You might also like
- Pediatric Liver Intensive CareFrom EverandPediatric Liver Intensive CareNaresh ShanmugamNo ratings yet
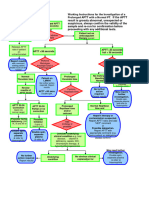
- Working Instructions Investigation of Prolonged APTTDocument1 pageWorking Instructions Investigation of Prolonged APTTtadeariba1No ratings yet
- PDF Nursing Care PlanDocument16 pagesPDF Nursing Care PlanMichael MabiniNo ratings yet
- Dat e Physicians Order RationaleDocument4 pagesDat e Physicians Order Rationaleember parkNo ratings yet
- Anae15291 Sup 0001 Appendixs1Document10 pagesAnae15291 Sup 0001 Appendixs1iamseraNo ratings yet
- 1st Half GORDON FUNCTIONAL HEALTH PATTERN - Head InjuryDocument2 pages1st Half GORDON FUNCTIONAL HEALTH PATTERN - Head InjuryTerence SalamatNo ratings yet
- Mixing Studies 1pp 08-13-15.pptx 0 PDFDocument49 pagesMixing Studies 1pp 08-13-15.pptx 0 PDFKholifah LintangNo ratings yet
- Haematology House Officer GuideDocument7 pagesHaematology House Officer GuidePuzzlingNo ratings yet
- Haematology House Officer GuideDocument7 pagesHaematology House Officer GuidePuzzlingNo ratings yet
- Thera Hypertension Pregnant Group 1 PDFDocument3 pagesThera Hypertension Pregnant Group 1 PDFJanet Jane de RidderNo ratings yet
- Hema 2 Lab: Coagulation Tests: PT and ApttDocument5 pagesHema 2 Lab: Coagulation Tests: PT and ApttGerly MaglangitNo ratings yet
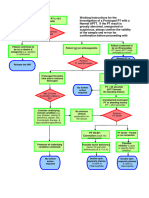
- Working Instructions Investigation of Prolonged PTDocument1 pageWorking Instructions Investigation of Prolonged PTtadeariba1No ratings yet
- Drug Study (Concept Map) : Nursing Intervention IndicationDocument4 pagesDrug Study (Concept Map) : Nursing Intervention IndicationdasdadadadaNo ratings yet
- Abdominal PDFDocument1 pageAbdominal PDFChakra BaktiNo ratings yet
- TRANSF Sangre MapaDocument1 pageTRANSF Sangre MapaSiu Lin WongNo ratings yet
- Objective Data Diagnosis Goals Interventions EvaluationDocument2 pagesObjective Data Diagnosis Goals Interventions EvaluationHira Akram Hira AkramNo ratings yet
- Drug StudyDocument9 pagesDrug StudyAysaaa DCNo ratings yet
- A Case of Electrical BurnDocument34 pagesA Case of Electrical BurnryanyganaNo ratings yet
- Uterine Hyperstimulation, Management of - ABMU Maternity Guideline 2018Document7 pagesUterine Hyperstimulation, Management of - ABMU Maternity Guideline 2018Chintya MarcellinNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Pharm Final Exam NotesDocument26 pagesPharm Final Exam Noteskatiana louis100% (1)
- Platelet Transfusion Guidelines NewDocument5 pagesPlatelet Transfusion Guidelines Newgautam harshNo ratings yet
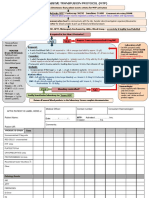
- Baseline:: Notify Transfusion Laboratory To: Activate MTP'. Footscray: 56292 Sunshine: 51480 Allocate Team RolesDocument2 pagesBaseline:: Notify Transfusion Laboratory To: Activate MTP'. Footscray: 56292 Sunshine: 51480 Allocate Team RolesDumindu PereraNo ratings yet
- Hema312 Lab Finals 1Document4 pagesHema312 Lab Finals 1JPNo ratings yet
- Anaesthesia JottingDocument2 pagesAnaesthesia JottingChinedu H. DuruNo ratings yet
- Bleeding DisordersDocument62 pagesBleeding DisordersxtineNo ratings yet
- Drug Study Prostate CancerDocument9 pagesDrug Study Prostate CancerMina RacadioNo ratings yet
- 9 - Anticoagulant Drugs (Final)Document17 pages9 - Anticoagulant Drugs (Final)wllmaanka4No ratings yet
- Deep Vein ThrombosisDocument5 pagesDeep Vein Thrombosisampogison08No ratings yet
- MODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsDocument7 pagesMODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsalliahjaneadlawanNo ratings yet
- Enoxaparin - Safe Prescribing - Check It Out 1Document3 pagesEnoxaparin - Safe Prescribing - Check It Out 1Zaid DewachiNo ratings yet
- Transurethral Resection of The Prostate (TURP)Document16 pagesTransurethral Resection of The Prostate (TURP)Princess Brigitte R. PATE�ANo ratings yet
- Troponin PathwayDocument1 pageTroponin PathwayAllana AngelesNo ratings yet
- Doctors OrderDocument2 pagesDoctors Ordermarc_alvin0% (1)
- Antiplatelets Anticoagulant Drugs 1668083619Document12 pagesAntiplatelets Anticoagulant Drugs 1668083619Nehal ElnagarNo ratings yet
- Heparin: AnticoagulantsDocument8 pagesHeparin: AnticoagulantsThierd Cañete III100% (1)
- Reteplase (MIRel)Document23 pagesReteplase (MIRel)Jhoann JamanilaNo ratings yet
- Analytical Method Development and Validation of RP-HPLC For Estimation of Pregabalin and Epalrestat in Pure and Pharmaceutical Dosage FormDocument10 pagesAnalytical Method Development and Validation of RP-HPLC For Estimation of Pregabalin and Epalrestat in Pure and Pharmaceutical Dosage FormSaravanan RamNo ratings yet
- DabigatranDocument25 pagesDabigatranNagesh JadavNo ratings yet
- History Lab Investigation: EclampsiaDocument5 pagesHistory Lab Investigation: EclampsiaShafiq Ur RahmanNo ratings yet
- 01 Cir 97 3 251Document6 pages01 Cir 97 3 251Kamonashis Sarkar TendulNo ratings yet
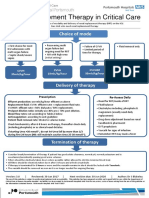
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Jurnal Gerd 3Document6 pagesJurnal Gerd 3sega maulanaNo ratings yet
- Update On Clinical Management - PrivateDocument57 pagesUpdate On Clinical Management - PrivateJashveerBediNo ratings yet
- Gyne Removals SamplexDocument43 pagesGyne Removals SamplexHa Jae kyeongNo ratings yet
- Lab Screening For Bleeding DisordersDocument40 pagesLab Screening For Bleeding Disordersmichael firmanNo ratings yet
- Management of Chronic ITP: TPO-R Agonist Vs ImmunosuppressantDocument29 pagesManagement of Chronic ITP: TPO-R Agonist Vs ImmunosuppressantNiken AmritaNo ratings yet
- Venous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDDocument23 pagesVenous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- Vertebral Canal Haematoma and Coagulopathy - BjaDocument2 pagesVertebral Canal Haematoma and Coagulopathy - BjaRENAULTNo ratings yet
- Prothrombin Time and International Normalized Ratio (PT - INR) - Lab Tests OnlineDocument11 pagesProthrombin Time and International Normalized Ratio (PT - INR) - Lab Tests OnlineAlyaNo ratings yet
- Lesson 42 Laboratory ValuesDocument4 pagesLesson 42 Laboratory ValuesDarren RossNo ratings yet
- Baby Case Study (FINAL)Document44 pagesBaby Case Study (FINAL)Rouie Björn ABrianNo ratings yet
- Infinosis NT-proBNP IN047705 enDocument2 pagesInfinosis NT-proBNP IN047705 enMeditech visionbdNo ratings yet
- Itp 2021Document64 pagesItp 2021Victoria MalakNo ratings yet
- Course in The Ward Intracerebral HemorrhageDocument14 pagesCourse in The Ward Intracerebral HemorrhageJeffrey Dela CruzNo ratings yet
- ICU One Pager - Pulmonary Embolism RX PDFDocument1 pageICU One Pager - Pulmonary Embolism RX PDFAbdul RaufNo ratings yet
- Diabetes Mellitus TranscribingDocument23 pagesDiabetes Mellitus TranscribingJasmin B. ERMITANo ratings yet
- Epo DrugstudyDocument3 pagesEpo DrugstudyKhatlen BagaresNo ratings yet
- 1 - DopamineDocument1 page1 - DopaminedianneangelaNo ratings yet
- 1case HFDocument38 pages1case HFshaymhNo ratings yet
- Patient Education: Hyperemesis Gravidarum (The Basics) - UpToDateDocument1 pagePatient Education: Hyperemesis Gravidarum (The Basics) - UpToDateKezia ImanuellaNo ratings yet
- Approach To Evaluating Pregnant Patients With Elevated Liver Biochemical and Function Tests - UpToDaDocument1 pageApproach To Evaluating Pregnant Patients With Elevated Liver Biochemical and Function Tests - UpToDaKezia ImanuellaNo ratings yet
- Guidelines To The Nurse's Role in The ManagementDocument16 pagesGuidelines To The Nurse's Role in The ManagementKezia ImanuellaNo ratings yet
- DISORDERS of The MEDIASTINUMDocument37 pagesDISORDERS of The MEDIASTINUMKezia ImanuellaNo ratings yet
- Aneurysmal DiseaseDocument33 pagesAneurysmal DiseaseKezia Imanuella100% (1)
- Intraop - Hemorrage and Bleeding DiathesisDocument1 pageIntraop - Hemorrage and Bleeding DiathesisKezia ImanuellaNo ratings yet
- Cheer SceneDocument6 pagesCheer SceneKezia ImanuellaNo ratings yet
- Clinical Microscopy Services PDFDocument5 pagesClinical Microscopy Services PDFNaima AmrosiNo ratings yet
- Pelvix Organ ProlapsDocument5 pagesPelvix Organ ProlapskazugawaNo ratings yet
- Observation On Therapeutic Effects of Cupping Therapy For Allergic RhinitisDocument2 pagesObservation On Therapeutic Effects of Cupping Therapy For Allergic Rhinitischakir BezzahiNo ratings yet
- Case Study For Diagnosis of DiseaseDocument29 pagesCase Study For Diagnosis of DiseaseFirifan DiribaNo ratings yet
- AAST Renal Injury ScaleDocument11 pagesAAST Renal Injury ScaleyuenkeithNo ratings yet
- Abnormal Psych CH 9 & 10 Power Pts 16Document38 pagesAbnormal Psych CH 9 & 10 Power Pts 16Natalya CespedesNo ratings yet
- 4th Year Online Class 16 - 21 KartikDocument3 pages4th Year Online Class 16 - 21 Kartikradha poudelNo ratings yet
- Burn Mcqs2Document11 pagesBurn Mcqs2Musa yohanaNo ratings yet
- A Patient of Poisoning in ICU (Ankit Jain)Document48 pagesA Patient of Poisoning in ICU (Ankit Jain)SharryNo ratings yet
- MohammediaDocument3 pagesMohammediasetata7128No ratings yet
- Therapeutic Conference: FacilitatorsDocument4 pagesTherapeutic Conference: FacilitatorsJolaine ValloNo ratings yet
- Badie 2004Document11 pagesBadie 2004Bhayu Rizallinoor BhayuNo ratings yet
- Angina Pectoris: History TakingDocument7 pagesAngina Pectoris: History TakingNavpreet KaurNo ratings yet
- Lifetree Gut Relax, An Ayurvedic Health SupplementDocument13 pagesLifetree Gut Relax, An Ayurvedic Health SupplementLifetree WorldNo ratings yet
- Drug StudyDocument3 pagesDrug StudySherlyn Delos ReyesNo ratings yet
- ABO-Rh Blood Typing With Synthetic Blood: Teacher'S Manual and Student GuideDocument32 pagesABO-Rh Blood Typing With Synthetic Blood: Teacher'S Manual and Student GuideMylan Gaston100% (1)
- Blood Cells LabDocument7 pagesBlood Cells LabKameron WardNo ratings yet
- The Mind Body Interaction in DiseaseDocument8 pagesThe Mind Body Interaction in DiseaseYuli MSNo ratings yet
- Shen Ling Bai Zhu San - 參苓白術散 - Ginseng, Poria and Atractylodis Macrocephalae Powder - 參苓白術散 - Ginseng and Atractylodes Formula - Chinese Herbs - American Dragon - Dr Joel Penner OMD, LAcDocument9 pagesShen Ling Bai Zhu San - 參苓白術散 - Ginseng, Poria and Atractylodis Macrocephalae Powder - 參苓白術散 - Ginseng and Atractylodes Formula - Chinese Herbs - American Dragon - Dr Joel Penner OMD, LAcangelesarenas0% (1)
- Hinoguin, Jocelyn Patana 1851114785Document3 pagesHinoguin, Jocelyn Patana 1851114785Paulline Joyce HinoguinNo ratings yet
- PhysioEx Exercise 7 Activity 1Document6 pagesPhysioEx Exercise 7 Activity 1Jorge CuevaNo ratings yet
- Questions About KidneysDocument30 pagesQuestions About KidneysKristine Mae AbrasaldoNo ratings yet
- Ganglion CystDocument3 pagesGanglion CystJuko FernandezNo ratings yet
- Burns SeminarDocument66 pagesBurns SeminarPratibha Thakur100% (1)
- Surgery Surgical Nursing Objs With AnsDocument136 pagesSurgery Surgical Nursing Objs With AnsmintahmeshackbenjaminNo ratings yet
- Position PaperDocument4 pagesPosition PaperBing Cossid Quinones CatzNo ratings yet
- IDA-PEPSODENT Poster PresentationDocument2 pagesIDA-PEPSODENT Poster PresentationvandarsNo ratings yet
- My Own Life: by Oliver SacksDocument4 pagesMy Own Life: by Oliver SacksAmerigo VespucciNo ratings yet
- Literature Review: The Relationship Between Sleep Patterns and The Incidence of Hypertension in The ElderlyDocument22 pagesLiterature Review: The Relationship Between Sleep Patterns and The Incidence of Hypertension in The ElderlyCalvin permana pinemNo ratings yet
- Cataract DissertationDocument6 pagesCataract DissertationPaperWritingHelpEverett100% (1)