could be discontinued. The nomi-
comes were measured as baseline to best medical therapy group and the deep nal significance level for the final analy-
6-month changes. brain stimulation group.18 All sample sis of the primary outcome was retro-
Medication usage was converted to sizes and power calculations were spectively set to .049.
levodopa equivalents for analysis.17 An 2-tailed with an ␣ level of .05. The origi- Average differences in outcomes be-
incidence risk ratio, the ratio of seri- nal sample size of 300 individuals tween best medical therapy and deep
ous adverse event incidence rates per permitted 99% and 93% power for brain stimulation in the intent-to-treat
patient for deep brain stimulation com- detecting effect sizes of 0.5 and 0.4, group (n=255) were slightly smaller than
pared with best medical therapy, was respectively, in the primary outcome. those for the group with at least 1 fol-
low-up visit (n = 230). However, be-
cause results for the 2 analyses were simi-
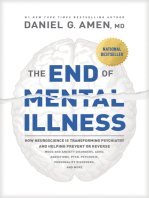
Figure. Patient Enrollment and Randomization Assignment
lar, only the former is presented.
278 Individuals screened for eligibility
RESULTS
23 Excluded A total of 255 patients with PD were ran-
11 Not willing to participate in domized to receive best medical therapy
follow-up study procedures
7 Neuropsychological dysfunction (n=134) or bilateral deep brain stimu-
2 Not responsive to levodopa
1 Disabling symptoms <3 h/d lation (n=121; of these patients, 61 were
1 Mini-Mental State Examination additionally randomized to globus pal-
score ≤24
1 Medical contraindication to lidus and 60 to subthalamic nucleus)
surgery and/or stimulation (FIGURE). Nineteen patients did not
complete any follow-up assessments be-
255 Randomized
cause they withdrew consent (9 in the
deep brain stimulation group and 9 in
134 Assigned to receive best 121 Assigned to receive deep
medical therapy brain stimulation
the best medical therapy group), died
(1 in the deep brain stimulation group),
61 Randomized to receive
or were administratively withdrawn
globus pallidus stimulation when the best medical therapy inter-
60 Randomized to receive vention group was closed (n=6). Base-
subthalamic nucleus
stimulation line characteristics for patients with no
follow-up did not differ from those who
119 Assessed at 3 mo 111 Assessed at 3 mo continued in the study except for mean
7 Withdrew consent 2 Withdrew consent
2 Withdrew because randomized 7 Withdrew due to medical or
age (67.6 years for noncompleters vs
to best medical therapy psychological problem 62.0 years for completers; P =.01). Of
6 Withdrew administratively when 1 Died
best medical therapy group the 255 patients included in the pri-
was closed mary analysis, 211 completed 3-month
evaluations and 224 completed
116 Assessed at 6 mo 108 Assessed at 6 mo
3 No follow-up data 3 No follow-up data 6-month evaluations.
Patients were male (82%), white
134 Included in primary analysis 121 Included in primary analysis (96%), and married (69%), had a mean
(SD) age of 62.4 (8.9) years (range,
A score of 24 or less on the Mini-Mental State Examination is indicitive of cognitive impairment, which met the 37-83 years), and it had been a mean
exclusion criteria for the study.
(SD) of 12.4 (5.8) years since diagno-
66 JAMA, January 7, 2009—Vol 301, No. 1 (Reprinted) ©2009 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
sis of PD. One-quarter were aged 70 TABLE 3). Similarly, in those aged 70 point in the best medical therapy group
years or older. Overall, the baseline years or older, motor function im- (P ⬍.001). The UPDRS scores for ac-
characteristics did not differ between proved 9.9 points in the deep brain tivities of daily living and complica-
the best medical therapy and deep brain stimulation group compared with 1 tions of therapy also improved signifi-
stimulation groups (TABLE 1). How-
ever, the best medical therapy pa-
Table 1. Patient Baseline Characteristics by Treatment Group
tients were treated with PD medica-
Best Medical Deep Brain
tions for a longer time (12.6 vs 10.8 Therapy Stimulation P
years for deep brain stimulation pa- (n = 134) (n = 121) Value
tients; P=.01) and had a lower work- No. (%)
Age ⱖ70 y 37 (27.6) 31 (25.6) .78
ing memory index (97.3 vs 101.2, re-
Men 110 (82.1) 98 (81.0) .87
spectively; P = .02). Patients receiving
VA patient 80 (59.7) 73 (60.3) ⬎.99
best medical therapy and deep brain
White race 128 (95.5) 117 (96.7) .75
stimulation did not differ on either av-
Married 95 (70.9) 81 (66.9) .50
erage hours per day in the on state with-
Living with family 102 (76.1) 100 (82.6) .37
out troublesome dyskinesia (7.0 vs 6.4 Has personal caregiver help 60 (44.8) 56 (46.3) .90
hours per day; P= .07), UPDRS score, Family history of Parkinson disease 32 (23.9) 32 (26.4) .67
or quality-of-life measures.
Mean (SD)
Age, y 62.3 (9.0) 62.4 (8.8) .97
Motor Diary
Years taking Parkinson disease medications 12.6 (5.6) 10.8 (5.4) .01
Deep brain stimulation patients gained Not taking medication
a mean of 4.6 hours per day of on time Hoehn and Yahr scale (range, 0-5) a 3.3 (0.8) 3.4 (0.9) .85
without troubling dyskinesia, while the Schwab and England scale (range, 0-100) b 51.0 (19.7) 50.4 (20.5) .80
mean change for the best medical Unified Parkinson Disease Rating Scale score a
I (mentation, behavior, and mood; range, 0-16) 2.7 (2.0) 2.6 (2.0) .69
therapy group was 0 hours (95% CI,
II (activities of daily living; range, 0-52) 19.7 (6.1) 19.1 (5.9) .44
3.7-5.4, P⬍.001; TABLE 2). Off time de-
III (motor function while not taking medication, blinded 43.2 (11.3) 43.0 (13.5) .88
creased by 2.4 hours per day and on assessment; range, 0-108)
time with troubling dyskinesia by 2.6 IV (complication of therapy; range, 0-23) 9.3 (3.1) 9.2 (3.0) .79
hours per day in patients in the deep On time, h/d
brain stimulation group compared with Without troublesome dyskinesia 7.0 (2.9) 6.4 (2.7) .07
0 and 0.3 hours per day in patients in Wth troublesome dyskinesia 4.2 (3.1) 4.4 (3.1) .59
the best medical therapy group Parkinson Disease Questionnaire 39 score (range, 0-100) a
Mobility 58.4 (21.4) 61.1 (21.0) .30
(P⬍.001). Asleep time did not change
Activities of daily living 54.8 (18.8) 55.0 (17.6) .92
significantly over time by group. Among
Emotional well-being 39.7 (18.6) 38.4 (19.3) .57
those aged 70 years or older, patients
Social support 26.0 (18.0) 26.9 (19.6) .71
receiving deep brain stimulation gained Beck Depression Inventory score (range, 0-63) a 11.7 (8.1) 11.3 (8.7) .68
an average of 3.8 hours of on time per Mattis Dementia Rating Scale score (range, 0-144) b 136.6 (5.8) 136.7 (4.8) .84
day, whereas patients receiving best Processing Speed Index score (range, 54-150) b,c 89.4 (14.1) 91.0 (13.9) .37
medical therapy lost 0.5 hours per day WAIS-III Working Memory Index score (range, 50-150) b,d 97.3 (13.6) 101.2 (13.3) .02
(P⬍.001). Phonemic fluency b,e 44.7 (12.1) 45.7 (12.1) .52
Category fluency (animal) b,e 49.5 (11.6) 50.9 (11.3) .34
Motor Function
Hopkins Verbal Learning Test b,e
The change in off-medication UPDRS Total (learning or memory) 39.9 (11.5) 38.9 (11.3) .50
motor scores over 6 months was sig- Delayed recall 38.1 (13.4) 37.3 (13.3) .62
nificantly greater in the deep brain Finger tapping b,e 37.6 (12.9) 37.1 (11.4) .75
stimulation group than in the best Boston Naming Test (language) b,e 55.9 (4.3) 55.5 (4.5) .44
medical therapy group based on WCST perseverative response b,e 43.7 (12.2) 46.1 (13.0) .13
blinded-rater evaluations (in only 2% Stroop interference b,e 51.0 (7.6) 50.7 (7.4) .71
of cases did blinded raters believe they Brief Visuospatial Memory Test b,e
Delayed recall 42.4 (13.3) 42.1 (13.3) .86
knew which intervention the patient re-
Total 39.7 (11.8) 39.0 (12.5) .68
ceived). Motor functioning improved
Abbreviations: VA, Veterans Affairs; WAIS-III, Wechsler Adult Intelligence Scales III; WCST, Wisconsin Card Sorting Test.
(decreased) by 12.3 points in the deep a Higher score indicates worse functioning.
b Higher score indicates better functioning.
brain stimulation group and by 1.7 c Indicates symbol search plus digit symbol.
d Indicates arithmetic plus letter-number plus digit span.
points in the best medical therapy group e These scales have a normal mean (SD) of 50 (10) and are T-scores.
while not taking medication (P⬍.001;
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 67
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
Table 2. Patient Motor Diary Outcomes
Best Medical Therapy
Best Medical Therapy Deep Brain Stimulation Minus
(n = 134) (n = 121) Deep Brain Stimulation
Mean Mean Mean
Baseline, 6 mo, Difference Baseline, 6 mo, Difference Difference P
Time Mean (SD) Mean (SD) (95% CI) Mean (SD) Mean (SD) (95% CI) (95% CI) Value a
On, h/d b
Without troublesome 7.0 (2.9) 7.1 (3.3) 0 6.4 (2.7) 10.9 (4.2) 4.6 −4.5 ⬍.001
dyskinesia (−0.5 to 0.5) (3.8 to 5.3) (−5.4 to −3.7)
With troublesome 4.2 (3.1) 3.9 (3.3) −0.3 4.4 (3.1) 1.8 (3.0) −2.6 2.3 ⬍.001
dyskinesia (−0.8 to 0.3) (−3.3 to −2.0) (1.5 to 3.2)
Off, h/d b 5.6 (2.9) 5.7 (2.8) 0 5.9 (2.6) 3.4 (3.1) −2.4 2.5 ⬍.001
(−0.4 to 0.5) (−3.1 to −1.8) (1.7 to 3.2)
Asleep, h/d 7.1 (1.7) 7.3 (2.0) 0.3 7.3 (1.8) 7.7 (2.0) 0.4 −0.1 .66
(0 to 0.6) (0 to 0.7) (−0.6 to 0.4)
Abbreviation: CI, confidence interval.
a Test for the change scores from baseline to 6 months between the best medical therapy group and the deep brain stimulation group.
b “On” and “off” time are described in the “Study Procedures” section of the “Methods.”
cantly in the deep brain stimulation 7 of 8 Parkinson Disease Question- played mild decrements in perfor-
group compared with the best medi- naire 39 subscales compared with pa- mance (1.0- to 3.5-point decreases).
cal therapy group (P⬍.001 for all com- tients who received best medical Neither treatment was associated with
parisons). When data were reexam- therapy, who had little change from significant change on the Mattis de-
ined using a 5-point change in UPDRS baseline on any subscale except stigma mentia or Beck depression scales or the
motor score as a measure of a minimal (Table 3). Social support scores did not majority of the measures assessing lan-
clinically important change,19 71% of change significantly as a result of in- guage, executive functioning, and learn-
deep brain stimulation patients vs 32% tervention. Older patients receiving ing and memory functioning.
of best medical therapy patients showed deep brain stimulation experienced sig-
improvement in motor function at 6 nificantly greater improvements in mo- Adverse Events
months (P ⬍ .001), while 3% of deep bility, activities of daily living, and Deep brain stimulation patients re-
brain stimulation patients and 21% of stigma subscales but did not differ in ported 659 moderate or severe ad-
best medical therapy patients had clini- other subscales from older patients re- verse events and best medical therapy
cally worsening scores (P ⬍.001). Re- ceiving best medical therapy (results not patients reported 236 moderate or
sults were similar when only those aged shown). severe adverse events. The most fre-
70 years or older were examined (61% quent adverse events were falls, gait
of deep brain stimulation patients vs Neurocognitive Function disturbance, dyskinesia, motor dys-
27% of best medical therapy patients ex- The deep brain stimulation and best function, balance disorder, depres-
periencing clinically improved motor medical therapy groups were gener- sion, and dystonia (ⱖ9% patients for
function; P ⬍ .006). While the deep ally well matched with regard to base- each). During the 6-month follow-up,
brain stimulation group had 9.0- line neuropsychological test perfor- there were significantly more events for
second improvements in their stand- mance. However, the deep brain the deep brain stimulation group than
walk-sit test, patients in the best medi- stimulation group performed signifi- the best medical therapy group for falls
cal therapy group had worsening of cantly better (P = .02) on working (P ⬍ .01), gait disturbance (P = .03),
their time by an average of 0.2 sec- memory at baseline. There were statis- depression (P = .03), and dystonia
onds from baseline (P = .046). Medica- tically significant treatment differ- (P⬍.01). Surgical site infection (9.9%)
tion (in levodopa equivalents) de- ences in the change between baseline and surgical site pain (9.0%) occurred
creased by 296 mg for patients in the and follow-up on composite measures only in the deep brain stimulation
deep brain stimulation group and in- of working memory (P=.005), process- group. There was no study site varia-
creased by 15 mg over baseline for pa- ing speed (P = .006), phonemic flu- tion in infection rates, ranging from 0
tients in the best medical therapy group ency (P ⬍.001), and delayed recall on to 2 infections per site.
(P⬍ .001). the Brief Visuospatial Memory Test Most differences in adverse events be-
(P = .03; Table 3). Whereas the best tween the 2 groups occurred in the first
Quality of Life medical therapy group showed slightly 3 months; only falls and dystonia were
Patients who received deep brain stimu- improved performance (1- to 2-point significantly greater for the deep brain
lation experienced significant improve- increases) at follow-up, patients in the stimulation group than for the best
ments on the summary measure and on deep brain stimulation group dis- medical therapy group in the later 3
68 JAMA, January 7, 2009—Vol 301, No. 1 (Reprinted) ©2009 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
months (TABLE 4). The majority of ad- Forty-nine deep brain stimulation adverse events (83%) were attributed
verse events (83%) in both groups had patients (40%) experienced 82 serious to the surgical procedure, stimulation
resolved by the 6-month follow-up. adverse events. Sixty-eight serious device, or stimulation therapy. Of the
Table 3. Outcomes at Baseline and 6 Months by Treatment Group a
Best Medical Therapy
Minus
Best Medical Therapy Deep Brain Stimulation Deep Brain
(n = 134) (n = 121) Stimulation
Mean Mean Mean
Difference Difference Difference P
Outcome Baseline 6 mo (95% CI) Baseline 6 mo (95% CI) (95% CI) Value b
Not taking medication
Hoehn and Yahr c 3.3 (0.8) 3.4 (0.9) 0 3.4 (0.9) 2.8 (0.9) −0.5 0.5 ⬍.001
(−0.1 to 0.1) (−0.7 to −0.4) (0.3 to 0.7)
Schwab and England d 51.0 (19.7) 49.3 (19.5) −1.7 50.4 (20.5) 66.2 (22.1) 15.8 −17.5 ⬍.001
(−4.2 to 0.8) (11.6 to 20.0) (−22.2 to −12.8)
Stand-walk-sit, s 36.3 (37.9) 36.9 (62.2) −0.2 34.6 (36.7) 25.2 (24.1) −9.0 8.8 .05
(−6.6 to 6.2) (−14.8 to −3.3) (0.1 to 17.5)
Unified Parkinson Disease Rating Scale score c
I (mentation, behavior, and mood) 2.7 (2.0) 3.0 (2.1) 0.3 2.6 (2.0) 2.6 (2.3) 0 0.3 .30
(−0.1 to 0.6) (−0.4 to 0.4) (−0.2 to 0.8)
II (activities of daily living) 19.7 (6.1) 19.7 (5.9) 0 19.1 (5.9) 14.5 (6.9) −4.6 4.6 ⬍.001
(−0.6 to 0.6) (−5.8 to −3.5) (3.4 to 5.9)
III (motor function, blinded assessment when)
Taking medication e 23.4 (11.1) 23.1 (11.7) −0.4 22.6 (12.6) 20.3 (11.3) −2.4 2.0 .08
(−1.9 to 1.2) (−4.0 to −0.8) (−0.2 to 4.2)
Not taking medication f 43.2 (11.3) 41.6 (12.7) −1.7 43.0 (13.5) 30.7 (14.5) −12.3 10.6 ⬍.001
(−3.3 to −0.1) (−14.3 to −10.3) (8.1 to 13.2)
IV (complications of therapy) 9.3 (3.1) 8.8 (3.2) −0.5 9.2 (3.0) 5.8 (3.0) −3.4 2.9 ⬍.001
(−0.9 to 0) (−4.0 to −2.7) (2.1 to 3.7)
Levodopa equivalents, mg g 1289 (546) 1303 (532) 15 1281 (521) 985 (633) −296 310 ⬍.001
(−44 to 73) (−415 to −176) (182 to 439)
Quality of Life
Parkinson Disease Questionnaire 39 score c
Mobility 58.4 (21.4) 58.0 (22.2) −0.3 61.1 (21.0) 48.8 (25.2) −12.3 12.0 ⬍.001
(−2.5 to 1.8) (−15.9 to −8.7) (7.9 to 16.1)
Activities of daily living 54.8 (18.8) 56.3 (19.1) 1.5 55.0 (17.6) 41.0 (22.2) −14.0 15.5 ⬍.001
(−0.6 to 3.7) (−17.1 to −11.0) (11.9 to 19.2)
Emotional well-being 39.7 (18.6) 38.4 (18.5) −1.3 38.4 (19.3) 32.6 (19.5) −5.7 4.4 .02
(−3.7 to 1.1) (−8.6 to −2.8) (0.7 to 8.2)
Stigma 44.0 (24.5) 39.8 (25.5) −4.2 40.6 (24.3) 28.2 (23.7) −12.5 8.3 .001
(−7.1 to −1.2) (−16.4 to −8.6) (3.6 to 13.1)
Social support 26.0 (18.0) 27.5 (19.0) 1.5 26.9 (19.6) 25.1 (21.1) −1.7 3.2 .17
(−1.7 to 4.6) (−5.1 to 1.7) (−1.4 to 7.8)
Cognition 42.2 (17.9) 43.8 (16.6) 1.7 40.4 (17.8) 36.7 (20.4) −3.7 5.3 .01
(−1.0 to 4.3) (−6.8 to −0.5) (1.3 to 9.4)
Communication 45.2 (17.9) 47.8 (18.5) 2.6 45.3 (20.0) 42.6 (22.6) −2.7 5.2 .01
(0.3 to 4.8) (−6.2 to 0.8) (1.2 to 9.3)
Bodily discomfort 47.6 (21.6) 48.6 (24.3) 1.1 51.2 (21.2) 44.0 (21.1) −7.2 8.3 ⬍.001
(−2.0 to 4.1) (−10.5 to −4.0) (3.8 to 12.7)
Single index 44.3 (13.1) 44.8 (13.4) 0.4 44.9 (13.2) 37.3 (16.0) −7.7 8.1 ⬍.001
(−1.0 to 1.8) (−9.7 to −5.6) (5.6 to 10.5)
Neurocognitive Tests
Beck Depression Inventory score c 11.7 (8.1) 10.2 (6.9) −1.5 11.3 (8.7) 10.9 (8.6) −0.4 −1.0 .22
(−2.6 to −0.3) (−1.7 to 0.9) (−2.7 to 0.6)
Mattis Dementia Rating Scale total score d 136.6 (5.8) 137.5 (5.5) 0.9 136.7 (4.8) 136.6 (6.7) −0.2 1.1 .12
(0.1 to 1.7) (−1.3 to 0.9) (−0.3 to 2.4)
Wechsler Adult Intelligence Scales III d
Working memory index h 97.3 (13.6) 98.3 (14.9) 1.0 101.2 (13.3) 99.6 (13.6) −1.6 2.6 .005
(−0.2 to 2.2) (−3.0 to −0.2) (0.8 to 4.4)
Processing speed index i 89.4 (14.1) 90.1 (13.9) 0.7 91.0 (13.9) 88.4 (14.3) −2.1 2.9 .006
(−0.7 to 2.2) (−3.6 to −0.6) (0.8 to 4.9)
(continued)
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 69
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
Table 3. Outcomes at Baseline and 6 Months by Treatment Group a (continued)
Best Medical Therapy
Best Medical Therapy Deep Brain Stimulation Minus
(n = 134) (n = 121) Deep Brain Stimulation
Mean Mean Mean
Difference Difference Difference P
Outcome Baseline 6 mo (95% CI) Baseline 6 mo (95% CI) (95% CI) Value b
Neurocognitive Tests
Phonemic fluency d,j 44.7 (12.1) 45.7 (11.8) 1.1 45.7 (12.1) 42.2 (12.3) −3.5 4.6 ⬍.001
(−0.3 to 2.6) (−4.9 to −2.0) (2.5 to 6.6)
Category (animal) fluency d,j 49.5 (11.6) 47.4 (11.9) −2.0 50.9 (11.3) 46.2 (11.3) −4.7 2.6 .06
(−4.0 to −0.1) (−6.6 to −2.7) (−0.2 to 5.4)
Boston Naming Test d,j 55.9 (4.3) 56.2 (4.0) 0.3 55.5 (4.5) 56.2 (3.8) 0.7 −0.4 .13
(0 to 0.6) (0.3 to 1.1) (−0.8 to 0.1)
Finger tapping d,j 37.6 (12.9) 38.7 (13.2) 1.0 37.1 (11.4) 36.9 (11.3) −0.2 1.3 .32
(−0.7 to 2.7) (−2.1 to 1.6) (−1.2 to 3.8)
Stroop interference d,j 51.0 (7.6) 51.8 (8.4) 0.7 50.7 (7.4) 49.8 (7.1) −0.9 1.6 .11
(−0.7 to 2.1) (−2.2 to 0.4) (−0.4 to 3.5)
WCST perseveration response d,j 43.7 (12.2) 45.0 (11.5) 1.3 46.1 (13.0) 45.8 (12.6) −0.3 1.6 .29
(−0.9 to 3.4) (−2.4 to 1.7) (−1.4 to 4.6)
Hopkins Verbal Learning Test d,j
Total (learning or memory) 39.9 (11.5) 40.2 (11.2) 0.3 38.9 (11.3) 39.0 (11.3) 0 (−1.8 to 1.9) 0.3 .82
(−1.3 to 2.0) (−2.2 to 2.7)
Delayed recall 38.1 (13.4) 37.6 (13.4) −0.5 37.3 (13.3) 35.9 (12.9) −1.4 0.8 .52
(−2.4 to 1.4) (−3.1 to 0.4) (−1.7 to 3.4)
Brief Visuospatial Memory Test d,j
Total 39.7 (11.8) 40.0 (12.4) 0.3 39.0 (12.5) 38.3 (12.4) −0.7 1.1 .45
(−1.5 to 2.2) (−2.9 to 1.5) (−1.7 to 3.9)
Delayed recall 42.4 (13.3) 44.6 (13.7) 2.2 42.1 (13.3) 41.1 (13.6) −1.0 3.2 .03
(0.2 to 4.1) (−3.1 to 1.0) (0.4 to 6.0)
Abbreviations: CI, confidence interval; WCST, Wisconsin Card Sorting Test.
a See Table 1 for the score range for each test. Values are expressed as mean (SD) unless otherwise indicated.
b Test for change scores from baseline to 6 mo between the best medical therapy group and the deep brain stimulation group.
c Higher score indicates worse functioning.
d Higher score indicates better functioning.
e Patient was taking medication (and receiving stimulation if in deep brain stimulation group); blinded assessment.
f Patient was not taking medication (and receiving stimulation if in deep brain stimulation group); blinded assessment.
g A dose of 100 mg of levodopa is equal to 125 mg of controlled-release levodopa is equal to 10 mg of bromocriptine is equal to 1 mg of pergolide is equal to 4 mg of ropinrirole is equal
to 100 mg of amantadine is equal to 2 mg of trihexyphenidyl is equal to 10 mg of seligiline is equal to 2 mg of cogentin (based on expert opinion plus Pahwa et al17).
h Includes arithmetic plus letter-number plus digit span tests.
i Includes symbol search plus digit symbol tests.
j T-scores have a mean (SD) of 50 (10) and are T-scores.
39 serious adverse events related to cluded nervous system disorders verse events were resolved in 99% of
the surgical procedure, 26 also were (n=15), psychiatric disorders (n=11), cases by 6 months. Although the seri-
attributed to other concurrent causes. device-related complications (such as ous adverse event rate was higher for
Two deep brain stimulation patients lead migration and defective lead wire; deep brain stimulation patients than for
died; 1 death was secondary to cere- n=8), cardiac disorders (n=4), other in- best medical therapy patients, there was
bral hemorrhage that occurred 24 fections (n = 2), and other events no difference in the serious adverse
hours after lead implantation. The (n = 20). Six patients experienced falls event rate between older (26%) and
second death was due to lung cancer; resulting in injury. younger (25%) patients. Also, there
however, the patient withdrew par- Fifteen best medical therapy pa- were no differences in types of serious
ticipation prior to deep brain stimula- tients (11%) experienced 19 serious ad- adverse events experienced by age (re-
tion implantation. verse events. Events included nervous sults not shown).
The most common serious adverse system (n=3), psychiatric (n=2), and
event was surgical site infection. Twelve cardiac (n = 2) disorders; falls (n = 2); COMMENT
patients had 16 infections related to the other infections (n=2); and other events This large randomized controlled trial
surgical procedure or device. These in- (n = 8). demonstrated that deep brain stimula-
fections resulted in antibiotic therapy The overall incidence risk of expe- tion is superior to best medical therapy
and removal of the leads, neurostimu- riencing a serious adverse event was 3.8 in improving motor function and qual-
lator, or both. By the 6-month follow- times higher (95% CI, 2.3-6.3) in deep ity of life in PD patients with motor
up, some patients received implants brain stimulation patients than in best complications and inadequate symp-
again. Other serious adverse events in- medical therapy patients. Serious ad- tom control with medication, even
70 JAMA, January 7, 2009—Vol 301, No. 1 (Reprinted) ©2009 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
when older patients were included in undergo deep brain stimulation experi- ment. However, adverse event rates
the study. Most successful recent clini- ence improvements in quality of life.23-25 were much higher in the deep brain
cal trials of adjunctive medications for There were small but statistically sig- stimulation group than in the best
patients with PD and motor fluctua- nificant group differences in change in medical therapy group. Many adverse
tions report an improvement of on time cognitive test performance. While the events experienced by patients in the
of only 1 to 2 hours.20-22 In the current best medical therapy group had slight im- deep brain stimulation group oc-
study, patients receiving deep brain provements on several scales, deep brain curred during the first 3 months fol-
stimulation reported an average in- stimulation was associated with small lowing surgery. Some reflect the typi-
crease of 4.6 hours per day in on time, decrements in cognitive test perfor- cal consequences of surgery performed
accompanied by reductions in on time mance. Previous studies of deep brain in older patients with comorbidities;
with troubling dyskinesia and off time. stimulation that included neuropsycho- others represent transient adverse ef-
Blinded UPDRS motor assessments, a logical batteries have shown reductions fects associated with adjustments of
unique feature of this study, con- in verbal associative fluency and other stimulation and medication therapies
firmed self-reported improvements in tasks following deep brain stimulation, during the postimplant period.
motor functioning, which improved by interpreted by some as indications of ex- The most common neurobehav-
29% on average. This is comparable ecutive dysfunction.26,27 The present re- ioral adverse events included depres-
with improvements reported in sev- search reveals an overall similar pattern sion, confusional state, and anxiety,
eral previous nonrandomized and un- but also suggests that in the present co- which were all higher in patients in the
blinded studies of globus pallidus and hort, several domains of executive func- deep brain stimulation group. A re-
subthalamic nucleus deep brain stimu- tioning remain unaffected, whereas cent meta-analysis 28 of psychiatric
lation.2 In contrast, most patients re- working memory and visuomotor speed events following deep brain stimula-
ceiving best medical therapy did not reveal small deep brain stimulation ef- tion reported that confusion ac-
show improvement in motor function- fects. The specific factors contributing to counted for 4% and depression for 2%
ing after 6 months of management by these declines in information process- of adverse events reported, which is
movement disorder neurologists. ing speed and working memory and their comparable with our findings. An-
Improved motor functioning experi- clinical significance remain to be ex- other review29 of behavioral changes fol-
enced by patients receiving deep brain plored. lowing subthalamic nucleus deep brain
stimulation was accompanied by signifi- The benefits of improved on time and stimulation found that 41% of pa-
cant improvements in quality of life. This quality of life need to be weighed against tients experienced cognitive problems
finding is comparable with uncon- the risk of complications related to sur- and 8% experienced depression, indi-
trolled studies of deep brain stimula- gery. The number of adverse events was cating that behavioral issues can be a
tion of both subthalamic nucleus and glo- high in both groups, which was ex- concern for treatment with deep brain
bus pallidus, showing that patients who pected due to the method of ascertain- stimulation.
Table 4. Most Frequent Moderate and Severe Adverse Events for Best Medical Therapy and Deep Brain Stimulation Groups a
Adverse Events From Randomization to 3 Months Adverse Events From 4 to 6 Months
Best Medical Deep Brain Best Medical Deep Brain
Therapy Stimulation Therapy Stimulation
No. of No. of No. of No. of P No. of No. of No. of No. of P
Adverse Events b Patients Events Patients Events Value c Patients Events Patients Events Value c
Fall 6 6 16 17 .02 5 5 14 14 .03
Gait disturbance 9 9 15 16 .14 4 4 10 10 .10
Dyskinesia 11 11 9 9 ⬎.99 5 5 12 12 .08
Motor dysfunction 9 9 13 13 .27 6 6 3 3 .51
Balance disorder 6 6 12 13 .14 4 4 6 6 .53
Pain 3 3 10 13 .04 3 3 8 9 .12
Speech disorder 2 2 12 13 .004 3 3 7 7 .20
Dystonia 5 5 10 11 .18 1 1 8 8 .02
Headache 1 1 20 22 ⬍.001 0 0 1 1 .48
Bradykinesia 4 4 12 13 .04 3 3 4 4 .71
Confusional state 1 1 13 15 ⬍.001 3 3 3 3 ⬎.99
Freezing phenomena 6 6 5 5 ⬎.99 3 3 7 7 .20
a Adverse events exclude those that were rated as mild and those with low total frequency (⬍10 events); also note that adverse events include severe adverse events by definition.
b The total number of moderate and severe adverse events were 236 for the best medical therapy group and 659 for the deep brain stimulation group.
c Based on the number of unique patients.
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 71
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
There also were more falls in the deep sion of an older cohort of patients and cognitive functioning following the con-
brain stimulation group, often result- the fact that the trial was rigorously clusion of phase 2 of this study will shed
ing in injuries (eg, fractures, disloca- monitored for identification of all light on these issues. Caution should
tions, head trauma) requiring surgery adverse events. be exercised, however, against over-
or another intervention. Falls have not A limitation of this study is that the stating or understating the risks of deep
been reported specifically in most stud- subthalamic nucleus and globus palli- brain stimulation for patients with PD.
ies of deep brain stimulation. It is not dus cases are pooled into a single deep Physicians must continue to weigh the
clear whether deep brain stimulation in- brain stimulation group. When the potential short-term and long-term risks
creases fall risk directly or whether pa- study was planned, it was thought that with the benefits of deep brain stimu-
tients are at higher risk secondary to the differences at 6 months between lation in each patient.
their improved function and greater ac- those treated with subthalamic nucleus Author Affiliations: Center for Management of Com-
tivity level. These results suggest that and those treated with globus pallidus plex Chronic Care (Dr Weaver) and Cooperative Stud-
ies Coordinating Center (Drs Hur and Reda), Hines VA
clinicians treating movement disor- would be small. Also, the second phase Hospital, Hines, Illinois; Department of Neurology,
ders should review fall-risk precau- of the study comparing surgical tar- Northwestern University, Chicago, Illinois (Dr Weaver);
Department of Neurosurgery, University of Ne-
tions with their patients prior to ad- gets remains blinded until completion braska, Omaha (Dr Follett); Department of Neurol-
ministering deep brain stimulation. of the study, which is anticipated to oc- ogy, University of Pennsylvania Health System, Phila-
Serious adverse events resulting in cur in April 2009. In a previous meta- delphia (Drs Stern, Duda, and Horn); Philadelphia VA
Medical Center, Philadelphia, Pennsylvania (Drs Stern
permanent sequelae were uncommon. analysis,2 as well as a small random- and Duda); VA Cooperative Studies Program, Clini-
One death was due to surgical compli- ized trial comparing subthalamic cal Research Pharmacy, Albuquerque, New Mexico (Dr
Harris); San Francisco VA Medical Center, San Fran-
cations following deep brain stimula- nucleus with globus pallidus,30 there cisco, California (Drs Marks and Rothlind); Depart-
tion implantation. A second patient were no significant differences in mo- ments of Neurology (Dr Marks) and Psychiatry (Dr
Rothlind), University of California, San Francisco; De-
withdrew prior to deep brain stimula- tor outcomes by deep brain stimula- partment of Neurosurgery, University of Michigan
tion and died due to lung cancer. An- tion target, supporting our presump- Medical Center, Ann Arbor (Dr Sagher); National In-
stitute of Neurological Disorders and Stroke, Rock-
other patient required permanent in- tion of little or no difference by deep ville, Maryland (Drs Moy and Heemskerk); Depart-
stitutionalization approximately 5 brain stimulation target group. Non- ment of Neurology, University of Kansas Medical
months after deep brain stimulation due randomized trials have identified more Center, Kansas City (Dr Pahwa); Portland VA Medi-
cal Center, Portland, Oregon (Drs Burchiel and
to impaired activities of daily living and cognitive adverse events in patients who Hogarth); Departments of Neurosurgery (Dr Bur-
occasional delusions or hallucina- have undergone subthalamic nucleus chiel) and Neurology (Dr Hogarth), Oregon Health and
Science University, Portland; Michael E. DeBakey VA
tions. Implant site infections occurred than globus pallidus deep brain stimu- Medical Center, Houston, Texas (Dr Lai); Depart-
in approximately 10% of patients re- lation.31 Phase 2 of this study, when ment of Neurology, Baylor College of Medicine, Hous-
ton, Texas (Dr Lai); Richmond VA Medical Center, Rich-
ceiving deep brain stimulation. completed, will provide an in-depth as- mond, Virginia (Dr Holloway); Department of
These findings support and extend sessment of a wide variety of out- Neurosurgery, Virginia Commonwealth University,
those of the study by Deuschl et al,7 comes based on surgical target. Richmond (Dr Holloway); Puget Sound Health Care
System, Seattle, Washington (Dr Samii); West Los An-
which involved 156 pairs of PD geles VA Medical Center, Los Angeles, California (Dr
patients randomized to subthalamic CONCLUSIONS Bronstein); Department of Neurosurgery, University
of Iowa Health Care, Iowa City (Ms Stoner); and De-
nucleus deep brain stimulation or In this randomized controlled trial, deep partment of Veterans Affairs, Cooperative Studies Pro-
medical therapy. The Parkinson Dis- brain stimulation was more effective gram Central Office, VA Office of Research and De-
velopment, Washington, DC (Dr Huang).
ease Questionnaire 39, UPDRS, and than best medical therapy in alleviat- Author Contributions: Dr Hur had full access to all of
motor diary findings were similar in ing disability in patients with moder- the data in the study and takes responsibility for the in-
both studies. Specifically, Deuschl et ate to severe PD with motor complica- tegrity of the data and the accuracy of the data analysis.
Study concept and design: Weaver, Follett, Stern, Hur,
al7 reported a 4.4-hour-per-day aver- tions responsive to levodopa and no Marks Jr, Sagher, Reda, Bronstein, Heemskerk.
age gain in on time and in this study, significant cognitive impairment. The Acquisition of data: Stern, Hur, Harris, Marks Jr,
Rothlind, Burchiel, Hogarth, Lai, Duda, Holloway, Samii,
we report a 4.6-hour-per-day average extent of benefit was similar for younger Horn, Bronstein, Stoner.
gain for patients in the deep brain and older patients, although adverse Analysis and interpretation of data: Weaver, Follett,
Stern, Hur, Harris, Marks Jr, Rothlind, Sagher, Reda,
stimulation group. Our results were events were higher in older patients. Moy, Pahwa, Hogarth, Lai, Samii, Horn, Huang.
comparable, even with the inclusion The clinical significance of the ad- Drafting of the manuscript: Weaver, Follett, Hur, Harris,
Marks Jr, Rothlind.
of a significant number of older verse events and minor neurocogni- Critical revision of the manuscript for important in-
patients. A larger proportion of tive changes observed in patients in the tellectual content: Follett, Stern, Hur, Harris, Marks
patients in our study experienced seri- deep brain stimulation group and, more Jr, Sagher, Reda, Moy, Pahwa, Burchiel, Hogarth, Lai,
Duda, Holloway, Samii, Horn, Bronstein, Stoner,
ous adverse events than in the study importantly, whether patients who un- Heemskerk, Huang.
by Deuschl et al7 (25% vs 8%); there dergo deep brain stimulation view im- Statistical analysis: Hur, Reda.
Obtained funding: Weaver, Follett, Stern, Reda,
were 2 deaths in this trial and 4 in the provement in motor function and qual- Heemskerk, Huang.
study by Deuschl et al. The greater ity of life as outweighing adverse events, Administrative, technical, or material support: Follett,
Stern, Harris, Moy, Burchiel, Hogarth, Lai, Duda,
number of serious adverse events in remain to be explored. More detailed Holloway, Samii, Horn, Bronstein, Stoner, Heemskerk,
our trial is likely attributable to inclu- analyses of adverse events and neuro- Huang.
72 JAMA, January 7, 2009—Vol 301, No. 1 (Reprinted) ©2009 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
TREATMENT FOR ADVANCED PARKINSON DISEASE
Study supervision: Weaver, Follett, Stern, Harris, Marks becca Warker, APRN, Heidi Watson, BSN, Pamela Will- for Evaluating Surgery in Parkinson’s Disease: Third
Jr, Rothlind, Sagher, Hogarth, Lai, Stoner, Heemskerk, son, PhD. Neurologists: Mark Baron, MD, Matthew Symposium on Parkinson’s Disease. Edinburgh, Scot-
Huang. Brodsky, MD, Jeff Bronstein, MD, PhD, Vincent Cala- land: Gillingham & Donaldson; 1969.
Financial Disclosures: Dr Marks Jr reported serving brese, MD, Gordon Campbell, ANP, Amy Colcher, MD, 14. Peto V, Jenkinson C, Fitzpatrick R. PDQ-39: a re-
as a faculty member for educational programs spon- John Duda, MD, Emad Faraq, MD, Eva Henry, MD, view of the development, validation and application
sored by Medtronic and also as a consultant to Penelope Hogarth, MD, Jyh-Gong Hou, MD, PhD, Gail of a Parkinson’s disease quality of life questionnaire
Medtronic, the manufacturer of the deep brain stimu- Kang, MD, Galit Kleiner-Fisman, MD, Jeff Kraakevik, and its associated measures. J Neurol. 1998;245
lation device. Dr Pahwa reported being a consultant MD, Stacy Horn, DO, Eugene C. Lai, MD, PhD, Wil- (suppl 1):S10-S14.
and speaker for Medtronic and a consultant for Ad- liam J. Marks Jr, MD, John Nutt, MD, Jill Ostrem, MD, 15. Hauser RA, Deckers F, Lehert P. Parkinson’s dis-
vanced Neuromodulation Systems. Dr Duda re- Ali Samii, MD, Aliya Sarwar, MD, Indu Subramanian, ease home diary: further validation and implications
ported serving as a board member for Boehringer/ MD, Zeba Vanek, MD. Neurosurgeons: Gordon Bal- for clinical trials. Mov Disord. 2004;19(12):1409-
Ingelheim. Dr Holloway reported serving as a teaching tuch, MD, PhD, Kim Burchiel, MD, Antonio DeSalles, 1413.
consultant for Medtronic, the manufacturer of the deep MD, PhD, Jorge Eller, MD, Kathryn Holloway, MD, Paul 16. Goetz CG, Stebbins GT, Blasucci LM, Grobman
brain stimulation device, instructing other neurosur- Larson, MD, Richard Simpson, MD, Philip Starr, MD, MS. Efficacy of a patient-training videotape on mo-
geons on the technique of deep brain stimulation im- PhD. Neuropsychologists: William Carne, PhD, Tom Erik- tor fluctuations for on-off diaries in Parkinson’s disease.
plantation. No other authors reported financial dis- son, PhD, Jurg Jaggi, PhD, Jeffrey Kreutzer, PhD, Mario Mov Disord. 1997;12(6):1039-1041.
closures. Mendez, MD, PhD, Paul Moberg, PhD, John Ragland, 17. Pahwa R, Wilkinson SB, Overman J, Lyons KE. Bi-
Funding/Support: The Cooperative Studies Program PhD, Johannes Rothlind, PhD, Ronald Seel, PhD, Eliza- lateral subthalamic stimulation in patients with Par-
of the Department of Veterans Affairs Office of Re- beth Soety, PhD, Daniel Storzbach, PhD, Alexander kinson disease: long-term follow up. J Neurosurg. 2003;
search and Development, the National Institute of Neu- Troster, PhD, Michele York, PhD. 99(1):71-77.
rological Disorders and Stroke, and Medtronic Neu- Disclaimer: The views expressed in this article are those 18. Cohen J. Statistical Power Analysis for the Be-
romodulation provided financial support for this study. of the authors and do not necessarily reflect the po- havioral Sciences. 2nd ed. Hillsdale, NJ: Erlbaum; 1988.
Role of the Sponsors: The Department of Veterans sition or policy of the Department of Veterans Affairs 19. Schrag A, Sampaio C, Counsell N, Poewe W. Mini-
Affairs Cooperative Studies Program and the Na- or the National Institute of Neurological Disorders and mal clinically important change on the United Parkin-
tional Institute of Neurological Disorders and Stroke Stroke. son’s Disease Rating Scale. Mov Disord. 2006;
contributed to the study design. The sponsors were Additional Contributions: We thank the Veterans Ad- 21(8):1200-1207.
not involved in the conduct, collection, manage- ministration Parkinson’s Disease Research, Education 20. Parkinson Study Group. DATATOP: a multi-
ment, analysis, and/or interpretation of the study re- and Clinical Centers in Portland/Seattle (Northwest), center controlled clinical trial in early Parkinson’s
sults and preparation, review, or approval of the manu- San Francisco, Los Angeles (Southwest), Houston, Rich- disease. Arch Neurol. 1989;46(10):1052-1060.
script. Medtronic provided financial support for mond (Southeast), and Philadelphia. 21. Parkinson’s Study Group. Entacapone improves
monitoring and collecting data at 3 years of patient motor fluctuations in levodopa-treated Parkinson’s dis-
follow-up. REFERENCES ease patients. Ann Neurol. 1997;42(5):747-755.
Past and Present Members of the CSP 468 Study Group: 22. Parkinson’s Study Group. A randomized placebo-
Kenneth Follett, MD, PhD, Matthew Stern, MD, Frances 1. Rodriguez RL, Fernandez HH, Haq I, Okun MS. controlled trial of rasagiline in levodopa-treated pa-
Weaver, PhD (chairpersons); Dolores Ippolito, MPH, Ga- Pearls in patient selection for deep brain stimulation. tients with Parkinson disease and motor fluctuations:
tana Stoner, RN, CCRC (chairpersons office). Hines VA Neurologist. 2007;13(5):253-260. the PRESTO study. Arch Neurol. 2005;62(2):241-
Cooperative Studies Program Coordinating Center: 2. Weaver F, Follett K, Hur K, Ippolito D, Stern M. 248.
Tammy Barnett, MA, Ken Bukowski, BS, Rosemarie Deep brain stimulation in Parkinson disease: a metaan- 23. Straits-Tröster K, Fields JA, Wilkinson SB, et al.
DeNicolo, Kwan Hur, PhD, Joyce Jimenez, Ping Luo, PhD, alysis of patient outcomes. J Neurosurg. 2005; Health-related quality of life in Parkinson’s disease af-
Jan Motyka, BS, Domenic Reda, PhD, Theresa Simon, 103(6):956-967. ter pallidotomy and deep brain stimulation. Brain Cogn.
RN, BS, Bharat Thakkar, MS, Robert Woolson, JD, MS. 3. Lang AE, Houeto JL, Krack P, et al. Deep brain stimu- 2000;42(3):399-416.
Pharmacy Coordinating Center: Carol Fye, RPh, MS, lation: preoperative issues. Mov Disord. 2006; 24. Just H, Ostergaard K. Health-related quality of life
CCRP, William Gagne, Crystal Harris, PharmD. Study 21(suppl 14):S171-S196. in patients with advanced Parkinson’s disease treated
Monitors: Julia Buckelew, CCRA, Carol Fye, RPh, MS, 4. Follett KA. The surgical treatment of Parkinson’s with deep brain stimulation of the subthalamic nuclei.
CCRP, Marilyn Garin, Sharon Matzek, CCRA, Donna disease. Annu Rev Med. 2000;51:135-147. Mov Disord. 2002;17(3):539-545.
Smith, CCRA. National Institute of Neurological Dis- 5. Temel Y, Blokland A, Steinbusch HW, 25. Limousin P, Martinez-Torres I. Deep brain stimu-
orders and Stroke: Jill Heemskerk, PhD, Claudia Moy, Visser-Vandewalle V. The functional role of the sub- lation for Parkinson’s disease. Neurotherapeutics. 2008;
PhD, Paul Sheehy, PhD. MAVERIC: Louis Fiore, MD, thalamic nucleus in cognitive and limbic circuits. Prog 5(2):309-319.
Robert Hall, MS. Health Economist: Kevin Stroupe, PhD. Neurobiol. 2005;76(6):393-413. 26. Witt K, Daniels C, Reiff J, et al. Neuropsychologi-
Executive Committee: Kim Burchiel, MD, Kenneth Fol- 6. Krack P, Batir A, Van Blercom N, et al. Five-year cal and psychiatric changes after deep brain stimula-
lett, MD, PhD, Carol Fye, RPh, MS, CCRP, Crystal Har- follow-up of bilateral stimulation of the subthalamic tion for Parkinson’s disease: a randomised, multicen-
ris, PharmD, Jill Heemskerk, PhD, Kwan Hur, PhD, Wil- nucleus in advanced Parkinson’s disease. N Engl J Med. tre trial. Lancet Neurol. 2008;7(7):605-614.
liam Koller, MD, PhD, William J. Marks Jr, MD, Claudia 2003;349(20):1925-1934. 27. Alegret M, Junque C, Valldeoriola F, et al. Ef-
Moy, PhD, Rajesh Pahwa, MD, Domenic Reda, PhD, 7. Deuschl G, Schade-Brittinger C, Krack P, et al; Ger- fects of bilateral subthalamic stimulation on cogni-
Johannes Rothlind, PhD, Oren Sagher, MD, Paul Sheehy, man Parkinson Study Group, Neurostimulation Section. tive function in Parkinson disease. Arch Neurol. 2001;
PhD, Matthew Stern, MD, Frances Weaver, PhD. Data A randomized trial of deep-brain stimulation for Parkin- 58(8):1223-1227.
and Safety Monitoring Board: Roy Bakay, MD (chair- son’s disease. N Engl J Med. 2006;355(9):896-908. 28. Appleby BS, Duggan PS, Regenberg A, Rabins
man), Rick Chappell, PhD, Robert Hart, MD, Robert Hol- 8. Hoehn MM, Yahr MD. Parkinsonism: onset, pro- PV. Psychiatric and neuropsychiatric adverse events
loway Jr, MD, PhD, George McCabe, PhD, Margaret gression and mortality. Neurology. 1967;17(5): associated with deep brain stimulation: a meta-
Schenkman, PhD, Jamal Taha, MD. Site Investigators: 427-442. analysis of ten years’ experience. Mov Disord. 2007;
Jeff Bronstein, MD, PhD, John Duda, MD, Penelope 9. Mattis S. Dementia Rating Scale: Professional 22(12):1722-1728.
Hogarth, MD, Kathryn Holloway, MD, Stacy Horn, DO, Manual. Odessa, FL: Psychological Assessment Re- 29. Temel Y, Kessels A, Tan S, Topdag A, Boon P,
Eugene C. Lai, MD, PhD, William J. Marks Jr, MD, Ali sources Inc; 1973. Visser-Vandewalle V. Behavioural changes after bi-
Samii, MD. Site Coordinators: Farah Atassi, MD, MPH, 10. Langston JW, Widner H, Goetz CG, et al. Core lateral subthalamic stimulation in advanced Parkin-
Cecilia Bello, BSN, Lisette Bunting-Perry, RN, MSN, assessment program for intracerebral transplanta- son disease: a systematic review. Parkinsonism Relat
CCRC, Tina Conn, BSN, Alice Cugley, RN, NP, Nanette tions (CAPIT). Mov Disord. 1992;7(1):2-13. Disord. 2006;12(5):265-272.
Eubank, RN, CCRP, Linda Fincher, RN, BSN, Romay 11. Folstein MF, Folstein SE, McHugh PR. ”Mini- 30. Burchiel KJ, Anderson VC, Favre J, Hammerstad
Franks, BSN, Tammy Harris, MSN, RN, GNP, Mariann mental state”: a practical method for grading the cog- JP. Comparison of pallidal and subthalamic nucleus
Haselman, RN, Susan Heath, RN, MS, Miriam Hirsch, nitive state of patients for the clinician. J Psychiatr Res. deep brain stimulation for advanced Parkinson’s dis-
MS, RN, Virginia Janovsky, RN, MN, MS, Elaine Lanier, 1975;12(3):189-198. ease: results of a randomized, blinded pilot study.
RN, MS, Mary Lloyd, RN, Susan Loehner, BSN, MBA, 12. Fahn S, Elton RL; Members of the UPDRS Devel- Neurosurgery. 1999;45(6):1375-1382.
Susan O’Connor, RN, Ligaya Ordonez, BSN, Heather opment Committee. Unified Parkinson’s Disease Rat- 31. Hariz MI, Rehncrona S, Quinn NP, Speelman JD,
Maccarone, RN, BSN, Kelli Massey-Makhoul, RN, Mary ing Scale. In: Fahn S, Marsden CD, Goldstein M, eds. Wensing C; Multicentre Advanced Parkinson’s Dis-
Matthews, RN, Elizabeth Meyn, BSN, Keiko Mimura, Recent Developments in Parkinson’s Disease. Vol 2. ease Deep Brain Stimulation Group. Multicenter study
RN, MSN, GNP, Wes Morrow, MS, MMSc, PAC, Tammy Florham Park, NJ: Macmillan Health Care Informa- on deep brain stimulation in Parkinson’s disease: an
Searles, RN, Jamye Valotta, BSN, Usha Vasthare, PhD, tion; 1987:153-164. independent assessment of reported adverse events
Monica Volz, RN, MS, Constance Ward, RN, MSN, Re- 13. Schwab RS, England AC. Projection Technique at 4 years. Mov Disord. 2008;23(3):416-421.
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 73
Downloaded From: http://jama.jamanetwork.com/ by a University of Delaware User on 06/19/2012
You might also like
- The End of Mental Illness: How Neuroscience Is Transforming Psychiatry and Helping Prevent or Reverse Mood and Anxiety Disorders, ADHD, Addictions, PTSD, Psychosis, Personality Disorders, and MoreFrom EverandThe End of Mental Illness: How Neuroscience Is Transforming Psychiatry and Helping Prevent or Reverse Mood and Anxiety Disorders, ADHD, Addictions, PTSD, Psychosis, Personality Disorders, and MoreRating: 4.5 out of 5 stars4.5/5 (12)
- Neil Mcdonald - The King's Indian Attack Move by Move PDFDocument353 pagesNeil Mcdonald - The King's Indian Attack Move by Move PDFantonius-raducu91% (43)
- Étude Du Centre de Traitement Des Lésions Cérébrales de L'université de DalhousieDocument41 pagesÉtude Du Centre de Traitement Des Lésions Cérébrales de L'université de DalhousieRadio-Canada100% (2)
- 00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenDocument13 pages00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenYo MeNo ratings yet
- Electronic Media. 2nd Edition PDFDocument319 pagesElectronic Media. 2nd Edition PDFAwobamise Ayodeji Olalekan100% (1)
- Bilateral Deep Brain Stimulation Vs Best Medical Therapy For Patients With Advanced Parkinson DiseaseDocument11 pagesBilateral Deep Brain Stimulation Vs Best Medical Therapy For Patients With Advanced Parkinson DiseasemasitaluthfivpNo ratings yet
- Jurnal 1Document10 pagesJurnal 1Hafizh Rafi RabbaniNo ratings yet
- JAMA Psychiatry - : Original InvestigationDocument10 pagesJAMA Psychiatry - : Original InvestigationMesianissimoNo ratings yet
- 1 s2.0 S0890856714004079 MainDocument10 pages1 s2.0 S0890856714004079 MainPar DoNo ratings yet
- 1 s2.0 S1064748113001644 PDFDocument25 pages1 s2.0 S1064748113001644 PDFUSM San IgnacioNo ratings yet
- Six-Month Neuropsychological Outcome of Medical Intensive Care Unit PatientsDocument9 pagesSix-Month Neuropsychological Outcome of Medical Intensive Care Unit PatientsYamile Cetina CaheroNo ratings yet
- Antipsychotics and The BrainDocument5 pagesAntipsychotics and The BrainsyamimisdNo ratings yet
- Fisher 2010Document10 pagesFisher 2010Estereotaxia BrasilNo ratings yet
- Aplicaciones Clínicas de La DbsDocument10 pagesAplicaciones Clínicas de La DbsTARNo ratings yet
- 007Document3 pages007Ed RibeiroNo ratings yet
- JCPDocument11 pagesJCPChangNo ratings yet
- 1er ArticuloDocument7 pages1er ArticuloAlexRázuriNo ratings yet
- Gray 2014Document10 pagesGray 2014Nada MachichNo ratings yet
- Psico CirugiaDocument24 pagesPsico CirugiaJuliana MartinezNo ratings yet
- Comparison of Hypothermia and Normothermia After Severe Traumatic Brain Injury in Children (Cool Kids) : A Phase 3, Randomised Controlled TrialDocument8 pagesComparison of Hypothermia and Normothermia After Severe Traumatic Brain Injury in Children (Cool Kids) : A Phase 3, Randomised Controlled TrialRupert AsesorNo ratings yet
- Rapid Decrease in Depressive Symptoms With An N-methyl-Daspartate Antagonist in ECT-Resistant Major DepressionDocument10 pagesRapid Decrease in Depressive Symptoms With An N-methyl-Daspartate Antagonist in ECT-Resistant Major DepressionCeyda AcarNo ratings yet
- 435 Full PDFDocument8 pages435 Full PDFRizky Qurrota AinyNo ratings yet
- Research Article: Neuroprotective Effects of Cistanches Herba Therapy On Patients With Moderate Alzheimer's DiseaseDocument13 pagesResearch Article: Neuroprotective Effects of Cistanches Herba Therapy On Patients With Moderate Alzheimer's DiseaseVeronica Yosita AnandaNo ratings yet
- Effects of Physical Therapy On Mental Function in Patients With StrokeDocument6 pagesEffects of Physical Therapy On Mental Function in Patients With StrokeTeuku FadhliNo ratings yet
- New England Journal Medicine: The ofDocument13 pagesNew England Journal Medicine: The ofTha Vila Le ColloNo ratings yet
- Panic Disorder Research PaperDocument5 pagesPanic Disorder Research Paperapi-640806239No ratings yet
- Clinical Hypnosis in The Treatment of Post-Menopausal Hot Flashes: A Randomized Controlled TrialDocument16 pagesClinical Hypnosis in The Treatment of Post-Menopausal Hot Flashes: A Randomized Controlled TrialEdson ToshioNo ratings yet
- Predictors of Poor Treatment Response ToDocument13 pagesPredictors of Poor Treatment Response ToMaite Novo del valleNo ratings yet
- Bilingualism As A Protection Against The Onset of Symptoms of DementiaDocument6 pagesBilingualism As A Protection Against The Onset of Symptoms of DementiaSonier KaeceipzNo ratings yet
- Bartlett 2020Document9 pagesBartlett 2020Erick SolisNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: Backgroundmonica ortizNo ratings yet
- Yoga On Our Minds: A Systematic Review of Yoga For Neuropsychiatric DisordersDocument16 pagesYoga On Our Minds: A Systematic Review of Yoga For Neuropsychiatric DisordersDaniela DiazNo ratings yet
- Dopamine Antagonists in ICU DeliriumDocument2 pagesDopamine Antagonists in ICU DeliriumRodrigoSachiFreitasNo ratings yet
- From Pro-Inflammatory Molecules To The Brain's Resting-State Connectivity The Future of Clinical Diagnosis of DepressionDocument36 pagesFrom Pro-Inflammatory Molecules To The Brain's Resting-State Connectivity The Future of Clinical Diagnosis of DepressiondgavrileNo ratings yet
- Neuroimage: Clinical: SciencedirectDocument9 pagesNeuroimage: Clinical: SciencedirectMoumi PanditNo ratings yet
- Medi 100 E23469Document7 pagesMedi 100 E23469Belva EdinaNo ratings yet
- Comp Il CationDocument8 pagesComp Il CationWahyu Permata LisaNo ratings yet
- Benefits of Cognitive-Motor Intervention in MCI and Mild To Moderate Alzheimer DiseaseDocument6 pagesBenefits of Cognitive-Motor Intervention in MCI and Mild To Moderate Alzheimer DiseaseLaura Alvarez AbenzaNo ratings yet
- Psychiatric Outcomes After Temporal Lobe Surgery in Patients With Temporal Lobe Epilepsy and Comorbid Psychiatric IllnessDocument8 pagesPsychiatric Outcomes After Temporal Lobe Surgery in Patients With Temporal Lobe Epilepsy and Comorbid Psychiatric IllnessFrancisco Javier Fierro RestrepoNo ratings yet
- Scalp Acupuncture Treatment Protocol For Anxiety Disorders: A Case ReportDocument6 pagesScalp Acupuncture Treatment Protocol For Anxiety Disorders: A Case ReportTanuku NetNo ratings yet
- ENERGY PSYCH THERAPY EVIDENCEDocument19 pagesENERGY PSYCH THERAPY EVIDENCElandburender100% (1)
- Depression and TelepsychiatryDocument6 pagesDepression and TelepsychiatryMaria Von ShaftNo ratings yet
- Cognitive Effects of Antipsychotic Drugs in First-Episode Schizophrenia and Schizophreniform Disorder: A Randomized, Open-Label Clinical Trial (EUFEST)Document8 pagesCognitive Effects of Antipsychotic Drugs in First-Episode Schizophrenia and Schizophreniform Disorder: A Randomized, Open-Label Clinical Trial (EUFEST)yeremias setyawanNo ratings yet
- A Pilot, Double-Blind, Placebo-Controlled Trial of Pregabalin (Lyrica) in The Treatment of Essential TremorDocument4 pagesA Pilot, Double-Blind, Placebo-Controlled Trial of Pregabalin (Lyrica) in The Treatment of Essential TremorPaul AsturbiarisNo ratings yet
- Bronfort2001 2Document10 pagesBronfort2001 2Shaun TylerNo ratings yet
- Use of Human Embryonic Stem Cells in The Treatment of Parkinson's Disease: A Case ReportDocument4 pagesUse of Human Embryonic Stem Cells in The Treatment of Parkinson's Disease: A Case Reportเพียงแค่ แอนโทนี่No ratings yet
- Quetiapine or Haloperidol As Monotherapy For Bipolar Mania A 12week Doubleblind Randomised Placebo Controlled Trial - Europ Neuropsych 2005Document13 pagesQuetiapine or Haloperidol As Monotherapy For Bipolar Mania A 12week Doubleblind Randomised Placebo Controlled Trial - Europ Neuropsych 2005Pedro GargoloffNo ratings yet
- Jurnal SkizoafektifDocument7 pagesJurnal SkizoafektifkhairinanurulNo ratings yet
- Current Trends Stroke Rehabilitation JohanssonDocument13 pagesCurrent Trends Stroke Rehabilitation Johanssonsidney drecotteNo ratings yet
- HHS Public Access: Double-Blind, Sham-Controlled, Pilot Study of Trigeminal Nerve Stimulation For ADHDDocument18 pagesHHS Public Access: Double-Blind, Sham-Controlled, Pilot Study of Trigeminal Nerve Stimulation For ADHDDaviani Sulbaran MercadoNo ratings yet
- Effects of Patient-Directed Music Intervention On Anxiety and Sedative Exposure in Critically Ill Patients Receiving Mechanical Ventilatory SupportDocument10 pagesEffects of Patient-Directed Music Intervention On Anxiety and Sedative Exposure in Critically Ill Patients Receiving Mechanical Ventilatory SupportIndahNo ratings yet
- Benefits Exceed Risks of Newer Antidepressant Medications in Youth-Maybe NotDocument3 pagesBenefits Exceed Risks of Newer Antidepressant Medications in Youth-Maybe NotJucas EscobarNo ratings yet
- CBT More Effective Than Nutrition Counseling for Anorexia RelapseDocument5 pagesCBT More Effective Than Nutrition Counseling for Anorexia RelapseAlexa AbendanoNo ratings yet
- Sedacion EcmoDocument10 pagesSedacion EcmodavidmontoyaNo ratings yet
- 2009 Article 57Document12 pages2009 Article 57khalila humairaNo ratings yet
- tsr1501 42Document10 pagestsr1501 42cah bagusNo ratings yet
- Randomized, Placebo-Controlled Trial Pregabalin For The Treatment of Postherpetic Neuralgia: ADocument12 pagesRandomized, Placebo-Controlled Trial Pregabalin For The Treatment of Postherpetic Neuralgia: AadityaNo ratings yet
- A 7 Minute Neurocognitive Screening Battery Highly Sensitive To Alzheimer's DiseaseDocument7 pagesA 7 Minute Neurocognitive Screening Battery Highly Sensitive To Alzheimer's DiseaseRealidades InfinitasNo ratings yet
- Prone Vs Supine Positioning For Breast Cancer RadiotherapyDocument3 pagesProne Vs Supine Positioning For Breast Cancer RadiotherapyJave GajellomaNo ratings yet
- Rehabilitas Cedera OtakDocument2 pagesRehabilitas Cedera Otakbotet_2306No ratings yet
- Prediction of Psychosis in Youth at High Clinical RiskDocument20 pagesPrediction of Psychosis in Youth at High Clinical Risksaurav.das2030No ratings yet
- HHS Public AccessDocument44 pagesHHS Public Accessade sucipto17meiNo ratings yet
- Mmk265 Marketing Research Major Project (3) 1.doc 22891Document26 pagesMmk265 Marketing Research Major Project (3) 1.doc 22891dnlkabaNo ratings yet
- Perceptions of CBA Students on RH BillDocument59 pagesPerceptions of CBA Students on RH BillRichelle Lumawag50% (2)
- Malbog Sulfuric Hot SpringDocument2 pagesMalbog Sulfuric Hot SpringMark-Christopher Roi Pelobello MontemayorNo ratings yet
- Demise of Blockbuster - A Case Study ReviewDocument13 pagesDemise of Blockbuster - A Case Study ReviewYash MudliarNo ratings yet
- Putnam Voice - 11/23/11Document16 pagesPutnam Voice - 11/23/11The Lima NewsNo ratings yet
- Telecom Business Information System AbstractDocument5 pagesTelecom Business Information System AbstractTelika RamuNo ratings yet
- The Last Lie Told (Debra Webb)Document259 pagesThe Last Lie Told (Debra Webb)Fikir HailegiorgisNo ratings yet
- Music of Your LifeDocument7 pagesMusic of Your LiferietracolNo ratings yet
- Shades of White: Rendering in WatercolorDocument4 pagesShades of White: Rendering in WatercolorMichael Reardon100% (4)
- Soal PAS 2019 Kelas X IPA-IPS FIXDocument8 pagesSoal PAS 2019 Kelas X IPA-IPS FIXJessica JolieNo ratings yet
- Bahasa Inggris ASPD Dikpora Feb 2022Document15 pagesBahasa Inggris ASPD Dikpora Feb 2022WIBI CAM100% (1)
- Effect of Smell in Space PerceptionDocument8 pagesEffect of Smell in Space PerceptionApoorva KalraNo ratings yet
- L46 - Whitefield Lab Home Visit Sy No. 18/1B, K R Puram, Hobli, Sree Sai Harsha Tower, White FieldDocument4 pagesL46 - Whitefield Lab Home Visit Sy No. 18/1B, K R Puram, Hobli, Sree Sai Harsha Tower, White FieldSayantan BanerjeeNo ratings yet
- Air Asia Final ProjectDocument59 pagesAir Asia Final Projectmanaswini sharma B.G.No ratings yet
- Bachelor ThesisDocument58 pagesBachelor ThesisGabriel RazvanNo ratings yet
- Roles of ManagerDocument14 pagesRoles of ManagerNurul Ain AisyaNo ratings yet
- Nuevas Funciones Ver 5Document2 pagesNuevas Funciones Ver 5EDISSON SOLARTENo ratings yet
- Wound Healing PhasesDocument27 pagesWound Healing PhasesAnil BasnetNo ratings yet
- GSN April Meeting Explores Tasiast Gold Deposit DiscoveryDocument18 pagesGSN April Meeting Explores Tasiast Gold Deposit DiscoveryarisNo ratings yet
- 6446 Gibson PBD - HR WebDocument192 pages6446 Gibson PBD - HR WebKoke Colil Benavente100% (1)
- Negotiation Self-Assessment and Vision Report - by Umang DharDocument1 pageNegotiation Self-Assessment and Vision Report - by Umang Dharumangdhar8No ratings yet
- Project Report TemplateDocument9 pagesProject Report TemplatePriyasha BanerjeeNo ratings yet
- Activity 9 - Invitations Valentina Muñoz AriasDocument2 pagesActivity 9 - Invitations Valentina Muñoz AriasValentina Muñoz0% (1)
- Admin Upload Food Processing Industry in India August 2013Document31 pagesAdmin Upload Food Processing Industry in India August 2013pv1977No ratings yet
- Middle School English Planning GuideDocument8 pagesMiddle School English Planning GuideVictoria GutierrezNo ratings yet
- Jag MandirDocument10 pagesJag MandirMadan ChaudharyNo ratings yet
- Essay Assessment CriteriaDocument1 pageEssay Assessment CriteriaNguyen Quynh AnhNo ratings yet
- Peritonitis GuiaDocument28 pagesPeritonitis GuiaAndrea ClaudieNo ratings yet