You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- MOI Lesson PlanDocument4 pagesMOI Lesson PlanPreeti KumariNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Swot Analysis Arifinjr Graphic Design Firm: Executive SummaryDocument3 pagesSwot Analysis Arifinjr Graphic Design Firm: Executive SummarySri WaluyoNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Sibunag River Development Project: Industry Sector: Business Type: Location TypeDocument4 pagesSibunag River Development Project: Industry Sector: Business Type: Location Typeemma gallosNo ratings yet
- Chapter 1 and Chapter 2 PowerpointDocument14 pagesChapter 1 and Chapter 2 Powerpointapi-252892423No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- 01 AR PFMEA - TemplateDocument3 pages01 AR PFMEA - TemplateAndrew DoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Full Download Social Problems in A Diverse Society 6th Edition Diana Kendall Test BankDocument35 pagesFull Download Social Problems in A Diverse Society 6th Edition Diana Kendall Test Bankpanorarubius100% (29)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Orca Share Media1676505355563 7031773118863093717Document42 pagesOrca Share Media1676505355563 7031773118863093717Charls Aron ReyesNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Letter of RecommendationDocument1 pageLetter of RecommendationIsaac Kocherla100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Rocna and Vulcan Anchor DimensionsDocument2 pagesRocna and Vulcan Anchor DimensionsJoseph PintoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- ASW 0822 Smart Watch With Sleep Function User Guide V10Document2 pagesASW 0822 Smart Watch With Sleep Function User Guide V10Se Jin CoohNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
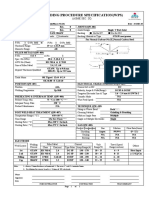
- Welding Procedure Specification (WPS) : (Asme Sec. Ix)Document1 pageWelding Procedure Specification (WPS) : (Asme Sec. Ix)Ahmed Lepda100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Inventory Management System VB6Document7 pagesInventory Management System VB6PureNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- PTE Academic - Strategies For Summarize The Written TextDocument9 pagesPTE Academic - Strategies For Summarize The Written TextPradeep PaudelNo ratings yet
- Examen EESDocument16 pagesExamen EESManu LlacsaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Case Study MtotDocument15 pagesCase Study MtotDotecho Jzo EyNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Mouthwash, PEG, Sulfate, Betaine FreeDocument2 pagesMouthwash, PEG, Sulfate, Betaine FreerekhilaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Arkansas DispensariesDocument6 pagesArkansas DispensariesAdam ByrdNo ratings yet
- Basic Electronics New - 3110016Document4 pagesBasic Electronics New - 3110016Sneha PandyaNo ratings yet
- Penilaian Kelayakan Usaha Mikro Dengan Kredit Skoring Dan Pengaruhnya Terhadap Pembiayaan Bermasalah Best Practice Lembaga Keuangan Di IndonesiaDocument12 pagesPenilaian Kelayakan Usaha Mikro Dengan Kredit Skoring Dan Pengaruhnya Terhadap Pembiayaan Bermasalah Best Practice Lembaga Keuangan Di IndonesiaRiantriaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Import FinalDocument5 pagesImport FinalRaza AliNo ratings yet
- Eatclub D5Z1X6Document1 pageEatclub D5Z1X6Devansh nayakNo ratings yet
- REC4281GDocument307 pagesREC4281GadrianahoukiNo ratings yet
- D.ANDAN PS-PROJECT WATCH ActionPlan 2018-2019Document3 pagesD.ANDAN PS-PROJECT WATCH ActionPlan 2018-2019Maria Fe PanuganNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Raymond V. Schoder, Vincent C. Horrigan, Leslie Collins Edwards - A Reading Course in Homeric Greek, Book 2-Focus Publishing (2008) PDFDocument134 pagesRaymond V. Schoder, Vincent C. Horrigan, Leslie Collins Edwards - A Reading Course in Homeric Greek, Book 2-Focus Publishing (2008) PDFSamarul MeuNo ratings yet
- Readings in Philippine History-CeDocument11 pagesReadings in Philippine History-Cedeluna.jerremieNo ratings yet
- Bài Kt 2 Biên Dịch 1-LiêmDocument10 pagesBài Kt 2 Biên Dịch 1-LiêmNguyen Loan100% (1)
- Healthcare SCM in Malaysia - Case StudyDocument10 pagesHealthcare SCM in Malaysia - Case StudyHussain Alam100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Final CV-Europass-20190916-MezakMatijević-EN (2) - Kopija PDFDocument4 pagesFinal CV-Europass-20190916-MezakMatijević-EN (2) - Kopija PDFMirela Mezak StastnyNo ratings yet
- International Journal of Transportation Science and TechnologyDocument11 pagesInternational Journal of Transportation Science and TechnologyIrvin SmithNo ratings yet
- Dynamic Strategies For Small BusinessDocument11 pagesDynamic Strategies For Small BusinessBusiness Expert Press0% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)