You might also like
- Respiratory System Anatomy and Physiology: Marianne Belleza, RNDocument18 pagesRespiratory System Anatomy and Physiology: Marianne Belleza, RNTiara GustiwiyanaNo ratings yet
- Respi & CardioDocument15 pagesRespi & CardioktNo ratings yet
- Respiratory SystemDocument46 pagesRespiratory SystemseancreedfhsNo ratings yet
- Anatomy of The Respiratory SystemDocument8 pagesAnatomy of The Respiratory Systemsuharti2365No ratings yet
- Functions of The Respiratory System: BloodDocument12 pagesFunctions of The Respiratory System: BloodSesrine BuendiaNo ratings yet
- NursingBulletin Respiratory SystemDocument35 pagesNursingBulletin Respiratory Systemseigelystic100% (3)
- NCM 113 M1 Lesson 1Document10 pagesNCM 113 M1 Lesson 1Ryrl ShinNo ratings yet
- Anatomy & Physiology of Respiratory SystemDocument12 pagesAnatomy & Physiology of Respiratory SystemDgjj CompuiterNo ratings yet
- The Human Respiratory SystemDocument15 pagesThe Human Respiratory SystemNandita Halder100% (1)
- Respiratory SystemDocument49 pagesRespiratory SystemVishal SharmaNo ratings yet
- The Respiratory SystemDocument16 pagesThe Respiratory SystemAirene Mae Lamputi SupilarNo ratings yet
- ANAPHYDocument10 pagesANAPHYcharles babasaNo ratings yet
- 10th Lecture - Respiratory System 1Document16 pages10th Lecture - Respiratory System 1Zainab Jamal SiddiquiNo ratings yet
- Respiratory System Anatomy, Assessment & Diagnostic TestsDocument24 pagesRespiratory System Anatomy, Assessment & Diagnostic TestsPrince Rener Velasco PeraNo ratings yet
- Respiratory Anatomy - Copy Edited 2022Document28 pagesRespiratory Anatomy - Copy Edited 2022celestelle247No ratings yet
- Respiratory SystemDocument12 pagesRespiratory SystemTricia CabiliNo ratings yet
- Anatomical Basis of The Human Respiratory System: Erial Bahar 2018Document103 pagesAnatomical Basis of The Human Respiratory System: Erial Bahar 2018AmNo ratings yet
- Respiratory System Anatomy and PhysiologyDocument19 pagesRespiratory System Anatomy and PhysiologyKBDNo ratings yet
- Anatomy of The Respiratory SystemDocument37 pagesAnatomy of The Respiratory SystemPal SedNo ratings yet
- Module 5-Respiratory SystemDocument64 pagesModule 5-Respiratory SystemBorja MelanieNo ratings yet
- Anatomy & PhysiologyDocument42 pagesAnatomy & PhysiologyArah Lyn ApiagNo ratings yet
- Exercise IxDocument27 pagesExercise IxShengrace GavinoNo ratings yet
- Respiratory System 1 Physiology 16-11-2018Document25 pagesRespiratory System 1 Physiology 16-11-2018Kangwa MasekaNo ratings yet
- 8 29 23 Lesson 1 Respiratory SystemDocument36 pages8 29 23 Lesson 1 Respiratory SystemMoreen LamsenNo ratings yet
- UntitledDocument62 pagesUntitledManaye MamuyeNo ratings yet
- Respiratory System CopDocument44 pagesRespiratory System CopAsad KHANNo ratings yet
- Respiratory Sysem-2Document78 pagesRespiratory Sysem-2Devrajsinh HadaNo ratings yet
- Respiratory SystemDocument85 pagesRespiratory SystemWilson chumpukaNo ratings yet
- The Respiratory SystemDocument25 pagesThe Respiratory SystemThess Flores CabreraNo ratings yet
- Anatomy and Physiology 2nd Semester BSN Notes, Educational PlatformDocument367 pagesAnatomy and Physiology 2nd Semester BSN Notes, Educational PlatformMuhammad KashifNo ratings yet
- CVS and RSDocument132 pagesCVS and RSclareawambuiNo ratings yet
- The Respiratory System: Anatomy and Histology Course # Pd-317 Dr. Faheema Siddiqi (PHD) Assistant Prof., DcopDocument78 pagesThe Respiratory System: Anatomy and Histology Course # Pd-317 Dr. Faheema Siddiqi (PHD) Assistant Prof., DcopWaseem AfzalNo ratings yet
- Module 4 Respiratory SystemDocument8 pagesModule 4 Respiratory SystemJake Donely C. PaduaNo ratings yet
- Respiratory SystemDocument14 pagesRespiratory SystemRalph QuiambaoNo ratings yet
- An Introduction To: The Respiratory SystemDocument22 pagesAn Introduction To: The Respiratory SystemSHANJIDA ALI RIANo ratings yet
- 11 Respiratory Pharma PrintDocument53 pages11 Respiratory Pharma Printabenezer isayasNo ratings yet
- 1.anatomy of Respiratory SystemDocument73 pages1.anatomy of Respiratory Systemokoti.omutanyi22No ratings yet
- Respiratory SystemDocument8 pagesRespiratory Systemkayeemperado997No ratings yet
- Lecture 5 Respiratory System 1Document61 pagesLecture 5 Respiratory System 1hafiz patahNo ratings yet
- Anatomy of Respiratory SystemDocument57 pagesAnatomy of Respiratory SystemRyan Larsen100% (1)
- Anatomy of Respiratory System: Dr. Dwi Rita Anggraini, MkesDocument64 pagesAnatomy of Respiratory System: Dr. Dwi Rita Anggraini, MkesFira TasyaNo ratings yet
- Lect. 11 Respiratory SystemDocument43 pagesLect. 11 Respiratory Systemflex gyNo ratings yet
- Therespiratorysystem Grade 9Document19 pagesTherespiratorysystem Grade 9ClarkBautistaNo ratings yet
- Therespiratorysystem 130524022043 Phpapp01 TestDocument21 pagesTherespiratorysystem 130524022043 Phpapp01 TestMergel GeconcilloNo ratings yet
- Anatomy and Physiology of PCAPDocument8 pagesAnatomy and Physiology of PCAPMads0% (1)
- Repiratory System I - 2023Document36 pagesRepiratory System I - 2023imaninjaloenkosiniNo ratings yet
- The RespiratoryDocument21 pagesThe RespiratoryPrincess Villasis BaciaNo ratings yet
- Respiratory System - Bio 2 ADocument31 pagesRespiratory System - Bio 2 A20181539No ratings yet
- Respiratory SystemDocument49 pagesRespiratory SystemSimply MiniNo ratings yet
- A &P Overview Respiratory SystemDocument16 pagesA &P Overview Respiratory SystemOpeyemi OmolabakeNo ratings yet
- Respiratory SystemhjhuDocument23 pagesRespiratory SystemhjhuSara ANo ratings yet
- Functional Anatomy of The Respiratory System NoseDocument5 pagesFunctional Anatomy of The Respiratory System NoseEjie Boy IsagaNo ratings yet
- Respiratory System - Anatomy and PhysiologyDocument6 pagesRespiratory System - Anatomy and PhysiologyJay Crishnan Morales CajandingNo ratings yet
- FinalDocument25 pagesFinalShane Patrick PanilagNo ratings yet
- Anatomi Sistem ParuDocument64 pagesAnatomi Sistem ParuMochammad Fariz AmsalNo ratings yet
- Respiratory System PreDocument11 pagesRespiratory System PrecontehamosaNo ratings yet
- 12 - Respiratory PhysiologyDocument62 pages12 - Respiratory PhysiologyRohit K YNo ratings yet
- The Respiratory System: Structure & FunctionDocument72 pagesThe Respiratory System: Structure & FunctionShanique ReidNo ratings yet
- Respiratory System Proj NotesDocument4 pagesRespiratory System Proj NotesLady Lee GuadalupeNo ratings yet
- How Do Humans Breathe? Science Book Age 8 | Children's Biology BooksFrom EverandHow Do Humans Breathe? Science Book Age 8 | Children's Biology BooksNo ratings yet
- Art AppreciationDocument20 pagesArt AppreciationMichelle Antenero100% (1)
- Summative 4.5Document5 pagesSummative 4.5Michelle AnteneroNo ratings yet
- Factors of InfluenceDocument23 pagesFactors of InfluenceMichelle AnteneroNo ratings yet
- RizalDocument15 pagesRizalMichelle AnteneroNo ratings yet
- Writing For New MediaDocument17 pagesWriting For New MediaMichelle AnteneroNo ratings yet
- Pulse OximetryDocument2 pagesPulse OximetryRaja AnuNo ratings yet
- 1best Practices For Migrating SAP Systems To Ora... - Oracle CommunityDocument4 pages1best Practices For Migrating SAP Systems To Ora... - Oracle CommunitymethukupallyNo ratings yet
- Unit 1 Paragraph To EssayDocument55 pagesUnit 1 Paragraph To EssayFrida BrNo ratings yet
- Winitzki - Heidelberg Lectures On Advanced General Relativity 2007Document156 pagesWinitzki - Heidelberg Lectures On Advanced General Relativity 2007winitzkiNo ratings yet
- IoT-Based Water Monitoring SystemDocument5 pagesIoT-Based Water Monitoring SystemManuel Luis Delos SantosNo ratings yet
- 03-Part C3-3 Spec Corrosion ProtectionDocument14 pages03-Part C3-3 Spec Corrosion ProtectionThandabantu MagengeleleNo ratings yet
- Kagan Quiz Quiz TradeDocument2 pagesKagan Quiz Quiz Tradeapi-401932164No ratings yet
- Production Technology of Cow PeaDocument20 pagesProduction Technology of Cow PeaMUHAMMAD AQEELNo ratings yet
- Sharp+Lc c6554u+Difference+Lc 65d64uDocument30 pagesSharp+Lc c6554u+Difference+Lc 65d64uNicholas RileyNo ratings yet
- Human Activities Notes For Form TwoDocument3 pagesHuman Activities Notes For Form TwoedwinmasaiNo ratings yet
- Yoga Retreat in India - Short Course - Yoga Treatment - Yoga TherapyDocument1 pageYoga Retreat in India - Short Course - Yoga Treatment - Yoga TherapynaveenNo ratings yet
- MBA Project Report of DY Patil Distance MBADocument4 pagesMBA Project Report of DY Patil Distance MBAPrakashB144No ratings yet
- Theoretical Foundation For Large-Scale Computations For Nonlinear Material BehaviorDocument411 pagesTheoretical Foundation For Large-Scale Computations For Nonlinear Material BehaviorDalelAzaiezNo ratings yet
- W. Chandraprakaikul Thesis 2008Document409 pagesW. Chandraprakaikul Thesis 2008Ana-Maria RaicuNo ratings yet
- LP Science2 q2w5Document7 pagesLP Science2 q2w5Gaila Mae Abejuela SanorjoNo ratings yet
- Readings in Philippine History-CeDocument11 pagesReadings in Philippine History-Cedeluna.jerremieNo ratings yet
- Irice VarietiesDocument28 pagesIrice VarietiesBlair TorioNo ratings yet
- Connector GuideDocument20 pagesConnector GuideBastian VarelaNo ratings yet
- Ce 8 Sem Advanced Reinforced Cement Concrete Design Winter 2018Document2 pagesCe 8 Sem Advanced Reinforced Cement Concrete Design Winter 2018SandeepNo ratings yet
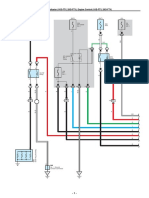
- ECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Document33 pagesECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Erick Lizana Neyra100% (4)
- SP 01 en Power Supply PS 303 ProDocument1 pageSP 01 en Power Supply PS 303 ProRemi de CaesNo ratings yet
- Pili Danica - Dyners Corporation - Case Analysis #1Document2 pagesPili Danica - Dyners Corporation - Case Analysis #1DANICA DANIELA PILINo ratings yet
- Janitza BHB Umg96rmpn enDocument128 pagesJanitza BHB Umg96rmpn enRafael PeÑaNo ratings yet
- My Visit To Agharta PDFDocument83 pagesMy Visit To Agharta PDFDario Riso100% (1)
- M&E Framework For Specimen ReferralsDocument22 pagesM&E Framework For Specimen Referralssabir osmanNo ratings yet
- BCA Syllabus 2016-17 CBCS RevisedDocument83 pagesBCA Syllabus 2016-17 CBCS Revisedmalliknl50% (2)
- 29102015000000B - Boehler DCMS-IG - SWDocument1 page29102015000000B - Boehler DCMS-IG - SWErdinc BayatNo ratings yet
- FDocument11 pagesFanjali yerawarNo ratings yet
- HSE Manager JDDocument2 pagesHSE Manager JDRukun SinagaNo ratings yet
- Sustainable Transportation and Electric VehiclesDocument17 pagesSustainable Transportation and Electric Vehicless131744No ratings yet