You might also like
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Acute Pyelonephritis in Adults: A Case Series of 223 PatientsDocument6 pagesAcute Pyelonephritis in Adults: A Case Series of 223 PatientsshiaNo ratings yet
- Silent NightDocument6 pagesSilent NightApril Rae Obregon GarcesNo ratings yet
- Does Tuberculosis After Kidney Transplantation Follow The Trend of Tuberculosis in General PopulationDocument12 pagesDoes Tuberculosis After Kidney Transplantation Follow The Trend of Tuberculosis in General Populationaisyah zlhjhNo ratings yet
- Cytomegalovirus Prophylaxis With Valganciclovir in Cytomegalovirus-Seropositive Kidney-Transplant PatientsDocument5 pagesCytomegalovirus Prophylaxis With Valganciclovir in Cytomegalovirus-Seropositive Kidney-Transplant PatientspicapicapicapedroNo ratings yet
- Tuberculosis in Patients On DialysisDocument5 pagesTuberculosis in Patients On Dialysisvasarhely imolaNo ratings yet
- 2014 Article 639Document8 pages2014 Article 639Anida HasnaNo ratings yet
- Long-Term Outcomes of Hepatitis B Virus-Related Cirrhosis Treated With Nucleos (T) Ide AnalogsDocument10 pagesLong-Term Outcomes of Hepatitis B Virus-Related Cirrhosis Treated With Nucleos (T) Ide AnalogsZulfiana NabilaNo ratings yet
- 2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)Document6 pages2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- Hepatitis C and Renal Disease: Epidemiology, Diagnosis, Pathogenesis and TherapyDocument14 pagesHepatitis C and Renal Disease: Epidemiology, Diagnosis, Pathogenesis and TherapyLinYi-FuNo ratings yet
- Post-Renal Transplant Infections: Single-Center Experience From NigeriaDocument9 pagesPost-Renal Transplant Infections: Single-Center Experience From NigeriaRaquel JimenezNo ratings yet
- 68 JMSCRDocument3 pages68 JMSCRVani Junior LoverzNo ratings yet
- WJH 3 130bacteremiaDocument7 pagesWJH 3 130bacteremiaLasiaf AlaskaNo ratings yet
- Delay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportDocument5 pagesDelay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportSneeze LouderNo ratings yet
- Hep Chiv Renal DZDocument9 pagesHep Chiv Renal DZSundar RamanathanNo ratings yet
- Cytomegalovirus:: Clinical Virological Correlations in Renal Transplant RecipientsDocument10 pagesCytomegalovirus:: Clinical Virological Correlations in Renal Transplant RecipientsRaffaharianggaraNo ratings yet
- Ma Dengue D.c.lye eDocument4 pagesMa Dengue D.c.lye eJazmin ZantiNo ratings yet
- Articulo ADocument8 pagesArticulo AJaver Andres HernandezNo ratings yet
- Tuberculosis and Chronic Renal FailureDocument38 pagesTuberculosis and Chronic Renal FailureGopal ChawlaNo ratings yet
- Outcome Pe Termen Lung La AsociereDocument6 pagesOutcome Pe Termen Lung La AsocieredeliaNo ratings yet
- Use of F-FDG PET To Predict Response To First-Line Tuberculostatics in HIV-Associated TuberculosisDocument6 pagesUse of F-FDG PET To Predict Response To First-Line Tuberculostatics in HIV-Associated TuberculosisdhaniNo ratings yet
- Sepsis: R. Dwi HendradiankoDocument36 pagesSepsis: R. Dwi HendradiankoSukamdani Rachman100% (1)
- SaudiJKidneyDisTranspl302470-5143025 141710Document8 pagesSaudiJKidneyDisTranspl302470-5143025 141710AmatystNo ratings yet
- 18 BudimirDocument8 pages18 BudimirJain KasparNo ratings yet
- TID 9999 E13413Document5 pagesTID 9999 E13413saraabolghasemi1No ratings yet
- Ciroza Hepatica Si InfectiiDocument9 pagesCiroza Hepatica Si InfectiiDinu Diana ArdeleanuNo ratings yet
- A 1Document5 pagesA 1cikobernicaNo ratings yet
- PIIS1198743X14652605Document3 pagesPIIS1198743X14652605Gerald NacoNo ratings yet
- Hypocalcemia Is Associated With Disease Severity in Patients With DengueDocument5 pagesHypocalcemia Is Associated With Disease Severity in Patients With DengueDwitari Novalia HaraziNo ratings yet
- Rivaroxaban Treatment in Acute Proximal DVT Patients WithDocument18 pagesRivaroxaban Treatment in Acute Proximal DVT Patients WithZiha Zia Leonita FauziNo ratings yet
- Per-Protocol Repeat Kidney Biopsy Portends Relapse and Long-Term Outcome in Incident Cases of Proliferative Lupus NephritisDocument11 pagesPer-Protocol Repeat Kidney Biopsy Portends Relapse and Long-Term Outcome in Incident Cases of Proliferative Lupus Nephritisjose pablo quero reyesNo ratings yet
- Severe Systemic Cytomegalovirus Infection in An Immunocompetent Patient Outside The Intensive Care Unit: A Case ReportDocument4 pagesSevere Systemic Cytomegalovirus Infection in An Immunocompetent Patient Outside The Intensive Care Unit: A Case ReportSebastián Garay HuertasNo ratings yet
- Handajani 2019 IOP Conf. Ser. Earth Environ. Sci. 217 012051 PDFDocument8 pagesHandajani 2019 IOP Conf. Ser. Earth Environ. Sci. 217 012051 PDFCitrawati Dyah Kencono WunguNo ratings yet
- 58 JMSCRDocument4 pages58 JMSCRhumayun kabirNo ratings yet
- Abdominal Sepsis Prognostic FactorDocument6 pagesAbdominal Sepsis Prognostic FactorPrasojo JojoNo ratings yet
- Hemodialysis Catheter-Related Bloodstream InfectionsDocument7 pagesHemodialysis Catheter-Related Bloodstream InfectionsHGZ 83 MoreliaNo ratings yet
- Carbapenemase-Producing Klebsiella Pneumoniae and Hematologic MalignanciesDocument2 pagesCarbapenemase-Producing Klebsiella Pneumoniae and Hematologic MalignanciesMark ReinhardtNo ratings yet
- HCV Treat Now Singapore 2014Document33 pagesHCV Treat Now Singapore 2014Robert G. Gish, MDNo ratings yet
- Limitation Graft BiopsyDocument11 pagesLimitation Graft BiopsyWEE LENG GANNo ratings yet
- APJCP - Volume 23 - Issue 9 - Pages 2965-2971Document7 pagesAPJCP - Volume 23 - Issue 9 - Pages 2965-2971Ivania MarquezNo ratings yet
- Pi Is 1083879118313909Document2 pagesPi Is 1083879118313909Ljc JaslinNo ratings yet
- Demam TifoidDocument16 pagesDemam TifoidnaraNo ratings yet
- AML Presenting With TBDocument10 pagesAML Presenting With TBshahzadNo ratings yet
- Our Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicDocument5 pagesOur Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicRonny DoankNo ratings yet
- Dengue Shock Syndrome Complicated With Acute Liver Failure and Kidney Injury, Infective Endocarditis, and Deep Vein ThrombosisDocument4 pagesDengue Shock Syndrome Complicated With Acute Liver Failure and Kidney Injury, Infective Endocarditis, and Deep Vein ThrombosisputiridhaNo ratings yet
- Disseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractDocument3 pagesDisseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractAmelia Fitria DewiNo ratings yet
- Bou Quill Ard 2009Document3 pagesBou Quill Ard 2009Rohit RajeevanNo ratings yet
- Transient Hyperglycemia in Patients With Tuberculosis in Tanzania: Implications For Diabetes Screening AlgorithmsDocument10 pagesTransient Hyperglycemia in Patients With Tuberculosis in Tanzania: Implications For Diabetes Screening AlgorithmsNura RamadhanNo ratings yet
- Heparin-Binding Protein: A Diagnostic Biomarker of Urinary Tract Infection in AdultsDocument9 pagesHeparin-Binding Protein: A Diagnostic Biomarker of Urinary Tract Infection in AdultsFitria NurulfathNo ratings yet
- JurnalDocument5 pagesJurnalgustina mariantiNo ratings yet
- mc7 Impact of HIV and AIDS On Surgical PracticeDocument5 pagesmc7 Impact of HIV and AIDS On Surgical PracticeRichard EscalonaNo ratings yet
- Lupus Dupa InterferonDocument3 pagesLupus Dupa InterferondeliaNo ratings yet
- Fan TVP PICC Riva Vs Warfa 2017Document7 pagesFan TVP PICC Riva Vs Warfa 2017Diego TonelloNo ratings yet
- 4 PDFDocument12 pages4 PDFQiuju LuNo ratings yet
- COHORT - TB MenigealDocument11 pagesCOHORT - TB MenigealYA MAAPNo ratings yet
- tmp20EE TMPDocument9 pagestmp20EE TMPFrontiersNo ratings yet
- Abstracts of The 2016 TTS CongressDocument929 pagesAbstracts of The 2016 TTS CongresspksdfpksdNo ratings yet
- 12 11 PBDocument168 pages12 11 PBYS NateNo ratings yet
- Cirrhosis of LiverDocument6 pagesCirrhosis of LiverBlackHAT GAMINGNo ratings yet
- Inspection ReportDocument5 pagesInspection ReportVimal SinghNo ratings yet
- Vyankatesh City-IIDocument17 pagesVyankatesh City-IIapi-27095887No ratings yet
- 28 CryptorchidismDocument23 pages28 CryptorchidismFaisal Ibn MushtaqNo ratings yet
- Peduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Document11 pagesPeduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Grace BrigondoNo ratings yet
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Antifoam Oh Conz - GHS EngDocument11 pagesAntifoam Oh Conz - GHS EngOUSMAN SEIDNo ratings yet
- A Decade of Dementia Care Training Learning Needs PDFDocument10 pagesA Decade of Dementia Care Training Learning Needs PDFYovana Pachón PovedaNo ratings yet
- Art Comparison Essay ExampleDocument5 pagesArt Comparison Essay Exampleflrzcpaeg100% (2)
- Internal Audit Ratings GuideDocument19 pagesInternal Audit Ratings Guidesanranist2100% (3)
- Business Plan Group 1Document21 pagesBusiness Plan Group 1Vienzkie12 BatoonNo ratings yet
- HaloperidolDocument1 pageHaloperidolSalma AKNo ratings yet
- Common Causes of Calf Pain in Endurance Athletes: by Brad J. Bernardini, MD, FAAOS, Reconstructive OrthopedicsDocument2 pagesCommon Causes of Calf Pain in Endurance Athletes: by Brad J. Bernardini, MD, FAAOS, Reconstructive Orthopedicsbila inunNo ratings yet
- Chevron Thailand Employee and Contractor Handbook EngDocument200 pagesChevron Thailand Employee and Contractor Handbook EngAndré Lima100% (1)
- CrimPro Cases (Rule 116)Document45 pagesCrimPro Cases (Rule 116)elvinperiaNo ratings yet
- Uts Ganjil Bahasa Inggris Kelas 9Document11 pagesUts Ganjil Bahasa Inggris Kelas 9Ketua EE 2021 AndrianoNo ratings yet
- Lost Prehistorica Lost Prehistorica. Lost Creatures CombinedDocument157 pagesLost Prehistorica Lost Prehistorica. Lost Creatures CombinedVassilis Tsipopoulos100% (8)
- Periodontal Accelerated Osteogenic OrthodonticsDocument6 pagesPeriodontal Accelerated Osteogenic Orthodonticsyui cherryNo ratings yet
- Foundation of Professional Nursing PracticeDocument5 pagesFoundation of Professional Nursing PracticeIvan LouiseNo ratings yet
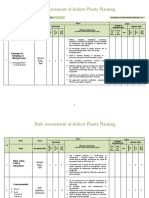
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Assessment of PersonalityDocument3 pagesAssessment of PersonalityRahman ButtNo ratings yet
- Psychological Communication Barriers PosterDocument1 pagePsychological Communication Barriers PostereliyaziyaNo ratings yet
- Window Cleaning Safety GuidelineDocument4 pagesWindow Cleaning Safety Guidelinejhunvalencia1203No ratings yet
- What Concentration Is The Best To Kill GermsDocument3 pagesWhat Concentration Is The Best To Kill GermsAncaja, Jameir 1CNo ratings yet
- Prokes Bahasa Inggris StuntingDocument15 pagesProkes Bahasa Inggris StuntingKameliaNo ratings yet
- Hizon Interview Group 2Document3 pagesHizon Interview Group 2Dan HizonNo ratings yet
- Science3 Q1 W4 Proper Use HandlingDocument50 pagesScience3 Q1 W4 Proper Use HandlingGina Contalba TubeoNo ratings yet
- UJA-Federation of New York Donor Recognition List 2022Document17 pagesUJA-Federation of New York Donor Recognition List 2022ericlkaplanNo ratings yet
- (S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFDocument8 pages(S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFVenom VerdinNo ratings yet
- HSC 430 - Lesson Plan Underage DrinkingDocument11 pagesHSC 430 - Lesson Plan Underage Drinkingapi-487139726No ratings yet
- EMP Procedure in MalaysiaDocument24 pagesEMP Procedure in Malaysialamkinpark3373No ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)