You might also like
- Partograph PPT 1Document55 pagesPartograph PPT 1Maria Lejani Terencio100% (1)
- Desertation in Obg RguhsDocument23 pagesDesertation in Obg RguhsVantrigaru Veeresh Bangi89% (44)
- BEmONC and CEmONCDocument3 pagesBEmONC and CEmONCGian Mauricio100% (2)
- Autonomic Dysreflexia Treatment AlgorithmDocument1 pageAutonomic Dysreflexia Treatment AlgorithmdandrewmNo ratings yet
- In-Vitro Fertilization (Ivf) : Step 1: Stimulation, Also Called Super OvulationDocument5 pagesIn-Vitro Fertilization (Ivf) : Step 1: Stimulation, Also Called Super Ovulationpriyanka100% (1)
- Management of Normal Labour ChartDocument1 pageManagement of Normal Labour ChartwedishaNo ratings yet
- Still: Consider Pai BleedingDocument15 pagesStill: Consider Pai Bleedingشريف محمد حسين شريف يوسفNo ratings yet
- Diagnostic Assessment Outline NotesDocument15 pagesDiagnostic Assessment Outline Notesyhfyhkcxb9No ratings yet
- Emergency Drugs-1Document13 pagesEmergency Drugs-1Pratik DeshmukhNo ratings yet
- Dams 1 General PhysiologyDocument44 pagesDams 1 General PhysiologyEvil QTNo ratings yet
- PDocument1 pagePbryan.zabala.mnlNo ratings yet
- CI4402 - 20200319 - PizarraDocument4 pagesCI4402 - 20200319 - PizarrajavierNo ratings yet
- Curs s3 1 + 2Document5 pagesCurs s3 1 + 2Zanoschi AdrianNo ratings yet
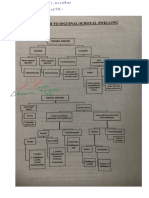
- Inguinal Scrotal Swelling + Pe HerniaDocument8 pagesInguinal Scrotal Swelling + Pe Herniaiman khaiNo ratings yet
- Urinary - Part#2Document10 pagesUrinary - Part#2Farah AljayyousiNo ratings yet
- 3 Normal LaborDocument101 pages3 Normal Laborfpnn56xyyvNo ratings yet
- OBG (Gynecology)Document229 pagesOBG (Gynecology)abhishekrajpurohit275No ratings yet
- Latch ScoreDocument1 pageLatch ScoreAnnie LijinNo ratings yet
- Img 0527Document2 pagesImg 0527Beatrice KoesmarsonoNo ratings yet
- Note 24 Mar 2021 11 - 14 - 58 PMDocument4 pagesNote 24 Mar 2021 11 - 14 - 58 PMibraNo ratings yet
- Fetal and Neonatal Death Rate - GROUP 2 (Garbosa, Garzon, Gascon, Geralo, Gonzaga, Gubtanga, Guerra, Guillergan, Guino-O)Document19 pagesFetal and Neonatal Death Rate - GROUP 2 (Garbosa, Garzon, Gascon, Geralo, Gonzaga, Gubtanga, Guerra, Guillergan, Guino-O)Rej GarbosaNo ratings yet
- Apma 0350 Cheat SheetDocument2 pagesApma 0350 Cheat SheethengabNo ratings yet
- By F.R.C.S., Surgeon Royal Infirmary, Consulting Surgeon Hospital, TyneDocument19 pagesBy F.R.C.S., Surgeon Royal Infirmary, Consulting Surgeon Hospital, Tynenao thaNo ratings yet
- 4) CVS Star Rated Questions - 7dcb9517 f817 46ef b4f4 5aa2434ffbc5Document3 pages4) CVS Star Rated Questions - 7dcb9517 f817 46ef b4f4 5aa2434ffbc5ShivNo ratings yet
- Physio RR NotesDocument123 pagesPhysio RR NoteshamarebehNo ratings yet
- Lec 12. Pulp TherapyDocument65 pagesLec 12. Pulp Therapygali3033No ratings yet
- ShockDocument3 pagesShockmiracleNo ratings yet
- Antihistamines 2019 14 - 08 - 02Document9 pagesAntihistamines 2019 14 - 08 - 02Alexandra AlexaNo ratings yet
- Block E 2020 Kmu AnnualDocument6 pagesBlock E 2020 Kmu Annualmuhammadshayan416No ratings yet
- Ass 12Document3 pagesAss 12bharath bodduNo ratings yet
- Utkast Grona Boken 2Document2 pagesUtkast Grona Boken 2maria lukNo ratings yet
- JaundiceDocument30 pagesJaundiceVasudeva LamNo ratings yet
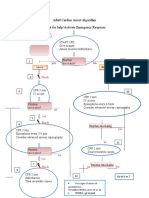
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocument1 pageAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMNo ratings yet
- Management of PPHDocument1 pageManagement of PPH098 U.KARTHIK SARAVANA KANTHNo ratings yet
- Chapter 3, Unit 3, Pharmaceutical Analysis, B Pharmacy 1st Sem, Carewell PharmaDocument7 pagesChapter 3, Unit 3, Pharmaceutical Analysis, B Pharmacy 1st Sem, Carewell Pharmavenkat ramanaNo ratings yet
- Digital Notes On Funda 2Document51 pagesDigital Notes On Funda 2Enna EstrellaNo ratings yet
- Drug Study: (Oxytocin)Document10 pagesDrug Study: (Oxytocin)Shara Lailanie A. AzisNo ratings yet
- Ucc Day 2-1Document181 pagesUcc Day 2-1Griffin HankNo ratings yet
- VEAL CHOP With Interventions and OutcomesDocument1 pageVEAL CHOP With Interventions and Outcomesayngn13No ratings yet
- 3rd AnswerDocument2 pages3rd Answermr.mandy3No ratings yet
- Trauma SurgeryDocument69 pagesTrauma SurgeryKumar ShivamNo ratings yet
- Testicular Torsion, Peds Cases NotesDocument1 pageTesticular Torsion, Peds Cases NotesdzalhcNo ratings yet
- Oxytocin Drug StudyDocument2 pagesOxytocin Drug StudyRem remNo ratings yet
- Oxytocin Drug StudyDocument1 pageOxytocin Drug Studysweetpixie1887% (15)
- Reproductive Health Mind MapDocument3 pagesReproductive Health Mind MapAkash Yadav100% (1)
- Pelvic FractureDocument27 pagesPelvic FractureElhamNo ratings yet
- Chapter 14 Maths 11.classDocument9 pagesChapter 14 Maths 11.classPramersh LagwalNo ratings yet
- Trans-Out Orders: NSVD Admitting Notes Postpartum OrdersDocument7 pagesTrans-Out Orders: NSVD Admitting Notes Postpartum OrdersDre ValdezNo ratings yet
- NCP On Postpartum MotherDocument13 pagesNCP On Postpartum MotherLenjun89% (57)
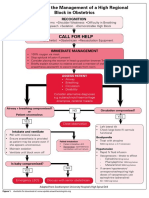
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- AlgorithmNeonatal Resuscitation 200615Document1 pageAlgorithmNeonatal Resuscitation 200615Ratna TambaNo ratings yet
- AlgorithmNeonatal Resuscitation 200615Document1 pageAlgorithmNeonatal Resuscitation 200615Atley TroyerNo ratings yet
- AlgorithmNeonatal Resuscitation 200615Document1 pageAlgorithmNeonatal Resuscitation 200615Ratna TambaNo ratings yet
- AlgorithmNeonatal Resuscitation 200615Document1 pageAlgorithmNeonatal Resuscitation 200615Amir NaghshzanNo ratings yet
- Anesthesia - RR Jan2023Document61 pagesAnesthesia - RR Jan2023Rohit DagarNo ratings yet
- Ipm GiDocument7 pagesIpm GiFritzienico BaskoroNo ratings yet
- Adult Cardiac Arrest AlgoritmaDocument1 pageAdult Cardiac Arrest AlgoritmaYouniehacibie Ichisky ChildNo ratings yet
- Lipid Profile Normal Values Cardiac Enzyme Normal Values: ECG ChangesDocument3 pagesLipid Profile Normal Values Cardiac Enzyme Normal Values: ECG Changesairnyn_manzo08No ratings yet
- Active Management of 3rd Stage LabourDocument3 pagesActive Management of 3rd Stage Labourrailabhi83No ratings yet
- OBSTETRIC II Course OutlineDocument7 pagesOBSTETRIC II Course Outlineabduse midwifNo ratings yet
- Research - Large For Gestational AgeDocument3 pagesResearch - Large For Gestational AgearizzadyetaNo ratings yet
- Rhesus ObgynDocument44 pagesRhesus Obgynpatboothe1880No ratings yet
- 10 - 15 - Infectia Cailor Urinare La Gravide.Document6 pages10 - 15 - Infectia Cailor Urinare La Gravide.MihaiNo ratings yet
- Obstetric Nursing RevisedDocument345 pagesObstetric Nursing Revisedkarendelarosa06100% (1)
- Pregnancy Simulation Scenario StudentDocument3 pagesPregnancy Simulation Scenario StudentmarieNo ratings yet
- REMS Obgyn Shelf Notes Dec 2021Document53 pagesREMS Obgyn Shelf Notes Dec 2021Swarna BanikNo ratings yet
- Placenta PreviaDocument4 pagesPlacenta PreviaJeizel IgnacioNo ratings yet
- Maternal, Child and Adolescent Health Services: Lawrence Ryan A. Daug, RN, MPM CHN 1 - InstructorDocument32 pagesMaternal, Child and Adolescent Health Services: Lawrence Ryan A. Daug, RN, MPM CHN 1 - InstructorLawrence Ryan DaugNo ratings yet
- Research Paper For AbortionDocument10 pagesResearch Paper For AbortionMarevisha Vidfather75% (4)
- HBN 09-02 FinalDocument82 pagesHBN 09-02 FinalDharani NachiyarNo ratings yet
- National Health Situation of Maternal and Child Health NursingDocument11 pagesNational Health Situation of Maternal and Child Health NursingNiña Ricci MtflcoNo ratings yet
- Practice Bulletin: Cerclage For The Management of Cervical InsufficiencyDocument8 pagesPractice Bulletin: Cerclage For The Management of Cervical InsufficiencyCarlos Rasmijn100% (1)
- Ultrasound Report The Black Box of Fetal StatusDocument43 pagesUltrasound Report The Black Box of Fetal StatusKalpavriksha19740% (1)
- Lamaze Early Labor InfographicDocument1 pageLamaze Early Labor Infographicionela stoicaNo ratings yet
- BWPA 2020 Survey ReportDocument22 pagesBWPA 2020 Survey ReportjmicekNo ratings yet
- A Reaction Paper About AftershockDocument1 pageA Reaction Paper About AftershockAlexa VeraNo ratings yet
- Oligohydramnios 171125104430Document27 pagesOligohydramnios 171125104430manjuNo ratings yet
- Prenatal Care - TransDocument3 pagesPrenatal Care - TransSean RodriguezNo ratings yet
- Cord Presentation and ProlapseDocument7 pagesCord Presentation and ProlapseIsrael WoseneNo ratings yet
- History-Taking & Physical Examination by DR Samer Abu EidehDocument48 pagesHistory-Taking & Physical Examination by DR Samer Abu EidehAbdullah MatarNo ratings yet
- Placental AbnormalitiesDocument5 pagesPlacental AbnormalitiesNica Lopez FernandezNo ratings yet
- Health Education For Record BookDocument24 pagesHealth Education For Record BookRoselineTiggaNo ratings yet
- Prematurely Ruptured of Membranes (PROM)Document23 pagesPrematurely Ruptured of Membranes (PROM)NiNie Sie MbakayuNeNo ratings yet
- Breech Presentation Delivery CareDocument12 pagesBreech Presentation Delivery CareFatmaNo ratings yet
- Ashrafian, Hutan Sunzi Surgical Philosophy Concepts of Modern Surgery Paralleled To Sun Tzus Art of WarDocument4 pagesAshrafian, Hutan Sunzi Surgical Philosophy Concepts of Modern Surgery Paralleled To Sun Tzus Art of WarWilliam AdiputraNo ratings yet