You might also like
- Mediterranean Diet May Decrease Risk of Prostate Cancer Progression - EurekAlert! Science NewsDocument2 pagesMediterranean Diet May Decrease Risk of Prostate Cancer Progression - EurekAlert! Science Newsluis Gomez VallejoNo ratings yet
- 7Document40 pages7Felipe RichardiosNo ratings yet
- How to Prevent Prostate Problems: A Complete Guide to the Essentials of Prostate HealthFrom EverandHow to Prevent Prostate Problems: A Complete Guide to the Essentials of Prostate HealthNo ratings yet
- Bacnet® Fixed Function Thermostat: For Fan Coil/Heat Pump/Conventional SystemsDocument8 pagesBacnet® Fixed Function Thermostat: For Fan Coil/Heat Pump/Conventional Systemsamjadjaved033148100% (1)
- The Complete Guide to Prostate Cancer: Causes, Risks, Prevention, Treatments, Cures & SupportFrom EverandThe Complete Guide to Prostate Cancer: Causes, Risks, Prevention, Treatments, Cures & SupportRating: 4 out of 5 stars4/5 (1)
- There Came A Gypsy RidingDocument45 pagesThere Came A Gypsy RidingMartin McNelisNo ratings yet
- Hospital Acquired Infections-IIDocument52 pagesHospital Acquired Infections-IIFATHIMA ANo ratings yet
- Effect of Cancer On Prostates All Over The WorldDocument42 pagesEffect of Cancer On Prostates All Over The WorldRahulNo ratings yet
- Foods and NutritionDocument10 pagesFoods and NutritionShakina FyffeNo ratings yet
- Prostate Cancer Research Paper TopicsDocument4 pagesProstate Cancer Research Paper Topicsafeaoebid100% (1)
- Foods and NutritionDocument10 pagesFoods and NutritionShakina FyffeNo ratings yet
- Orgg PDFDocument12 pagesOrgg PDFVictoria KeitelNo ratings yet
- Prostate-Cancer-Screening-Info-Sheet-Final NHMRCDocument2 pagesProstate-Cancer-Screening-Info-Sheet-Final NHMRCapi-238551404No ratings yet
- Prostate Gland and Prostatic DiseaseDocument5 pagesProstate Gland and Prostatic DiseaseSalman360No ratings yet
- Prostate Cancer Research PapersDocument5 pagesProstate Cancer Research Papersyscgudvnd100% (1)
- Prostate Cancer Screening: Current Understanding and Management Adeep Thumar MD June 11, 2015Document21 pagesProstate Cancer Screening: Current Understanding and Management Adeep Thumar MD June 11, 2015NinaNo ratings yet
- Prostate Cancer Early Detection, Diagnosis, and StagingDocument39 pagesProstate Cancer Early Detection, Diagnosis, and StagingLuis AcevedoNo ratings yet
- An Introduction To: Prostate CancerDocument8 pagesAn Introduction To: Prostate Cancerkw21167No ratings yet
- Assignment of Prostate Cancer by Adel Khalil PDFDocument18 pagesAssignment of Prostate Cancer by Adel Khalil PDFعادل خليلNo ratings yet
- How To Write A Research Paper On Prostate CancerDocument4 pagesHow To Write A Research Paper On Prostate Cancertus0zaz1b1g3No ratings yet
- Early Detection and Screening of Colon Cancer Literature ReviewDocument6 pagesEarly Detection and Screening of Colon Cancer Literature Reviewapi-359121011No ratings yet
- Early Detection and Screening of Colon Cancer Literature: June 3, 2017Document5 pagesEarly Detection and Screening of Colon Cancer Literature: June 3, 2017api-359121011No ratings yet
- Pi Is 0022534713043085Document8 pagesPi Is 0022534713043085Andri Feisal NasutionNo ratings yet
- Prostate CA Poster SLUDocument2 pagesProstate CA Poster SLUkar27No ratings yet
- Prostate Cancer Treatment in India Detailed InformationDocument3 pagesProstate Cancer Treatment in India Detailed InformationinadorNo ratings yet
- Colon Cancer Screening and Prevention: Health Screening and PreventionFrom EverandColon Cancer Screening and Prevention: Health Screening and PreventionNo ratings yet
- Cancer Prevention and Screening of Older Adults: Quratulain Tariq DPTM-F15-075Document7 pagesCancer Prevention and Screening of Older Adults: Quratulain Tariq DPTM-F15-075Hafiz Shahid1No ratings yet
- Prostate Cancer Term PaperDocument4 pagesProstate Cancer Term Paperc5pdd0qg100% (1)
- Am Cancer Society 2023 - Key Statistics For Prostate Cancer Prostate CancDocument15 pagesAm Cancer Society 2023 - Key Statistics For Prostate Cancer Prostate Canctiffannie123No ratings yet
- Prostate Cancer in TripuraDocument13 pagesProstate Cancer in TripuraSnehendu BhowmikNo ratings yet
- MR - Shafi Synopsis East WestDocument22 pagesMR - Shafi Synopsis East Westshantidhama nursingNo ratings yet
- Literature Review On Cervical Cancer ScreeningDocument4 pagesLiterature Review On Cervical Cancer Screeningbqvlqjugf100% (1)
- Assignmnet LondonDocument16 pagesAssignmnet LondonRikenkumar BariaNo ratings yet
- Nourish Your Prostate, Heal Your Cancer: A comprehensive Diet Plan for Prostate Cancer Prevention, Management, Reversal and RecoveryFrom EverandNourish Your Prostate, Heal Your Cancer: A comprehensive Diet Plan for Prostate Cancer Prevention, Management, Reversal and RecoveryNo ratings yet
- Prostate Cancer THE BASICS 1 INTRODUCTION - PC The-Basics 1Document9 pagesProstate Cancer THE BASICS 1 INTRODUCTION - PC The-Basics 1arthurmathieuNo ratings yet
- Koko's Project 2 Submitted WorkDocument50 pagesKoko's Project 2 Submitted WorkNlemorusa PaschalineNo ratings yet
- Progressive Prostate Cancer, Biochemically DefinedDocument9 pagesProgressive Prostate Cancer, Biochemically DefinedchrisjoyfulNo ratings yet
- Prostate Cancer Screening: Patient Guide SeriesDocument2 pagesProstate Cancer Screening: Patient Guide SeriesThiago FeltreNo ratings yet
- MS Final Assignment Colon CancerDocument2 pagesMS Final Assignment Colon CancerI'm a PepegaNo ratings yet
- Name of Student Name of Instructor Course ID DateDocument18 pagesName of Student Name of Instructor Course ID DateNeelam shahzadiNo ratings yet
- 4152 10485 1 PBDocument6 pages4152 10485 1 PBismaili RizmiNo ratings yet
- Oup Accepted Manuscript 2018Document7 pagesOup Accepted Manuscript 2018FaidurrahmanNo ratings yet
- 168 Essentials of Gerontological Nursing: CancerDocument3 pages168 Essentials of Gerontological Nursing: CancerNeoGellinNo ratings yet
- Prostate CancerDocument8 pagesProstate CancerJohnNo ratings yet
- RRL 3Document32 pagesRRL 3louie johnNo ratings yet
- Research Paper On Colon CancerDocument7 pagesResearch Paper On Colon Cancerj1zijefifin3100% (1)
- 1 s2.0 S0889858823001077 MainDocument36 pages1 s2.0 S0889858823001077 MainNUR ADDILAH BINTI ABDUL RAHMANNo ratings yet
- Prostate Cancer Essay ThesisDocument7 pagesProstate Cancer Essay Thesisfc50ex0j100% (2)
- NURS 530 Prostate CancerDocument7 pagesNURS 530 Prostate CancerVivian OcampoNo ratings yet
- Research Paper On Cancer PreventionDocument7 pagesResearch Paper On Cancer Preventionh07d16wn100% (1)
- Brief: Ovarian Cancers: Evolving Paradigms in Research and CareDocument4 pagesBrief: Ovarian Cancers: Evolving Paradigms in Research and CareFrancesco MultinuNo ratings yet
- Prostate Cancer Screening: Are We There Yet?: March 2010 Andrew M.D. Wolf, MD University of Virginia School of MedicineDocument48 pagesProstate Cancer Screening: Are We There Yet?: March 2010 Andrew M.D. Wolf, MD University of Virginia School of Medicineibrunom3No ratings yet
- Active Surveillance For Prostate Cancer AUA Update 33 2008Document8 pagesActive Surveillance For Prostate Cancer AUA Update 33 2008moetazNo ratings yet
- 38565-Article Text-106129-3-10-20200930Document5 pages38565-Article Text-106129-3-10-20200930kirito azumaNo ratings yet
- Growing Burden of Cancer Cases in India - Overview On Causes and Types of CancerDocument7 pagesGrowing Burden of Cancer Cases in India - Overview On Causes and Types of CancerBISHAL KUMAR PATRONo ratings yet
- Prostate Cancer Screening Infosheet (1)Document2 pagesProstate Cancer Screening Infosheet (1)aravindNo ratings yet
- SennettresearchfinalpaperDocument5 pagesSennettresearchfinalpaperapi-490058714No ratings yet
- Critique Paper PayadDocument2 pagesCritique Paper PayadPhum ViphuritNo ratings yet
- Cancer. Quratulain TariqDocument18 pagesCancer. Quratulain TariqHafiz Shahid1No ratings yet
- Prostate CancerDocument19 pagesProstate CancersamwelNo ratings yet
- Thermo Fluids LabDocument23 pagesThermo Fluids LabMuket AgmasNo ratings yet
- Unit 7. The Dynamics of Ecosystems.Document12 pagesUnit 7. The Dynamics of Ecosystems.nimolesaNo ratings yet
- Dead ZoneDocument10 pagesDead ZoneariannaNo ratings yet
- Conversion Disorder in Childhood: James R. BrašićDocument8 pagesConversion Disorder in Childhood: James R. BrašićmasriffaNo ratings yet
- 可汗语法48篇(明志教育推荐) PDFDocument163 pages可汗语法48篇(明志教育推荐) PDFtellmewhour100% (2)
- Mandaya: Presented By: Cutad, Ray Dag-Uman, Ely Mae Cortes, MaikoDocument24 pagesMandaya: Presented By: Cutad, Ray Dag-Uman, Ely Mae Cortes, MaikoAPPLE MAE AGOSTONo ratings yet
- Hedging FuturesDocument39 pagesHedging Futuresapi-3833893100% (1)
- AA3 My Favorite City - Comparing Places Ejercicio FinalDocument6 pagesAA3 My Favorite City - Comparing Places Ejercicio FinalCesar Augusto Triana AyalaNo ratings yet
- Plasma MachiningDocument14 pagesPlasma MachiningMayankNo ratings yet
- Personal Development Course for Senior High StudentsDocument7 pagesPersonal Development Course for Senior High StudentsLucelle PalarisNo ratings yet
- Pds - Sunshades Instrument CoverDocument2 pagesPds - Sunshades Instrument CoverAntonio LantiguaNo ratings yet
- Include The Following in Your RTI ApplicationDocument4 pagesInclude The Following in Your RTI ApplicationRam LoharNo ratings yet
- SOP - APS - PUR - 02A - Flow Chart For PurchaseDocument2 pagesSOP - APS - PUR - 02A - Flow Chart For Purchaseprakash patelNo ratings yet
- 9-10 Manajemen Fasilitas Dan Keselamatan - PCC, HSEDocument30 pages9-10 Manajemen Fasilitas Dan Keselamatan - PCC, HSEMars Esa UnggulNo ratings yet
- SupermanDocument3 pagesSupermanGlen Michael F. WongNo ratings yet
- Microwave TubesDocument36 pagesMicrowave TubesHINDUSTAN KNOW 1No ratings yet
- Survitec Mooring Ropes BrochureDocument20 pagesSurvitec Mooring Ropes Brochurearifsarwo_wNo ratings yet
- Midterm MMMDocument2 pagesMidterm MMMasdfghjkl zxcvbnmNo ratings yet
- Mental Health Lesson on Identity, Grief, Anxiety, OCD, Schizophrenia, and Eating DisordersDocument2 pagesMental Health Lesson on Identity, Grief, Anxiety, OCD, Schizophrenia, and Eating DisordersKaya S75% (4)
- Klubermatic Lubricant DispensersDocument13 pagesKlubermatic Lubricant Dispenserstatankise100% (1)
- 2017 Aso Security TrainingDocument60 pages2017 Aso Security TrainingTanzila SiddiquiNo ratings yet
- Premium detergent market insights and Nirma case studyDocument32 pagesPremium detergent market insights and Nirma case studyBhavya ShahNo ratings yet
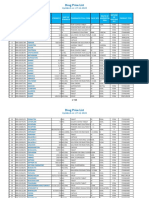
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
- Stress and Coping in Families With Deaf Children: Terri Feher-Prout University of PittsburghDocument12 pagesStress and Coping in Families With Deaf Children: Terri Feher-Prout University of PittsburghGolfiNo ratings yet
- MP Maxat Pernebayev Tanvi Singh Karthick SundararajanDocument117 pagesMP Maxat Pernebayev Tanvi Singh Karthick SundararajansadiaNo ratings yet
- Barriers To Nurse - Patient Communication in Saudi Arabia: An Integrative ReviewDocument10 pagesBarriers To Nurse - Patient Communication in Saudi Arabia: An Integrative Reviewmark3dasaNo ratings yet