You might also like
- Casos de Dat Positivos - AabbDocument101 pagesCasos de Dat Positivos - AabbVictor Vargas100% (1)
- Transfusion Practice Guidelines For Clinic and Laboratory PersonnelDocument98 pagesTransfusion Practice Guidelines For Clinic and Laboratory PersonnelZhayreal Zaki100% (1)
- Disease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesDocument11 pagesDisease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesSara AshurstNo ratings yet
- Platelet Disorders: Practice GapsDocument14 pagesPlatelet Disorders: Practice GapsMichelleHanNo ratings yet
- NCP-risk For BleedingDocument3 pagesNCP-risk For BleedingAce Dioso Tubasco100% (2)
- Clopidogrel Bisulfate (PLOGREL)Document2 pagesClopidogrel Bisulfate (PLOGREL)Kristine Young0% (1)
- Hematology ReviewerDocument15 pagesHematology ReviewerNichol Villalba100% (1)
- AJH Test de MezclasDocument12 pagesAJH Test de Mezclasvalentina campo mejiaNo ratings yet
- Laboratory Studies in Coagulation Disorders: Renu Saxena, Meganathan Kannan and Ved P ChoudhryDocument7 pagesLaboratory Studies in Coagulation Disorders: Renu Saxena, Meganathan Kannan and Ved P ChoudhryJulius FrondaNo ratings yet
- A Normal Ida Des de La Coagulacion 2010 ASADocument6 pagesA Normal Ida Des de La Coagulacion 2010 ASAJohan Lanzziano SilvaNo ratings yet
- Vertebral Canal Haematoma and Coagulopathy - BjaDocument2 pagesVertebral Canal Haematoma and Coagulopathy - BjaRENAULTNo ratings yet
- Nursing Care Plan StrokeDocument2 pagesNursing Care Plan StrokeA HNo ratings yet
- Pseudo ThrombocytopeniaDocument10 pagesPseudo ThrombocytopeniaKamran DawoodNo ratings yet
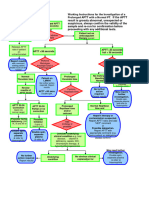
- Working Instructions Investigation of Prolonged APTTDocument1 pageWorking Instructions Investigation of Prolonged APTTtadeariba1No ratings yet
- 114 - Coagulation DisordersDocument9 pages114 - Coagulation Disorders4g8psyr2qfNo ratings yet
- Trombositopenia AfpDocument5 pagesTrombositopenia AfpFadhila RamadhaniNo ratings yet
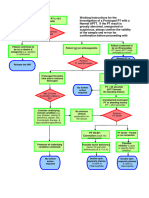
- Working Instructions Investigation of Prolonged PTDocument1 pageWorking Instructions Investigation of Prolonged PTtadeariba1No ratings yet
- Fix Bm1 - Dental Surgery - Haemorrhage IIDocument4 pagesFix Bm1 - Dental Surgery - Haemorrhage IIannisa anindyaNo ratings yet
- Grand RoundsDocument55 pagesGrand Roundsapi-716714980No ratings yet
- BR J Haematol - 2017 - Donadieu - Congenital Neutropenia in The Era of Genomics Classification Diagnosis and NaturalDocument18 pagesBR J Haematol - 2017 - Donadieu - Congenital Neutropenia in The Era of Genomics Classification Diagnosis and NaturalTomasz GórskiNo ratings yet
- 197 FullDocument3 pages197 FullArum NafilahNo ratings yet
- PDF Nursing Care PlanDocument16 pagesPDF Nursing Care PlanMichael MabiniNo ratings yet
- TRANSF Sangre MapaDocument1 pageTRANSF Sangre MapaSiu Lin WongNo ratings yet
- Jurnal PendarahanDocument15 pagesJurnal Pendarahanイアン リムホト ザナガNo ratings yet
- Drug StudyDocument16 pagesDrug Studykint manlangitNo ratings yet
- Risk For Deficient Fluid VolumeDocument2 pagesRisk For Deficient Fluid VolumeMariella BadongenNo ratings yet
- Concept Map Aplastic Anemia 212 1Document1 pageConcept Map Aplastic Anemia 212 1S AustinNo ratings yet
- Inpatient Inherited Thrombophilia Testing: Choosing Wisely: Things We Do For No ReasonDocument4 pagesInpatient Inherited Thrombophilia Testing: Choosing Wisely: Things We Do For No Reasonkishore kumar meelNo ratings yet
- 2017 Pediatric AnesthDocument2 pages2017 Pediatric AnesthAirwayNo ratings yet
- Pathology Outlines - Abnormal PT and PTT - CausesDocument1 pagePathology Outlines - Abnormal PT and PTT - CausesShane AranetaNo ratings yet
- BLEEDINGDocument5 pagesBLEEDINGKezia ImanuellaNo ratings yet
- 2003 Purpura Trombocitopenica Idiopatica en AdultosDocument5 pages2003 Purpura Trombocitopenica Idiopatica en AdultosConrado Vera PinedaNo ratings yet
- Int J Lab Hematology - 2015 - Adcock - Pearls and Pitfalls in Factor Inhibitor AssaysDocument9 pagesInt J Lab Hematology - 2015 - Adcock - Pearls and Pitfalls in Factor Inhibitor AssaysMehmood-ul-Hasan MalikNo ratings yet
- Coagulation TestDocument5 pagesCoagulation TestZahid HussainNo ratings yet
- Diagnostics Aptt PTTDocument1 pageDiagnostics Aptt PTTi.jesylbpNo ratings yet
- The Evaluation of Hematologic Screening and Perioperative Management in Patients With Noonan Syndrome: A Retrospective Chart ReviewDocument11 pagesThe Evaluation of Hematologic Screening and Perioperative Management in Patients With Noonan Syndrome: A Retrospective Chart ReviewMariaNo ratings yet
- Transfusion MasivaDocument8 pagesTransfusion MasivaMatias FlammNo ratings yet
- HR 11 1 7732Document5 pagesHR 11 1 7732ResidenPatKlin Juli2022No ratings yet
- Diff DiagnDocument3 pagesDiff DiagnАбдул Насер МохаммадізмаелNo ratings yet
- Kegawatan Hematologis Pada Neonatus Kritis - DR Azharry, SpADocument59 pagesKegawatan Hematologis Pada Neonatus Kritis - DR Azharry, SpAsonia imaNo ratings yet
- Thrombocytopenia: An Update: K. J. Smock, S. L. PerkinsDocument10 pagesThrombocytopenia: An Update: K. J. Smock, S. L. PerkinsRevathy GunaseelanNo ratings yet
- Rare Bleeding DisordersDocument11 pagesRare Bleeding DisordersJovanna OrtuñoNo ratings yet
- Standardization of Prothrombin Time:International Normalized Ratio (PT:INR)Document8 pagesStandardization of Prothrombin Time:International Normalized Ratio (PT:INR)GABRIELA HERRERANo ratings yet
- Assess Extrinsic Pathway (Tissue Factor Pathway) Prothrombin Time / PT Test / INRDocument3 pagesAssess Extrinsic Pathway (Tissue Factor Pathway) Prothrombin Time / PT Test / INRKristin DouglasNo ratings yet
- Best Diagnostic Centre in Lucknow: Advanced Cardiovascular Genomics Risk Assessment PanelDocument1 pageBest Diagnostic Centre in Lucknow: Advanced Cardiovascular Genomics Risk Assessment Panelrmlpath12No ratings yet
- APTT & PT Mixing StudiesDocument9 pagesAPTT & PT Mixing StudiesmarrowbiopsyNo ratings yet
- DIC in PediatricsDocument11 pagesDIC in PediatricsRizky LumalessilNo ratings yet
- Heart FailureDocument8 pagesHeart FailureKKUTC PerlisNo ratings yet
- Hemostaticdisorders Associatedwith Hepatobiliarydisease: Cynthia R.L. WebsterDocument15 pagesHemostaticdisorders Associatedwith Hepatobiliarydisease: Cynthia R.L. WebsterJuan DuasoNo ratings yet
- Bleeding DisordersDocument92 pagesBleeding DisordersIsaac MwangiNo ratings yet
- Approach To BleedingDocument7 pagesApproach To BleedingMunish DograNo ratings yet
- Blood Component ChirrosisDocument8 pagesBlood Component ChirrosisFernando JiménezNo ratings yet
- Platelets PDFDocument65 pagesPlatelets PDFLana AmerieNo ratings yet
- How To Approach A Patient With Bleeding?: ISTH Advanced Training Course, Portugal March 2014Document100 pagesHow To Approach A Patient With Bleeding?: ISTH Advanced Training Course, Portugal March 2014ramanNo ratings yet
- CLG Chapter5 PDFDocument5 pagesCLG Chapter5 PDFIberisNo ratings yet
- Things To Look For During Morning RoundDocument3 pagesThings To Look For During Morning RoundTom YipNo ratings yet
- Absolute and Relative Contraindications To IV Rt-PA For Acute Ischemic StrokeDocument12 pagesAbsolute and Relative Contraindications To IV Rt-PA For Acute Ischemic Strokeأبو أويس شرف الدينNo ratings yet
- In Ammation in Heart Failure: JACC State-of-the-Art ReviewDocument17 pagesIn Ammation in Heart Failure: JACC State-of-the-Art ReviewAhmad FauzanNo ratings yet
- The Geriatric PatientDocument13 pagesThe Geriatric PatientismailcemNo ratings yet
- Glanz MansDocument7 pagesGlanz Mansthroaty rhinoNo ratings yet
- Handbook of Inpatient CardiologyFrom EverandHandbook of Inpatient CardiologyBryan J. WellsNo ratings yet
- Scandinavian Journal of Clinical and Laboratory InvestigationDocument8 pagesScandinavian Journal of Clinical and Laboratory Investigationraiden thunderNo ratings yet
- (2005) AAP Thrombocytopenia in ChildhoddDocument11 pages(2005) AAP Thrombocytopenia in ChildhoddFabiola Vania FeliciaNo ratings yet
- Blood GroupingDocument8 pagesBlood GroupingdevarajNo ratings yet
- Dabl Educational TrustMonitors For Self-Measurement of Blood Pressure (SBPM)Document1 pageDabl Educational TrustMonitors For Self-Measurement of Blood Pressure (SBPM)iranbengoaNo ratings yet
- 3.2 Diagnostic Procedures (Denver)Document44 pages3.2 Diagnostic Procedures (Denver)DPNS 0024 NOR ARINA BINTI AB HAMIDNo ratings yet
- Approach To The Patient With AnemiaDocument37 pagesApproach To The Patient With AnemiaSumeet PratapNo ratings yet
- UpToDate Massive Blood TransfusionDocument10 pagesUpToDate Massive Blood TransfusionAlice HuiiNo ratings yet
- Evaluation and Comparison of The New Mindray BC-6200 Hematology Analyzer With ADVIA 2120iDocument8 pagesEvaluation and Comparison of The New Mindray BC-6200 Hematology Analyzer With ADVIA 2120iGABRIELA HERRERANo ratings yet
- ANTIBODY SCREENING - FinalDocument4 pagesANTIBODY SCREENING - FinalHaniya KhanNo ratings yet
- Hemolytic Disease of The NewbornDocument7 pagesHemolytic Disease of The NewbornLara CarisaNo ratings yet
- Pmls II Lesson 3 Circulatory SystemDocument7 pagesPmls II Lesson 3 Circulatory SystemanaodtohanNo ratings yet
- Haematological Profile and Erythrocyte Indices in Different Breeds of PoultryDocument4 pagesHaematological Profile and Erythrocyte Indices in Different Breeds of PoultrySukma WijayaNo ratings yet
- Multiple Alleles ABO Quiz 6B: AnswersDocument2 pagesMultiple Alleles ABO Quiz 6B: AnswersAlvie GaydaNo ratings yet
- Xerostomia PDFDocument7 pagesXerostomia PDFSak BolNo ratings yet
- Blood Storage Policy and ProcedureDocument3 pagesBlood Storage Policy and ProcedureMohamed AllamNo ratings yet
- MARCH 31 (S) T25 Thu NganDocument8 pagesMARCH 31 (S) T25 Thu NganChi Hoàng Minh TrươngNo ratings yet
- Department of Haematology - : Mr. Nagaraja N 72yr 0Mth 3days Male Uhid Sin /LRN W/Bno/RefnoDocument1 pageDepartment of Haematology - : Mr. Nagaraja N 72yr 0Mth 3days Male Uhid Sin /LRN W/Bno/RefnoPrashanth NNo ratings yet
- HRM Week 2 - Introduction 2020 - PrintDocument34 pagesHRM Week 2 - Introduction 2020 - PrintShiv SookunNo ratings yet
- Ratio Assessment Exam Blood BankDocument3 pagesRatio Assessment Exam Blood BankJayniel Erys MollenoNo ratings yet
- (A Unit of Shriman Enterprises), Nurpur, Pathankot Road, Jalandhar, Punjab 144012Document16 pages(A Unit of Shriman Enterprises), Nurpur, Pathankot Road, Jalandhar, Punjab 144012J KNo ratings yet
- HasanahDocument10 pagesHasanahnia kurniawatiNo ratings yet
- NCM1-18 0122Document3 pagesNCM1-18 0122CeeNo ratings yet
- Hematology TestsDocument7 pagesHematology TestsVenkatesan VidhyaNo ratings yet
- Result: Call Center: 01756963308Document2 pagesResult: Call Center: 01756963308Activity ManagerNo ratings yet
- Secondary Hemostasis Lab TestsDocument2 pagesSecondary Hemostasis Lab TestsWho KnowsNo ratings yet
- Acute Infectious Purpura FulminansDocument15 pagesAcute Infectious Purpura FulminansFranklin Aranda100% (2)
- Clotting Factors Platelets: Optimal Use ofDocument316 pagesClotting Factors Platelets: Optimal Use ofJonathan Alfaro LCBSUCRNo ratings yet