You might also like
- Effect of Nicotine On PlantsDocument27 pagesEffect of Nicotine On Plantsajaysharma196861910% (1)
- Chapmans ReflexesDocument10 pagesChapmans ReflexesNickosteo100% (9)
- 2016 HESI Exam Version 2Document12 pages2016 HESI Exam Version 2Jennifer Anderson Wilson100% (1)
- God's PharmacyDocument18 pagesGod's PharmacyTrack and Trace Committee100% (3)
- Case Study Pneumonia)Document20 pagesCase Study Pneumonia)Jai - Ho83% (6)
- Drugs QT IntervalDocument3 pagesDrugs QT Intervalsubhan fadilahNo ratings yet
- Floracopeia Essential Oil EbookDocument61 pagesFloracopeia Essential Oil EbookOana Algasovschi100% (1)
- Anticoagulation PharmacologyDocument36 pagesAnticoagulation PharmacologyaymenNo ratings yet
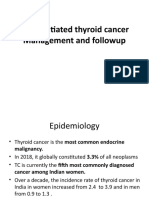
- Differentiated Thyroid CancerDocument61 pagesDifferentiated Thyroid CancerKNo ratings yet
- How To Write ThesisDocument22 pagesHow To Write ThesisKenneth LewisNo ratings yet
- Drugs Affecting Coagulation ObjectivesDocument14 pagesDrugs Affecting Coagulation ObjectiveslouradelNo ratings yet
- Adr ReportingDocument12 pagesAdr Reportinguss uusNo ratings yet
- Nursing Care Plan Impaired Urinary EliminationDocument1 pageNursing Care Plan Impaired Urinary Eliminationderic86% (14)
- Clostridium Difficile EpidemiologyDocument36 pagesClostridium Difficile EpidemiologyIsha BhattNo ratings yet
- John Jameson, Danny Bryden - Care of The Critically Ill Surgical Patient Student Handbook-The Royal College of Surgeons of England (2017)Document355 pagesJohn Jameson, Danny Bryden - Care of The Critically Ill Surgical Patient Student Handbook-The Royal College of Surgeons of England (2017)osamaeNo ratings yet
- Key Features of Rheumatoid ArthritisDocument42 pagesKey Features of Rheumatoid ArthritisNoman MunirNo ratings yet
- Itp 2021Document64 pagesItp 2021Victoria MalakNo ratings yet
- Therapeutic Drug Monitoring: T H e R A P e U T I C T o X I CDocument22 pagesTherapeutic Drug Monitoring: T H e R A P e U T I C T o X I Ckavya nainitaNo ratings yet
- DabigatranDocument25 pagesDabigatranNagesh JadavNo ratings yet
- Overview of Covid 19 Interventions v4.1.0Document6 pagesOverview of Covid 19 Interventions v4.1.0onibur@hotmail..comNo ratings yet
- DVT and PE: Understanding Venous ThromboembolismDocument40 pagesDVT and PE: Understanding Venous ThromboembolismShahab AlamNo ratings yet
- Farklin 1 2021 Ppds Fkunsri 16 JuliDocument134 pagesFarklin 1 2021 Ppds Fkunsri 16 JuliBayu WisnuNo ratings yet
- Damage Control Resuscitation in Patients With Severe Traumatic Hemorrhage A Practice Management Guideline From The Eastern Association For TheDocument11 pagesDamage Control Resuscitation in Patients With Severe Traumatic Hemorrhage A Practice Management Guideline From The Eastern Association For TheMadalina TalpauNo ratings yet
- Trastuzumab IV For HER2 Positive Breast CancersDocument4 pagesTrastuzumab IV For HER2 Positive Breast CancersEnrico GaharaNo ratings yet
- Polytrauma Jacques Duranteau PDFDocument48 pagesPolytrauma Jacques Duranteau PDFMarcelo MercadoNo ratings yet
- BRAJTR ProtocolDocument4 pagesBRAJTR ProtocolBangla SidNo ratings yet
- Bladder Cancer 6Document26 pagesBladder Cancer 6Awais AyubNo ratings yet
- Hip Fracture GuidelinesDocument10 pagesHip Fracture GuidelinesiamseraNo ratings yet
- TransfusionDocument3 pagesTransfusionjulissand10No ratings yet
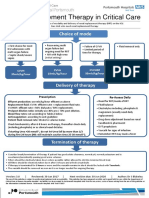
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Curriculum Vitae and Radiation Therapy for Gynecologic CancerDocument31 pagesCurriculum Vitae and Radiation Therapy for Gynecologic CancerpisangphoeNo ratings yet
- Lesson 42 Laboratory ValuesDocument4 pagesLesson 42 Laboratory ValuesDarren RossNo ratings yet
- Prostate CarcinomaDocument103 pagesProstate CarcinomaDrRajendra PatelNo ratings yet
- Salvage Therapy in Testicular Cancer (Hirao)Document1 pageSalvage Therapy in Testicular Cancer (Hirao)Taufik HidayatNo ratings yet
- Ijpr 123825Document12 pagesIjpr 123825personneNo ratings yet
- PDF Nursing Care PlanDocument16 pagesPDF Nursing Care PlanMichael MabiniNo ratings yet
- JP Journals 10071 23412Document5 pagesJP Journals 10071 23412Karina Dwi SwastikaNo ratings yet
- Response Evaluation of Cancer ChemotherapyDocument36 pagesResponse Evaluation of Cancer ChemotherapyRumah Sakit Bhakti NugrahaNo ratings yet
- Management of Nonperforated Appendicitis in AdultsDocument1 pageManagement of Nonperforated Appendicitis in Adultsjoaoduarte95No ratings yet
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModeJelena Obrenovic StankovicNo ratings yet
- Oncology Cheat Sheets -1 (1)Document5 pagesOncology Cheat Sheets -1 (1)abdallahmaurice94No ratings yet
- Management of Inpatient ChemotherapyDocument27 pagesManagement of Inpatient Chemotherapyapi-649066372No ratings yet
- CINVDocument23 pagesCINVHesham IbrahimNo ratings yet
- Benefit of Rituximab Maintenance Is Associated.7Document7 pagesBenefit of Rituximab Maintenance Is Associated.7ppdsipd2019No ratings yet
- Breast 1Document1 pageBreast 1Ramez AntakiaNo ratings yet
- BLEEDINGDocument5 pagesBLEEDINGKezia ImanuellaNo ratings yet
- CINV Guidelines PDFDocument8 pagesCINV Guidelines PDFagilNo ratings yet
- Ca Treatment Rectal Web AlgorithmDocument17 pagesCa Treatment Rectal Web AlgorithmPatrick JohnNo ratings yet
- Hormone Therapy For Prostate Cancer Guidelines Versus Clinical PracticeDocument7 pagesHormone Therapy For Prostate Cancer Guidelines Versus Clinical PracticeNenad MladenovicNo ratings yet
- Rivaroxaban Xarelto Requiring Emergency Surgery or Treatment For HaemorrhageDocument7 pagesRivaroxaban Xarelto Requiring Emergency Surgery or Treatment For HaemorrhageRomeo-Remus RaffaiNo ratings yet
- Rtog 0813 Marina CousinsDocument22 pagesRtog 0813 Marina Cousinsapi-426094285No ratings yet
- Multiple Myeloma: Is It Now A Curable Disease?: Pritesh Patel, MDDocument26 pagesMultiple Myeloma: Is It Now A Curable Disease?: Pritesh Patel, MDRabia AhmadNo ratings yet
- Adult Patients On Antiplatelet Therapy Who Require Elective Surgery or An Invasive Procedure Management of CA5127 V6Document5 pagesAdult Patients On Antiplatelet Therapy Who Require Elective Surgery or An Invasive Procedure Management of CA5127 V6adybutucNo ratings yet
- 0300060513485864Document11 pages0300060513485864Aashish KalikaNo ratings yet
- Bivalirudin Anticoagulant1Document6 pagesBivalirudin Anticoagulant1walid hassanNo ratings yet
- Renal Dialysis Unit Explains Therapeutic Plasma ExchangeDocument25 pagesRenal Dialysis Unit Explains Therapeutic Plasma ExchangeGi Mendez DimzonNo ratings yet
- UPDATED MalDocument52 pagesUPDATED MalABDIRAHIM ADAMNo ratings yet
- ANDROGEN DEPRIVATION THERAPY ENGLISH v6.02305843009217033820Document1 pageANDROGEN DEPRIVATION THERAPY ENGLISH v6.02305843009217033820Eduardo5671No ratings yet
- MILsgsdgdsVDocument4 pagesMILsgsdgdsVgarywall.ukNo ratings yet
- Webinanar Onko - JoglosemarDocument19 pagesWebinanar Onko - JoglosemarFerdinand SimanjuntakNo ratings yet
- 3 - Evaluation and Management of Rheumatoid ArthritisDocument56 pages3 - Evaluation and Management of Rheumatoid ArthritisDwi Astika SariNo ratings yet
- A Concise Guide to ITP Treatment and ManagementDocument16 pagesA Concise Guide to ITP Treatment and ManagementFein MalricNo ratings yet
- Testicular Tumors Part4Document52 pagesTesticular Tumors Part4Ramesh ReddyNo ratings yet
- Ash Itp Pocket Guide For Web 1204Document5 pagesAsh Itp Pocket Guide For Web 1204Restu Annisa PutriNo ratings yet
- Generic and Brand Drugs: Dosages, Mechanisms, Indications, Side Effects, Nursing ResponsibilitiesDocument4 pagesGeneric and Brand Drugs: Dosages, Mechanisms, Indications, Side Effects, Nursing Responsibilitiesbea pegadNo ratings yet
- Critical Appraisal Treatment: Emmanuel D. Margate, JRDocument21 pagesCritical Appraisal Treatment: Emmanuel D. Margate, JREmmanuel MargateNo ratings yet
- Laboratory Control of Anticoagulant Therapy TestsDocument69 pagesLaboratory Control of Anticoagulant Therapy TestsTusabe FredNo ratings yet
- Terapia Antiandrogenica A Acancerului de Prostata Rezistent La CastrareDocument1 pageTerapia Antiandrogenica A Acancerului de Prostata Rezistent La CastrareConstantin TataruNo ratings yet
- Breast Cancer - ETDocument21 pagesBreast Cancer - ETaprinaaaNo ratings yet
- Frontiers in Clinical Drug Research - Anti-Cancer Agents: Volume 5From EverandFrontiers in Clinical Drug Research - Anti-Cancer Agents: Volume 5No ratings yet
- OCTAPLEXDocument6 pagesOCTAPLEXNiken AmritaNo ratings yet
- Cancer Sarcoma Chemotherapy Regimen V2.1 May 2012Document75 pagesCancer Sarcoma Chemotherapy Regimen V2.1 May 2012Niken AmritaNo ratings yet
- CML and PregnancyDocument1 pageCML and PregnancyNiken AmritaNo ratings yet
- Hospitalizations and Testing in Gastroparesis: Journal ReadingDocument16 pagesHospitalizations and Testing in Gastroparesis: Journal ReadingNiken AmritaNo ratings yet
- Case Acutenecrotizing Coitis Due To AmebaDocument11 pagesCase Acutenecrotizing Coitis Due To AmebaNiken AmritaNo ratings yet
- DiphtheriaDocument13 pagesDiphtheriaNiken AmritaNo ratings yet
- MDR ThyphoidDocument4 pagesMDR ThyphoidNiken AmritaNo ratings yet
- MELD Outcome Cirrhosis and PregnantDocument8 pagesMELD Outcome Cirrhosis and PregnantNiken AmritaNo ratings yet
- Electrodiagnosisofcervical Radiculopathy: Kevin Hakimi,, David SpanierDocument12 pagesElectrodiagnosisofcervical Radiculopathy: Kevin Hakimi,, David Spanierkashif mansoorNo ratings yet
- Alleged starvation death of disabled child in Odisha villageDocument11 pagesAlleged starvation death of disabled child in Odisha villageBasudev MahapatraNo ratings yet
- Carolyn O'Neal v. Fremont County Board of Commissioners, Et Al.Document40 pagesCarolyn O'Neal v. Fremont County Board of Commissioners, Et Al.Michael_Lee_RobertsNo ratings yet
- Sex Hormone Synthesis, Regulation, and Function - McMaster Pathophysiology ReviewDocument7 pagesSex Hormone Synthesis, Regulation, and Function - McMaster Pathophysiology ReviewWahyu W'cas PamungkasNo ratings yet
- College of Nursing: Pharmacology Drug StudyDocument2 pagesCollege of Nursing: Pharmacology Drug StudyChristine Pialan SalimbagatNo ratings yet
- Jewish Standard, May 24, 2019Document48 pagesJewish Standard, May 24, 2019New Jersey Jewish StandardNo ratings yet
- Alexandra Plavsa FinalCVDocument2 pagesAlexandra Plavsa FinalCVAlex PlavsaNo ratings yet
- Taurine L Arginine ArrhythmiasDocument5 pagesTaurine L Arginine Arrhythmiasasd65433No ratings yet
- Making Dentistry Even Safer: Understanding The Proper Choice and Use of Emergency MedicationsDocument10 pagesMaking Dentistry Even Safer: Understanding The Proper Choice and Use of Emergency MedicationsMishellKarelisMorochoSegarraNo ratings yet
- MaternityDocument91 pagesMaternityAnonymous D8KswoNo ratings yet
- HospitalDocument116 pagesHospitalKhadija KamranNo ratings yet
- Gate Ee FinalDocument171 pagesGate Ee FinalAnonymous LXHlHv2RWNo ratings yet
- Rundown Kegiatan Pearls Makassar 2021: HARI 1, 23 OKTOBER 2021 WaktuDocument12 pagesRundown Kegiatan Pearls Makassar 2021: HARI 1, 23 OKTOBER 2021 WaktuangelicaNo ratings yet
- Dental Sealant ToxicityDocument14 pagesDental Sealant ToxicityGuru SvamiNo ratings yet
- Underlying The Mechanisms of Doxorubicin-InducedDocument11 pagesUnderlying The Mechanisms of Doxorubicin-InducedRania T. SabriNo ratings yet
- Transfusion Products: ImmunohematologyDocument12 pagesTransfusion Products: ImmunohematologyDiana Gabriela NinaNo ratings yet
- Bone TumorsDocument29 pagesBone TumorsmatameaNo ratings yet
- NCP RenalDocument22 pagesNCP Renalمحمود على ما تفرجNo ratings yet
- Effectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisDocument9 pagesEffectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisrebeca paulinoNo ratings yet
- Thesis Statement Examples On Childhood ObesityDocument8 pagesThesis Statement Examples On Childhood Obesityjaclyncreedonannarbor100% (2)