You might also like
- Chemotherapy and Renal Andhepatic Insufficiency 2008Document24 pagesChemotherapy and Renal Andhepatic Insufficiency 2008Vika RatuNo ratings yet
- Drug Induced Kidney DeseaseDocument12 pagesDrug Induced Kidney DeseaseNurul MasyithahNo ratings yet
- Drug Induced NephrotoxicityDocument13 pagesDrug Induced NephrotoxicityAgnes BastonNo ratings yet
- Drug Induced Kidney DiseaseDocument12 pagesDrug Induced Kidney DiseaseTusharNo ratings yet
- Drug Induced Liver DiseaseDocument35 pagesDrug Induced Liver DiseaseKris Sharine Batalla OderoNo ratings yet
- Which Psychotropic Medications Induce He PDFDocument9 pagesWhich Psychotropic Medications Induce He PDFnisastNo ratings yet
- Drugs and Kidney DiseasesDocument46 pagesDrugs and Kidney Diseasesمرتضى محمد فاضل جرجوكNo ratings yet
- Chandok Et Al, 2010Document8 pagesChandok Et Al, 2010Cika Zahrah DewisoniaNo ratings yet
- Review: Hepatocellular Damage From Non-Steroidal Anti-Inflammatory DrugsDocument5 pagesReview: Hepatocellular Damage From Non-Steroidal Anti-Inflammatory Drugsshessy-jolycia-kerrora-3047No ratings yet
- Drug-Induced Nephrotoxicity: Cynthia A. Naughton, Pharmd, BCPS, North Dakota State University College of PharmacyDocument8 pagesDrug-Induced Nephrotoxicity: Cynthia A. Naughton, Pharmd, BCPS, North Dakota State University College of PharmacyAbdur Rachman Ba'abdullahNo ratings yet
- Drug-Induced Liver Disease.Document16 pagesDrug-Induced Liver Disease.Dr. Ammar Khalil100% (1)
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaDocument36 pagesATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Drug Induced Kidney Disease: Dr. Hamid SaeedDocument42 pagesDrug Induced Kidney Disease: Dr. Hamid SaeedKhadija KamranNo ratings yet
- Acute Kidney Injury: Prerenal Azotemia, Intrinsic Renal Parenchymal Disease, and Postrenal ObstructionDocument11 pagesAcute Kidney Injury: Prerenal Azotemia, Intrinsic Renal Parenchymal Disease, and Postrenal Obstructionnathan asfahaNo ratings yet
- Acute On Chronic Kidney DiseaseDocument6 pagesAcute On Chronic Kidney DiseaseElizabeth LieNo ratings yet
- Review of nephrotic syndrome managementDocument7 pagesReview of nephrotic syndrome managementGarit Hapsari KiranaNo ratings yet
- Drug-Induced Nephrotoxicity: A Review of Risk Factors and BiomarkersDocument9 pagesDrug-Induced Nephrotoxicity: A Review of Risk Factors and BiomarkersCecep Darwis MuttaqinNo ratings yet
- Nephrotoxic DrugsDocument8 pagesNephrotoxic DrugsAhmad Radhya DionandaNo ratings yet
- Drug Induced NephrotoxicityDocument15 pagesDrug Induced NephrotoxicityMUGHALNo ratings yet
- Manifestations of and Risk Factors For Aminoglycoside Nephrotoxicity - UpToDateDocument8 pagesManifestations of and Risk Factors For Aminoglycoside Nephrotoxicity - UpToDateMARTINA MARIA INSUA CASTRONo ratings yet
- Understanding Diabetic Nephropathy and Herbal TreatmentsDocument30 pagesUnderstanding Diabetic Nephropathy and Herbal TreatmentsBhoj RajNo ratings yet
- Acut Hepatic FailureDocument11 pagesAcut Hepatic FailureDennis CobbNo ratings yet
- Anaesthesia For Patients With Liver DiseaseDocument5 pagesAnaesthesia For Patients With Liver DiseaseRitu BhandariNo ratings yet
- Drug Induced Liver Diseases in The Elderly: Chandy GM, Chandy RGDocument4 pagesDrug Induced Liver Diseases in The Elderly: Chandy GM, Chandy RGkazekiraNo ratings yet
- Drug Induced Liver DisordersDocument31 pagesDrug Induced Liver DisordersJason fernandes jNo ratings yet
- ABC Acute Renal FailureDocument5 pagesABC Acute Renal FailureAngela CristinoNo ratings yet
- Renal Failure in Burn Patients ReviewedDocument4 pagesRenal Failure in Burn Patients ReviewedbrianNo ratings yet
- Drug Induced LiverDocument8 pagesDrug Induced LiverDita IndahNo ratings yet
- Chronic Kidney Disease in HIV Positive PatientsDocument22 pagesChronic Kidney Disease in HIV Positive PatientsAdityaNo ratings yet
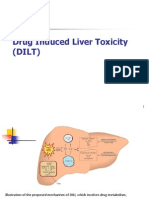
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- A Primer For The Primary Care Physician.: Drug Management in The Elderly Adult With Chronic Kidney DiseaseDocument33 pagesA Primer For The Primary Care Physician.: Drug Management in The Elderly Adult With Chronic Kidney Diseaseyuliana160793No ratings yet
- CKD Stages, Risks, and PathophysiologyDocument30 pagesCKD Stages, Risks, and Pathophysiologynathan asfahaNo ratings yet
- DR - Mukesh Dassani Synopsis 20 SepDocument20 pagesDR - Mukesh Dassani Synopsis 20 SepMukesh DassaniNo ratings yet
- CKD UnsoedDocument42 pagesCKD UnsoedSutan Malik IbrahimNo ratings yet
- Acute Renal Failure DXDocument7 pagesAcute Renal Failure DXfarid akbarNo ratings yet
- Chapter 31 - Anesthesia For Patients With Kidney DiseaseDocument21 pagesChapter 31 - Anesthesia For Patients With Kidney DiseasefewNo ratings yet
- Drug-Induced Kidney Disease: ArticleDocument11 pagesDrug-Induced Kidney Disease: Articledwi harisNo ratings yet
- Aki 6Document12 pagesAki 6WindaNo ratings yet
- Acute On ChronicDocument4 pagesAcute On ChronicrendyoscaNo ratings yet
- Drug Prescription in CKD and DialysisDocument24 pagesDrug Prescription in CKD and DialysisAnitha SNo ratings yet
- Drug Induced Liver InjuryDocument13 pagesDrug Induced Liver InjuryIhsan PutraNo ratings yet
- Prescribing in Patients With Liver Disease: Rakesh K TandonDocument4 pagesPrescribing in Patients With Liver Disease: Rakesh K Tandonjoydeep chakrabortyNo ratings yet
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaNo ratings yet
- Cirrhosis Alcoholic Liver DiseaseDocument10 pagesCirrhosis Alcoholic Liver DiseaseSarah ZiaNo ratings yet
- Jurnal Pendukung Proposal 9Document4 pagesJurnal Pendukung Proposal 9Munawwar AweNo ratings yet
- Welcome To Journal Club Presentation: Presented byDocument54 pagesWelcome To Journal Club Presentation: Presented byneptorNo ratings yet
- For Practitioner: Tuberculosis and Chronic Renal Failure Therapy PatternsDocument3 pagesFor Practitioner: Tuberculosis and Chronic Renal Failure Therapy PatternsAnastasia Lilian SuryajayaNo ratings yet
- ASHP Chapter 29 - Medication Dosing in Patients With Renal DysfunctionDocument5 pagesASHP Chapter 29 - Medication Dosing in Patients With Renal DysfunctionTammyNo ratings yet
- Nephrotic Syndrome 5th Year Lecture 2011Document7 pagesNephrotic Syndrome 5th Year Lecture 2011Gutierrez MarinellNo ratings yet
- Risk Factors and Management of Acute Kidney Injury in the ElderlyDocument15 pagesRisk Factors and Management of Acute Kidney Injury in the ElderlySiti NcitNo ratings yet
- Agranulocytosis An Adverse Effect of Allopurinol TDocument4 pagesAgranulocytosis An Adverse Effect of Allopurinol TSYARIF HIDAYATULLAHNo ratings yet
- G6PD Deficiency RBC Hemolysis from TMP-SMXDocument63 pagesG6PD Deficiency RBC Hemolysis from TMP-SMXAppu ayyala100% (2)
- Drugs & KidneyDocument18 pagesDrugs & KidneyAamir MohammadNo ratings yet
- First do no harmDocument21 pagesFirst do no harmPHARMACY 2021No ratings yet
- The Use of Albumin For The Prevention of Hepatorenal Syndrome in Patients With Spontaneous Bacterial Peritonitis and CirrhosisDocument14 pagesThe Use of Albumin For The Prevention of Hepatorenal Syndrome in Patients With Spontaneous Bacterial Peritonitis and CirrhosisPaulus MetehNo ratings yet
- GinjalDocument11 pagesGinjalOneng IfayaniNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Psychiatric Aspects of Medical IllnessDocument52 pagesPsychiatric Aspects of Medical IllnessPIH SHTNo ratings yet
- Obsessive Compulsive DisorderDocument26 pagesObsessive Compulsive DisorderPIH SHTNo ratings yet
- L2 Mcqs On Classification of AAs AnsweredDocument3 pagesL2 Mcqs On Classification of AAs AnsweredPIH SHTNo ratings yet
- Posttraumatic Stress Disorder and Acute Stress DisorderDocument42 pagesPosttraumatic Stress Disorder and Acute Stress DisorderPIH SHTNo ratings yet
- L1 McqsDocument5 pagesL1 McqsPIH SHTNo ratings yet
- L2 McqsDocument8 pagesL2 McqsPIH SHTNo ratings yet
- Carbohydrate MetabolismDocument15 pagesCarbohydrate MetabolismPIH SHTNo ratings yet
- Glycine & Serine NUB (IHB)Document4 pagesGlycine & Serine NUB (IHB)PIH SHTNo ratings yet
- L1 McqsDocument5 pagesL1 McqsPIH SHTNo ratings yet
- L1-Introduction To Human Physiology-2Document9 pagesL1-Introduction To Human Physiology-2PIH SHTNo ratings yet
- Glycine & Serine NUB (IHB)Document4 pagesGlycine & Serine NUB (IHB)PIH SHTNo ratings yet
- General Protein Metabolism NUB Full 2022Document11 pagesGeneral Protein Metabolism NUB Full 2022PIH SHTNo ratings yet
- L2 McqsDocument8 pagesL2 McqsPIH SHTNo ratings yet
- Eicosanoids Handout NUBDocument4 pagesEicosanoids Handout NUBPIH SHTNo ratings yet
- L1 Mcqs AnsweredDocument7 pagesL1 Mcqs AnsweredPIH SHTNo ratings yet
- L1-Introduction To Human Physiology-2Document9 pagesL1-Introduction To Human Physiology-2PIH SHTNo ratings yet
- L1 Mcqs AnsweredDocument7 pagesL1 Mcqs AnsweredPIH SHTNo ratings yet
- Human Factors (Topic 2)Document37 pagesHuman Factors (Topic 2)PIH SHTNo ratings yet
- L2 McqsDocument8 pagesL2 McqsPIH SHTNo ratings yet
- Binder 1Document1 pageBinder 1PIH SHTNo ratings yet
- L1-Introduction To Human Physiology-2Document9 pagesL1-Introduction To Human Physiology-2PIH SHTNo ratings yet
- General Protein Metabolism NUB Full 2022Document11 pagesGeneral Protein Metabolism NUB Full 2022PIH SHTNo ratings yet
- INFERTILITYDocument4 pagesINFERTILITYPIH SHTNo ratings yet
- Lipid Chemistery Hand Out FinalDocument12 pagesLipid Chemistery Hand Out FinalPIH SHTNo ratings yet
- INFERTILITYDocument4 pagesINFERTILITYPIH SHTNo ratings yet
- Ketone Bodies MetabolismDocument7 pagesKetone Bodies MetabolismPIH SHTNo ratings yet
- Management of Obstetric Emergencies: Hypertension and HemorrhageDocument66 pagesManagement of Obstetric Emergencies: Hypertension and Hemorrhageputri azzahraNo ratings yet
- jhmbf01562 Sup 0001Document10 pagesjhmbf01562 Sup 0001niva annantsNo ratings yet
- Journal Heptojugular RefluxDocument5 pagesJournal Heptojugular RefluxFarhan RezaNo ratings yet
- Desain GordingDocument17 pagesDesain GordingIrfan Gơlden BơyNo ratings yet
- Cardio ReviewDocument25 pagesCardio ReviewHarini PrayagaNo ratings yet
- Topic Respiratory Distress in NewbornDocument45 pagesTopic Respiratory Distress in NewbornICETNPNo ratings yet
- Histology of the Urinary SystemDocument48 pagesHistology of the Urinary SystemNel TinduganiNo ratings yet
- Pretreatment Medications For Rapid Sequence Intubation in Adults For Emergency Medicine and Critical Care - UpToDateDocument19 pagesPretreatment Medications For Rapid Sequence Intubation in Adults For Emergency Medicine and Critical Care - UpToDateignacia.conejerosNo ratings yet
- Myxedema Coma NCLEX ReviewDocument4 pagesMyxedema Coma NCLEX ReviewhaleyNo ratings yet
- Medical ReportDocument4 pagesMedical Reportdriddle36No ratings yet
- WR - Senior Paeds Notes 2nd Ed UPDATED JAN 2019 - Anggelos EditDocument223 pagesWR - Senior Paeds Notes 2nd Ed UPDATED JAN 2019 - Anggelos Editdale 99No ratings yet
- Case Study of Congestive Heart FailureDocument74 pagesCase Study of Congestive Heart FailureAnonymous XvwKtnSrMR93% (27)
- Building Your Peripheral Artery Disease Toolkit MDocument11 pagesBuilding Your Peripheral Artery Disease Toolkit MehaffejeeNo ratings yet
- Acute Biologic Crisis-ArDocument71 pagesAcute Biologic Crisis-ArJayvee Novenario CasaljayNo ratings yet
- Download ebook Atlas Of Endovascular Venous Surgery Pdf full chapter pdfDocument67 pagesDownload ebook Atlas Of Endovascular Venous Surgery Pdf full chapter pdfjeremy.gainey785100% (24)
- Technological Assessment and Objective Evaluation of Minimally Invasive and Noninvasive Cardiac Output Monitoring SystemsDocument8 pagesTechnological Assessment and Objective Evaluation of Minimally Invasive and Noninvasive Cardiac Output Monitoring Systemsnvidia coreNo ratings yet
- Download ebook Diagnostic Imaging Chest 2 full chapter pdfDocument47 pagesDownload ebook Diagnostic Imaging Chest 2 full chapter pdfjade.burrow118100% (22)
- Nurseslabs Cram SheetDocument17 pagesNurseslabs Cram SheetCris GalendezNo ratings yet
- Heart Anatomy 3DDocument9 pagesHeart Anatomy 3DMaram RanadeepNo ratings yet
- Diabetes Ferri 2019Document12 pagesDiabetes Ferri 2019cochipinkNo ratings yet
- Guideline Reading Diagnosis and Management of Pericardial DiseaseDocument87 pagesGuideline Reading Diagnosis and Management of Pericardial DiseaseMirza AlfiansyahNo ratings yet
- Annals of Medicine and Surgery: Sara Bouabdella, Soraya Aouali, Hanan Ragragui, Nada Zizi, Siham DikhayeDocument3 pagesAnnals of Medicine and Surgery: Sara Bouabdella, Soraya Aouali, Hanan Ragragui, Nada Zizi, Siham DikhayeGeysel SuarezNo ratings yet
- Pulmonary EmbolismDocument21 pagesPulmonary EmbolismMadhu Bala100% (2)
- DAIBETESDocument23 pagesDAIBETESAditya MahakalNo ratings yet
- Krok 2 Medicine (EN)_ Attempt review 5Document19 pagesKrok 2 Medicine (EN)_ Attempt review 5IS ZDNo ratings yet
- Warfarin's mechanism of action and indicationsDocument4 pagesWarfarin's mechanism of action and indicationsAmir mohammad moori MohammadiNo ratings yet
- Sicksinussyndrome: Roberto de Ponti,, Jacopo Marazzato,, Giuseppe Bagliani,, Fabio M. Leonelli,, Luigi PadelettiDocument13 pagesSicksinussyndrome: Roberto de Ponti,, Jacopo Marazzato,, Giuseppe Bagliani,, Fabio M. Leonelli,, Luigi Padelettijose noel garcia perezNo ratings yet
- Arab Board 2017 Internal MedicineDocument37 pagesArab Board 2017 Internal MedicineAFAQ MAMMEDZADENo ratings yet
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
- Krok 2- 2013מסומן (General Medicine)Document26 pagesKrok 2- 2013מסומן (General Medicine)Nicole VinnikNo ratings yet