You might also like
- Drug Induced Liver DisordersDocument31 pagesDrug Induced Liver DisordersJason fernandes jNo ratings yet
- Antituberculosis Treatment Hepatotoxicity MechanismsDocument6 pagesAntituberculosis Treatment Hepatotoxicity Mechanismsadilah fazliNo ratings yet
- Welcome To Journal Club Presentation: Presented byDocument54 pagesWelcome To Journal Club Presentation: Presented byneptorNo ratings yet
- Drug-Induced Liver Disease.Document16 pagesDrug-Induced Liver Disease.Dr. Ammar Khalil100% (1)
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaDocument36 pagesATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Drug Induced Liver InjuryDocument13 pagesDrug Induced Liver InjuryIhsan PutraNo ratings yet
- Drug Induced Liver Diseases (DILD) : M. DeepalakshmiDocument22 pagesDrug Induced Liver Diseases (DILD) : M. DeepalakshmicrissNo ratings yet
- AKI DrugsDocument4 pagesAKI DrugsPIH SHTNo ratings yet
- Prescribing in Patients With Liver Disease: Rakesh K TandonDocument4 pagesPrescribing in Patients With Liver Disease: Rakesh K Tandonjoydeep chakrabortyNo ratings yet
- Drug Induced NephrotoxicityDocument15 pagesDrug Induced NephrotoxicityMUGHALNo ratings yet
- Which Psychotropic Medications Induce He PDFDocument9 pagesWhich Psychotropic Medications Induce He PDFnisastNo ratings yet
- Drug Induced Liver Diseases in The Elderly: Chandy GM, Chandy RGDocument4 pagesDrug Induced Liver Diseases in The Elderly: Chandy GM, Chandy RGkazekiraNo ratings yet
- ANTIMICROBIAL PRESCRIPTIONDocument64 pagesANTIMICROBIAL PRESCRIPTIONMalueth AnguiNo ratings yet
- ADRsDocument54 pagesADRsraffia mahakNo ratings yet
- Drug-Induced Liver DiseaseDocument20 pagesDrug-Induced Liver DiseaseNoreen ArshadNo ratings yet
- Chandok Et Al, 2010Document8 pagesChandok Et Al, 2010Cika Zahrah DewisoniaNo ratings yet
- Nephrotoxic DrugsDocument8 pagesNephrotoxic DrugsAhmad Radhya DionandaNo ratings yet
- Anticancer Drugs 2Document15 pagesAnticancer Drugs 2shotot767No ratings yet
- ChoiDocument19 pagesChoiLuciana RafaelNo ratings yet
- Drug Therapy of Viral Hepatitis 1-Hepatitis A: Passive ImmunityDocument4 pagesDrug Therapy of Viral Hepatitis 1-Hepatitis A: Passive ImmunityOsama El ShfieNo ratings yet
- First do no harmDocument21 pagesFirst do no harmPHARMACY 2021No ratings yet
- Review: Hepatocellular Damage From Non-Steroidal Anti-Inflammatory DrugsDocument5 pagesReview: Hepatocellular Damage From Non-Steroidal Anti-Inflammatory Drugsshessy-jolycia-kerrora-3047No ratings yet
- Porphyrias: Implications For Anaesthesia, Critical Care: Speaker: DR Bharani Kumar Moderator: DR Sherine KoudairaDocument20 pagesPorphyrias: Implications For Anaesthesia, Critical Care: Speaker: DR Bharani Kumar Moderator: DR Sherine KoudairaBharani KumarNo ratings yet
- Phenelzine - Liver ToxicityDocument8 pagesPhenelzine - Liver Toxicitydo leeNo ratings yet
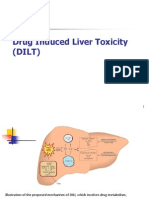
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- Hypomagnesemia A Clinical Approach in Chronically Ill Patients With Multiple ComorbiditiesDocument14 pagesHypomagnesemia A Clinical Approach in Chronically Ill Patients With Multiple ComorbiditiesAthenaeum Scientific PublishersNo ratings yet
- Efectoas Adversos AtbDocument13 pagesEfectoas Adversos AtbAgueda MaribelNo ratings yet
- GinjalDocument11 pagesGinjalOneng IfayaniNo ratings yet
- Metabolic Precautions and ER Reccomendations (Parikh, MD, 2007)Document5 pagesMetabolic Precautions and ER Reccomendations (Parikh, MD, 2007)F4AR100% (1)
- Wernicke EncephalopathyDocument8 pagesWernicke Encephalopathydrkadiyala2100% (1)
- ADE & Factors Affecting Drug Response 2016 Draft 1Document45 pagesADE & Factors Affecting Drug Response 2016 Draft 1احمد علىNo ratings yet
- Drug Induced LiverDocument8 pagesDrug Induced LiverDita IndahNo ratings yet
- Jurnal Pendukung Proposal 9Document4 pagesJurnal Pendukung Proposal 9Munawwar AweNo ratings yet
- Adverse Drug ReactionsDocument21 pagesAdverse Drug ReactionsRohit100% (1)
- Drug Induced Pathology in The Large IntestineDocument9 pagesDrug Induced Pathology in The Large IntestineBlumeNo ratings yet
- Hepatotoxicity From Biologics?: Ross Pierce, M.D. Division of Hematology, Obrr/Cber/FdaDocument16 pagesHepatotoxicity From Biologics?: Ross Pierce, M.D. Division of Hematology, Obrr/Cber/Fdansk79in@gmail.comNo ratings yet
- Drug Induced Kidney DiseaseDocument12 pagesDrug Induced Kidney DiseaseTusharNo ratings yet
- Drug Induced Liver Disease 2007Document226 pagesDrug Induced Liver Disease 2007Eric GibsonNo ratings yet
- HyperammonemiaDocument10 pagesHyperammonemiaAsfoor gake1No ratings yet
- Speaker-Arindam Pande Chairperson - Prof. B K Dey Prof. S B GangulyDocument66 pagesSpeaker-Arindam Pande Chairperson - Prof. B K Dey Prof. S B GangulyhananNo ratings yet
- Acute HepatitisDocument36 pagesAcute HepatitisMuhammad BilalNo ratings yet
- Acute Liver Failure: Concise ReviewDocument8 pagesAcute Liver Failure: Concise ReviewJoseph Stans KasiryeNo ratings yet
- Adult Health Nursing Phase I Thursday 6:00-9:00 PM: Irritable Bowel SyndromeDocument18 pagesAdult Health Nursing Phase I Thursday 6:00-9:00 PM: Irritable Bowel SyndromeLavinia Malazarte CaballeroNo ratings yet
- 3 and 4 Management of Medically CompromisedDocument63 pages3 and 4 Management of Medically Compromisedranareda499No ratings yet
- Drug-Induced Kidney Disease: ArticleDocument11 pagesDrug-Induced Kidney Disease: Articledwi harisNo ratings yet
- Adverse Reactions To FluoroquinolonesDocument3 pagesAdverse Reactions To FluoroquinolonesAvelox FloxNo ratings yet
- DILIDocument14 pagesDILIfadi01234No ratings yet
- Seizure On CKDDocument5 pagesSeizure On CKDDita Paramita HaryatiNo ratings yet
- Drug-induced liver injury causes and agentsDocument5 pagesDrug-induced liver injury causes and agentsospapNo ratings yet
- ImmunodisorderDocument28 pagesImmunodisorderabdoNo ratings yet
- Soluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesDocument11 pagesSoluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesShiela Montances100% (1)
- Acetaminophen-Induced Hepatotoxicity PDFDocument12 pagesAcetaminophen-Induced Hepatotoxicity PDFFranklin AvilaNo ratings yet
- Hepatic Encephalopathy: DR Sadath HussainDocument32 pagesHepatic Encephalopathy: DR Sadath Hussain966342No ratings yet
- Acute Pancreatitis-A Clinical Update: Review ArticleDocument6 pagesAcute Pancreatitis-A Clinical Update: Review ArticleDương Ngọc DiệpNo ratings yet
- Drug-Induced Nephrotoxicity: A Review of Risk Factors and BiomarkersDocument9 pagesDrug-Induced Nephrotoxicity: A Review of Risk Factors and BiomarkersCecep Darwis MuttaqinNo ratings yet
- Electrolyte Disturbances in Patients With Chronic Alcohol Use DisorderDocument10 pagesElectrolyte Disturbances in Patients With Chronic Alcohol Use DisorderBookwormNo ratings yet
- Clinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsDocument26 pagesClinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsNadia Ancharuz100% (1)
- Agranulocytosis, A Simple Guide to The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAgranulocytosis, A Simple Guide to The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 1 s2.0 S0045206818311969 MainDocument20 pages1 s2.0 S0045206818311969 MainLuiz Guilherme FiorinNo ratings yet
- Cancer-Related Inflammation as the Seventh Hallmark of CancerDocument9 pagesCancer-Related Inflammation as the Seventh Hallmark of Cancerlucia coronaNo ratings yet
- Growth Factors & Cell Death...Document22 pagesGrowth Factors & Cell Death...siddhi meenaNo ratings yet
- Accepted Manuscript: Advances in Colloid and Interface ScienceDocument171 pagesAccepted Manuscript: Advances in Colloid and Interface ScienceMarinoChavarroCordobaNo ratings yet
- Mitochondria More Than JustDocument10 pagesMitochondria More Than JustCarla MONo ratings yet
- (Carbon Nanostructures) Gil Gonçalves, Paula Marques, Mercedes Vila (Eds.) - Graphene-Based Materials in Health and Environment - New Paradigms-Springer International Publishing (2016)Document358 pages(Carbon Nanostructures) Gil Gonçalves, Paula Marques, Mercedes Vila (Eds.) - Graphene-Based Materials in Health and Environment - New Paradigms-Springer International Publishing (2016)lonelystar19No ratings yet
- Medication Related Osteonecrosis of The Jaw - Otto SvenDocument216 pagesMedication Related Osteonecrosis of The Jaw - Otto SvenNicoPaullierNo ratings yet
- PromoCellKatalog2013 LowresDocument212 pagesPromoCellKatalog2013 LowresmohdkhairNo ratings yet
- Cell Injury, Inflammation, and Repair ProcessesDocument55 pagesCell Injury, Inflammation, and Repair Processesgabb bbNo ratings yet
- Cancer HandoutDocument2 pagesCancer Handoutry22041996No ratings yet
- Suyama, Takashi L.: Electronic Theses and Dissertations UC San DiegoDocument409 pagesSuyama, Takashi L.: Electronic Theses and Dissertations UC San DiegoDiego Contreras HernándezNo ratings yet
- Jurnal Spinal Cord InjuryDocument14 pagesJurnal Spinal Cord InjurynuvitaNo ratings yet
- Mechanisms of Drug-Induced HepatotoxicityDocument20 pagesMechanisms of Drug-Induced Hepatotoxicityfebri kusuma arfiskaNo ratings yet
- Mpmi 05 23 0073 HHDocument8 pagesMpmi 05 23 0073 HHRoden Carlo LizardoNo ratings yet
- Role of Oxidative Stress in Semen Quality of Infertile MenDocument9 pagesRole of Oxidative Stress in Semen Quality of Infertile MenAyadPalaniNo ratings yet
- Cell Injury: Dr. Sanjiv Kumar Assistant Professor, Deptt. of Pathology, BVC, PatnaDocument32 pagesCell Injury: Dr. Sanjiv Kumar Assistant Professor, Deptt. of Pathology, BVC, PatnaAjinkya JadhaoNo ratings yet
- Cell DeathDocument21 pagesCell DeathBlaNo ratings yet
- Last Look PathologyDocument136 pagesLast Look Pathologyrama100% (1)
- Bisc 3150 General Pathology: Neoplasia Wednesday, January 31, 2018 Friday, February 2, 2018 Judy Maloney, PHDDocument62 pagesBisc 3150 General Pathology: Neoplasia Wednesday, January 31, 2018 Friday, February 2, 2018 Judy Maloney, PHDEvan PfeiferNo ratings yet
- Jejas SelDocument26 pagesJejas SelDesy NataliaNo ratings yet
- GuiaDocument5 pagesGuiaGustavo LopezNo ratings yet
- (Methods in Molecular Biology 1644) Vladimir V. Didenko (Eds.) - Fast Detection of DNA Damage - Methods and Protocols-Springer New York (2017) PDFDocument213 pages(Methods in Molecular Biology 1644) Vladimir V. Didenko (Eds.) - Fast Detection of DNA Damage - Methods and Protocols-Springer New York (2017) PDFMauro Porcel de PeraltaNo ratings yet
- PR 2001219Document10 pagesPR 2001219Amr Mohamed GalalNo ratings yet
- Labdanes of Natural Origin-Biological ActivitiesDocument24 pagesLabdanes of Natural Origin-Biological Activitiestheyuri@tlen.plNo ratings yet
- Khan Academy Cellular Development QuestionsDocument3 pagesKhan Academy Cellular Development QuestionsLoraNo ratings yet
- Notes Pathoma Webinar PDF PDFDocument84 pagesNotes Pathoma Webinar PDF PDFNosheen Hafeez100% (1)
- The Effects of Zhikang Capsule On The Growth and Apoptosis of Breast Cancer Mcf7Document4 pagesThe Effects of Zhikang Capsule On The Growth and Apoptosis of Breast Cancer Mcf7Riya CassendraNo ratings yet
- MetS genetic links and pathogenesis updateDocument15 pagesMetS genetic links and pathogenesis updateMunteanu DragosNo ratings yet
- Pathoma Notes CH 1-3Document11 pagesPathoma Notes CH 1-3imdaking12392% (25)
- Mitochondrial Mechanisms of Degeneration and Repair in Parkinson's DiseaseDocument279 pagesMitochondrial Mechanisms of Degeneration and Repair in Parkinson's Diseasek5blazerNo ratings yet