You might also like
- Anemia ChartDocument1 pageAnemia ChartBetsy Brown ByersmithNo ratings yet
- RBC Morphology and InclusionsDocument3 pagesRBC Morphology and InclusionsDeomicah SolanoNo ratings yet
- High Voltage X-Ray GeneratorDocument52 pagesHigh Voltage X-Ray GeneratorMunish Dogra100% (3)
- Tugas Vascular AnomaliesDocument26 pagesTugas Vascular AnomaliesElno TatipikalawanNo ratings yet
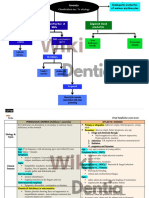
- Concept MapDocument4 pagesConcept MapDud AccNo ratings yet
- Activity 6 - Drug StudyDocument14 pagesActivity 6 - Drug StudyAl-Mujib TanogNo ratings yet
- BloodDocument6 pagesBloodBell GatesNo ratings yet
- Drug Study CISPLATINDocument2 pagesDrug Study CISPLATINCorrine IvyNo ratings yet
- MED (App17) - Approach To AnaemiaDocument5 pagesMED (App17) - Approach To AnaemiaFlora XuNo ratings yet
- Abruptio Placenta PathophysiologyDocument4 pagesAbruptio Placenta Pathophysiologyjamie carpioNo ratings yet
- Compatibility Testing For Blood TransfusionDocument40 pagesCompatibility Testing For Blood TransfusionMunish Dogra100% (4)
- Disseminated Intravascular CoagulationDocument12 pagesDisseminated Intravascular CoagulationMunish Dogra100% (1)
- DIC PathophysiologyDocument1 pageDIC Pathophysiologykathy100% (1)
- Lupus Erythematosus CellDocument58 pagesLupus Erythematosus CellMunish Dogra100% (1)
- Radiation HazardsDocument40 pagesRadiation HazardsMunish Dogra100% (1)
- Hematoxylin Stain Its Importance in HistologyDocument35 pagesHematoxylin Stain Its Importance in HistologyMunish Dogra60% (5)
- Vit K Drug StudyDocument2 pagesVit K Drug Studyelle100% (3)
- 2.2.3.1 Diathesis HemorragikDocument20 pages2.2.3.1 Diathesis HemorragikaiysahmirzaNo ratings yet
- Coombs' TestDocument42 pagesCoombs' TestMunish Dogra100% (1)
- Risk AnalysisDocument50 pagesRisk AnalysisMunish DograNo ratings yet
- Malabsorption A Clinical ApproachDocument42 pagesMalabsorption A Clinical ApproachMunish DograNo ratings yet
- Week 13 Disorders of Secondary Hemostasis LecDocument8 pagesWeek 13 Disorders of Secondary Hemostasis LecCzarina Mae IlaganNo ratings yet
- Seco Ndar Y HEM Osta SIS (Coa Gula Tion Fact OR) : Mucocutaneous - PetechiaeDocument7 pagesSeco Ndar Y HEM Osta SIS (Coa Gula Tion Fact OR) : Mucocutaneous - Petechiaea a r o n b a u t i s t aNo ratings yet
- Dissiminated Intravascular Coagulation PathoDocument2 pagesDissiminated Intravascular Coagulation Pathoapi-341263362No ratings yet
- FINAL Student Preparation Surgical Client Case and Safe Medication AdministrationDocument3 pagesFINAL Student Preparation Surgical Client Case and Safe Medication AdministrationsaemhatdsbNo ratings yet
- Hematology 2 ReviewerDocument4 pagesHematology 2 ReviewerAnn YeongNo ratings yet
- Bleeding Disorders: VASCULAR AbnormalityDocument21 pagesBleeding Disorders: VASCULAR Abnormalityokwadha simionNo ratings yet
- Kelainan Perdarahan Kelainan PembekuanDocument28 pagesKelainan Perdarahan Kelainan PembekuanEga FlorenceNo ratings yet
- Drug Study. GeamhDocument5 pagesDrug Study. GeamhMacky RobentaNo ratings yet
- Clotting Bleeding: Changes in Liver Disease HemostasisDocument2 pagesClotting Bleeding: Changes in Liver Disease HemostasisRismha SlidesNo ratings yet
- Diff DiagnDocument3 pagesDiff DiagnАбдул Насер МохаммадізмаелNo ratings yet
- LIGHT Venous Thromboembolism Dr. ConstantinoDocument7 pagesLIGHT Venous Thromboembolism Dr. ConstantinoMiguel Cuevas DolotNo ratings yet
- DocumentDocument4 pagesDocumentALi AL-kwafiNo ratings yet
- Cap 14Document49 pagesCap 14Saul RivasNo ratings yet
- Bleeding Disorder ApproachDocument9 pagesBleeding Disorder Approachmalik003No ratings yet
- Hematology 101: Interpreting Lab Results - Patterns and PitfallsDocument55 pagesHematology 101: Interpreting Lab Results - Patterns and PitfallsAmorrita Puspita Ratu100% (1)
- Pratique: Bleeding Disorders of Importance in Dental Care and Related Patient ManagementDocument7 pagesPratique: Bleeding Disorders of Importance in Dental Care and Related Patient ManagementSaurabh SatheNo ratings yet
- Family History - Heriditory DisordersDocument3 pagesFamily History - Heriditory DisordersSanthosh KumarNo ratings yet
- Degenevie - HematologyDocument71 pagesDegenevie - Hematologykkq7fhkwvkNo ratings yet
- How To Approach A Patient With Bleeding?: ISTH Advanced Training Course, Portugal March 2014Document100 pagesHow To Approach A Patient With Bleeding?: ISTH Advanced Training Course, Portugal March 2014ramanNo ratings yet
- Concept Map - Polycythemia VeraDocument1 pageConcept Map - Polycythemia VeraMaej Marie OragaNo ratings yet
- Intravascular Extravascular: Fe Storage Tibc SerumDocument2 pagesIntravascular Extravascular: Fe Storage Tibc Serumazhar hussinNo ratings yet
- Bleeding Disorders A Clinical Approach: PACES Station 5Document9 pagesBleeding Disorders A Clinical Approach: PACES Station 5Ahmed AlhalwajiNo ratings yet
- Bleeding DisordersDocument92 pagesBleeding DisordersIsaac MwangiNo ratings yet
- anemia summary كاملDocument10 pagesanemia summary كاملmdio midoNo ratings yet
- Apixaban Cme SlidesDocument26 pagesApixaban Cme SlidesBharat GuptaNo ratings yet
- AspirinDocument3 pagesAspirinKim SunooNo ratings yet
- Clinical Approach of Bleeding Problems in Childhood: Novie Amelia ChozieDocument38 pagesClinical Approach of Bleeding Problems in Childhood: Novie Amelia ChoziebennyrolandnababanNo ratings yet
- Cara Mendiagnose AnemiaDocument1 pageCara Mendiagnose AnemiaMuchlissatus Lisa MedicalbookNo ratings yet
- Drug StudyDocument1 pageDrug Studymickks098No ratings yet
- Hemophilia and Coagulation Disorders: DR Nishant VermaDocument68 pagesHemophilia and Coagulation Disorders: DR Nishant VermaЮлия ЦыгановаNo ratings yet
- Anemia Testing Algorithm PDFDocument1 pageAnemia Testing Algorithm PDFIrene Demegillo SalongaNo ratings yet
- AnemiaDocument2 pagesAnemiaRed DiggerNo ratings yet
- Anemia AplastikDocument1 pageAnemia AplastikAlika Nigandiva41No ratings yet
- DR Anna Mira Lubis - Diagnostic Approach of ThrombocytopeniaDocument36 pagesDR Anna Mira Lubis - Diagnostic Approach of Thrombocytopeniayosua simarmataNo ratings yet
- Kegawatan Hematologis Pada Neonatus Kritis - DR Azharry, SpADocument59 pagesKegawatan Hematologis Pada Neonatus Kritis - DR Azharry, SpAsonia imaNo ratings yet
- Disease Patho Manifestations Assessment Labs Tx/Nursing Disseminated Intravascular CoagulationDocument1 pageDisease Patho Manifestations Assessment Labs Tx/Nursing Disseminated Intravascular CoagulationSara SabraNo ratings yet
- Vit K Drug Study PDFDocument2 pagesVit K Drug Study PDFA sisonNo ratings yet
- Bleeding Disorders Tandem Desember 2019Document47 pagesBleeding Disorders Tandem Desember 2019reshaNo ratings yet
- Bleeding Disorders Tandem Desember 2019Document47 pagesBleeding Disorders Tandem Desember 2019reshaNo ratings yet
- Healthcare - Drug Study Worksheet - Penicillin G SodiumDocument2 pagesHealthcare - Drug Study Worksheet - Penicillin G SodiumBenjamin CañalitaNo ratings yet
- Microcytic Type Aeitology Clinical Features Investigations ManagementDocument7 pagesMicrocytic Type Aeitology Clinical Features Investigations ManagementJason AnthonyNo ratings yet
- Tiempos en Malformaciones VascularesDocument7 pagesTiempos en Malformaciones VascularesJosue AyalaNo ratings yet
- Disseminated Intravascular Coagulation: Robert R. Zaid D.O. Genesys Regional Medical Center Pgy-IDocument37 pagesDisseminated Intravascular Coagulation: Robert R. Zaid D.O. Genesys Regional Medical Center Pgy-IGilang KusdinarNo ratings yet
- Anticoagulation TherapyFrom EverandAnticoagulation TherapyJoe F. LauNo ratings yet
- Compendium on Cardiomyopathies - Basics, Therapeutics, and PerspectivesFrom EverandCompendium on Cardiomyopathies - Basics, Therapeutics, and PerspectivesNo ratings yet
- Ionising Radiation and Living ThingsDocument23 pagesIonising Radiation and Living ThingsMunish DograNo ratings yet
- Radiation HazardsDocument32 pagesRadiation HazardsMunish DograNo ratings yet
- Every Child Is SpecialDocument1 pageEvery Child Is SpecialMunish DograNo ratings yet
- THALASSEMIADocument49 pagesTHALASSEMIAMunish DograNo ratings yet
- School Libraries and ReadingDocument133 pagesSchool Libraries and ReadingMunish DograNo ratings yet
- Bone Marrow Strcuture and FunctionDocument25 pagesBone Marrow Strcuture and FunctionMunish DograNo ratings yet
- The Feasibility of A Community Based Health Insurance (CBHI) at Wayanad, KeralaDocument43 pagesThe Feasibility of A Community Based Health Insurance (CBHI) at Wayanad, Keralatapz07No ratings yet
- Health Financing Protecting The PoorDocument8 pagesHealth Financing Protecting The PoorMunish DograNo ratings yet