You might also like
- Approach to Patients with CytopeniasDocument48 pagesApproach to Patients with CytopeniasYabetsNo ratings yet
- Genetic Diagnosis of Endocrine DisordersFrom EverandGenetic Diagnosis of Endocrine DisordersRoy E. WeissNo ratings yet
- Idiosyncrasy: Idiosyncratic ReactionsDocument38 pagesIdiosyncrasy: Idiosyncratic Reactionsfaisalnadeem100% (1)
- DIBDDocument11 pagesDIBDKabirNo ratings yet
- Manual of Pediatric Hematology and OncologyFrom EverandManual of Pediatric Hematology and OncologyRating: 4 out of 5 stars4/5 (5)
- Drug Induced NephrotoxicityDocument15 pagesDrug Induced NephrotoxicityMUGHALNo ratings yet
- Non-Parkinsonian Movement DisordersFrom EverandNon-Parkinsonian Movement DisordersDeborah A. HallNo ratings yet
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- Toxic Responses of The BloodDocument10 pagesToxic Responses of The BloodM. Joyce100% (2)
- Drug Induced DiseasesDocument4 pagesDrug Induced DiseasesMahewash PathanNo ratings yet
- Drug Induced Liver DiseaseDocument35 pagesDrug Induced Liver DiseaseKris Sharine Batalla OderoNo ratings yet
- Drugs Induce Hematologic DisordersDocument3 pagesDrugs Induce Hematologic DisorderspaymanmatinNo ratings yet
- Drug Induced DiseasesDocument8 pagesDrug Induced DiseasesB.pharm 16th BatchNo ratings yet
- Common Causes of Delirium and Confusional StatesDocument4 pagesCommon Causes of Delirium and Confusional StatesAnonymous ZUaUz1wwNo ratings yet
- AKI DrugsDocument4 pagesAKI DrugsPIH SHTNo ratings yet
- Acute KidneyDocument50 pagesAcute Kidneyme.lakshay077No ratings yet
- Emergencias TiroideasDocument19 pagesEmergencias Tiroideasmireya nuñezNo ratings yet
- Drugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDocument4 pagesDrugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDejan OgnjanovicNo ratings yet
- Obat-Obat NefrotoksikDocument43 pagesObat-Obat Nefrotoksiknursidiq10100% (1)
- Toxicidades Asociadas A QuimioterapiaDocument46 pagesToxicidades Asociadas A QuimioterapiaAldo LealNo ratings yet
- AnemiaDocument51 pagesAnemiaAravind A SNo ratings yet
- Drug induced diseases: An overviewDocument5 pagesDrug induced diseases: An overviewraisul razaNo ratings yet
- Bone Marrow Failure 2008-09Document15 pagesBone Marrow Failure 2008-09Karan BhattNo ratings yet
- Curs Ia. Anemia AplasticaDocument10 pagesCurs Ia. Anemia Aplasticaalina2009No ratings yet
- Drug Study - HRZEDocument4 pagesDrug Study - HRZEEunice Ordonez67% (3)
- HematologyDocument444 pagesHematologyalnote.1.docNo ratings yet
- Hafizuddin Mohamed Fauzi P-UM0037/10Document54 pagesHafizuddin Mohamed Fauzi P-UM0037/10Hafizuddin Mohamed FauziNo ratings yet
- Czarina Drug Study JuneDocument20 pagesCzarina Drug Study JuneNicoh AvilaNo ratings yet
- Drugs & KidneyDocument18 pagesDrugs & KidneyAamir MohammadNo ratings yet
- CH 46 Antineoplastic Drugs Part 2Document7 pagesCH 46 Antineoplastic Drugs Part 2Taleisha CoppedgeNo ratings yet
- Clinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsDocument26 pagesClinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsNadia Ancharuz100% (1)
- ADRsDocument54 pagesADRsraffia mahakNo ratings yet
- PRESENTED:-Dr. Raju NiraulaDocument29 pagesPRESENTED:-Dr. Raju NiraulaRaju NiraulaNo ratings yet
- Drug Induced Hematologic and Organ DisordersDocument19 pagesDrug Induced Hematologic and Organ DisordersMisgi Candra DasaNo ratings yet
- ADE & Factors Affecting Drug Response 2016 Draft 1Document45 pagesADE & Factors Affecting Drug Response 2016 Draft 1احمد علىNo ratings yet
- Toxic Effect of DrugDocument8 pagesToxic Effect of DrugFrances Lau Yee ChinNo ratings yet
- Haematology LastDocument65 pagesHaematology LastficocNo ratings yet
- Drug Induced LupusDocument4 pagesDrug Induced LupusRohaniNo ratings yet
- Antirheumatic and Antigout DrugsDocument66 pagesAntirheumatic and Antigout DrugsBadri KarkiNo ratings yet
- Pharmacology II: Treatments for Blood Disorders and InflammationDocument61 pagesPharmacology II: Treatments for Blood Disorders and InflammationDiane BanuaNo ratings yet
- Causes of Acute Renal FailureDocument11 pagesCauses of Acute Renal FailureAndrea Roman chavezNo ratings yet
- Causes, Symptoms and Treatment of Aplastic AnemiaDocument34 pagesCauses, Symptoms and Treatment of Aplastic AnemiaKhadar mohamedNo ratings yet
- Antituberculosis Treatment Hepatotoxicity MechanismsDocument6 pagesAntituberculosis Treatment Hepatotoxicity Mechanismsadilah fazliNo ratings yet
- Drug Induced Liver Diseases (DILD) : M. DeepalakshmiDocument22 pagesDrug Induced Liver Diseases (DILD) : M. DeepalakshmicrissNo ratings yet
- Adverse ReactionsDocument1 pageAdverse ReactionsChrissieNo ratings yet
- SEMINAR ON HYPERTENSIVE EMERGENCIES AND URGENT TREATMENTDocument7 pagesSEMINAR ON HYPERTENSIVE EMERGENCIES AND URGENT TREATMENTGede AdiNo ratings yet
- Chemotherapy and Renal Andhepatic Insufficiency 2008Document24 pagesChemotherapy and Renal Andhepatic Insufficiency 2008Vika RatuNo ratings yet
- K12 - Pharmacology of Anticancer-NEW-1Document114 pagesK12 - Pharmacology of Anticancer-NEW-1Josephine IrenaNo ratings yet
- CBC 150106153749 Conversion Gate02Document44 pagesCBC 150106153749 Conversion Gate02KhetanNo ratings yet
- Understanding Adverse Drug ReactionsDocument614 pagesUnderstanding Adverse Drug Reactionsela fania100% (1)
- Ojim 2016091213324550Document10 pagesOjim 2016091213324550rianmg21No ratings yet
- Drug EruptionsDocument11 pagesDrug EruptionsAchmad Hariyanto100% (1)
- Nephrotoxic DrugsDocument43 pagesNephrotoxic DrugsAnnisa Mulyandini100% (1)
- Aplastic Anemia: Review of Etiology and TreatmentDocument7 pagesAplastic Anemia: Review of Etiology and TreatmentCleber MaiaNo ratings yet
- Drug Induced Liver Toxicity (DILT): Mechanisms, Classifications and SpectrumDocument39 pagesDrug Induced Liver Toxicity (DILT): Mechanisms, Classifications and SpectrumAjeng SekariniNo ratings yet
- Causes and Management of ThrombocytopeniaDocument25 pagesCauses and Management of ThrombocytopeniaAbdul Gafoor CPNo ratings yet
- Drug Induced Kidney DeseaseDocument12 pagesDrug Induced Kidney DeseaseNurul MasyithahNo ratings yet
- Crash Course Crash Course: Niper-2021Document7 pagesCrash Course Crash Course: Niper-2021ramesh joshiNo ratings yet
- Call For PapersDocument1 pageCall For PapersLovely Ann AyapanaNo ratings yet
- Antiplatelet and Anticoagulation GuideDocument31 pagesAntiplatelet and Anticoagulation GuideMarcelliaNo ratings yet
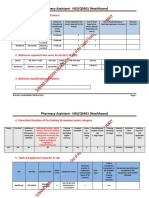
- Pharmacy Assistant-HSS/Q5401 (Healthcare) : 1. Minimum Qualification For TrainersDocument7 pagesPharmacy Assistant-HSS/Q5401 (Healthcare) : 1. Minimum Qualification For TrainersBabar AliNo ratings yet
- Sanofi AventisDocument18 pagesSanofi AventisNavedNo ratings yet
- Cell-Based Model of CoagulationDocument8 pagesCell-Based Model of CoagulationIULIU-CONSTANTIN MOCANUNo ratings yet
- Spesialit Obat Gastro MeDocument4 pagesSpesialit Obat Gastro MeHanadya Femer RajagukgukNo ratings yet
- Hatch Waxman Act and Generic Drugs PDFDocument6 pagesHatch Waxman Act and Generic Drugs PDFGaming ViperNo ratings yet
- Endocrinology - Internal Medicine, Dr. A. Mowafy (2020-2021)Document172 pagesEndocrinology - Internal Medicine, Dr. A. Mowafy (2020-2021)Mohammed RisqNo ratings yet
- Clinical SignificanceDocument3 pagesClinical Significanceapi-539267574No ratings yet
- Neurotransmitter Cheat Sheet AP ReviewDocument2 pagesNeurotransmitter Cheat Sheet AP ReviewNathania DawitNo ratings yet
- Insulin Therapy - A Pocket Guide 2013Document86 pagesInsulin Therapy - A Pocket Guide 2013Ismai Eko SaputraNo ratings yet
- Clinical Neurology and Neurosurgery: Case ReportDocument2 pagesClinical Neurology and Neurosurgery: Case ReportBhanu DahiyaNo ratings yet
- The Pharmacist Guide To Implementing Pharmaceutical Care PDFDocument502 pagesThe Pharmacist Guide To Implementing Pharmaceutical Care PDFLuis SosaNo ratings yet
- Card RepertoryDocument6 pagesCard RepertorySuhas IngaleNo ratings yet
- PDFDocument14 pagesPDFmuhammad rustamNo ratings yet
- Drug Study PethidineDocument2 pagesDrug Study Pethidinerica sebabillonesNo ratings yet
- Acute Pyelonephritis: Causes/ Risk FactorsDocument6 pagesAcute Pyelonephritis: Causes/ Risk FactorsShiraishiNo ratings yet
- Fluticasone Furoate Nasal SprayDocument59 pagesFluticasone Furoate Nasal Sprayhamna fitriahNo ratings yet
- Dr. Reddy's API Product List PDFDocument9 pagesDr. Reddy's API Product List PDFROUNAK PALNo ratings yet
- GIT - Dr. Allam 2021 PDFDocument47 pagesGIT - Dr. Allam 2021 PDFMohammedNo ratings yet
- Kmab 14 2111748Document20 pagesKmab 14 2111748bilou hertNo ratings yet
- MEDICATIONSDocument16 pagesMEDICATIONSCynthia LuayNo ratings yet
- Minutes 246th Registration Board PDFDocument496 pagesMinutes 246th Registration Board PDFAbdullah BhattiNo ratings yet
- Derma Quiz 2 NotesDocument9 pagesDerma Quiz 2 NotesJolaine ValloNo ratings yet
- Cerebral VasculitisDocument46 pagesCerebral VasculitisMatteo PaolucciNo ratings yet
- Amide ImpurityDocument11 pagesAmide Impuritymailtorubal2573No ratings yet
- Are Fish The Victims of 'Speciesism' A Discussion About Fear, Pain and Animal ConsciousnessDocument12 pagesAre Fish The Victims of 'Speciesism' A Discussion About Fear, Pain and Animal ConsciousnessReuben DylanNo ratings yet
- Metformin Poisoning - UpToDateDocument7 pagesMetformin Poisoning - UpToDateLucian SiriteanuNo ratings yet
- Toster And-BeattyDocument2 pagesToster And-BeattyGabrysia MajsikNo ratings yet