You might also like
- Indiana Contract With ID - MeDocument23 pagesIndiana Contract With ID - MeWTHR80% (5)
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Print Version - 2010-2016 Audi A6 (C7) Fuse Box DiagramDocument6 pagesPrint Version - 2010-2016 Audi A6 (C7) Fuse Box DiagramAyan ShaikhNo ratings yet
- Comprehensive Nursing Care PlanDocument3 pagesComprehensive Nursing Care PlanJaylord VerazonNo ratings yet
- Spinal Cord Injury NCPDocument2 pagesSpinal Cord Injury NCPEmmanuelRodriguez100% (1)
- NCP of Impaired MobilityDocument3 pagesNCP of Impaired MobilityHazel Cabrera0% (1)
- NCP Above The Knee AmputationDocument3 pagesNCP Above The Knee AmputationKristine AcasioNo ratings yet
- NCP Impaired MobilityDocument4 pagesNCP Impaired MobilityLouis LazaroNo ratings yet
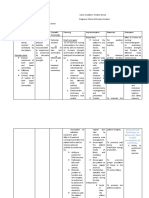
- Assessment Diagnosis Planning Implementation Rationale Desired Outcomes Subjective: "Napakasakit NG Mga Kasukasuhan Ko" As Verbalized by The PatientDocument5 pagesAssessment Diagnosis Planning Implementation Rationale Desired Outcomes Subjective: "Napakasakit NG Mga Kasukasuhan Ko" As Verbalized by The PatientAngelou Mortos100% (1)
- NCP Cva Impaired Physical MobilityDocument2 pagesNCP Cva Impaired Physical Mobilityexcel2112180% (5)
- Nursing Care Plan Acute Pain (Surgery AMB Incision)Document3 pagesNursing Care Plan Acute Pain (Surgery AMB Incision)deric100% (23)
- NEMA Standards Publication 250-1997: Enclosure TypesDocument5 pagesNEMA Standards Publication 250-1997: Enclosure TypesRock'nrollGuysNo ratings yet
- Nursing Care Plan - Spinal Cord InjuryDocument2 pagesNursing Care Plan - Spinal Cord Injuryderic92% (36)
- Sped and AlsDocument20 pagesSped and Alsrose dianne reyesNo ratings yet
- Oral Disease: Dental CariesDocument8 pagesOral Disease: Dental CariesAnna PruteanuNo ratings yet
- NAME: Sonwalkar Pratik Rohidas Class: 12 R1 Subject: Biology TOPIC: Detailed Study On Infertility Its Causes and TreatmentDocument27 pagesNAME: Sonwalkar Pratik Rohidas Class: 12 R1 Subject: Biology TOPIC: Detailed Study On Infertility Its Causes and TreatmentPratik Sonwalkar0% (1)
- Impaired Physical MobilityDocument8 pagesImpaired Physical MobilityKM78% (9)
- Production Technology of Date PalmDocument12 pagesProduction Technology of Date PalmAkash Tahir100% (2)
- SSPC SP1Document2 pagesSSPC SP1Jose AngelNo ratings yet
- NCP - BedriddenDocument4 pagesNCP - Bedriddenadelaigner_racho589475% (4)
- Nursing Care Plan: Precipitating FactorDocument8 pagesNursing Care Plan: Precipitating FactorJe Zal100% (1)
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
- Love Is More Powerful Than HateDocument4 pagesLove Is More Powerful Than Hatepachichoy100% (3)
- Analyst Validation Protocol PCR No.: Avalon Cosmetics PVT LTD ACPL/QA/AV/002 Page: 1 of 13Document13 pagesAnalyst Validation Protocol PCR No.: Avalon Cosmetics PVT LTD ACPL/QA/AV/002 Page: 1 of 13Sankar ChinnathambiNo ratings yet
- Nursing Care Plan-AscitesDocument10 pagesNursing Care Plan-AscitesKayki Louise75% (4)
- Instrument Assisted Soft Tissue MobilizationDocument5 pagesInstrument Assisted Soft Tissue MobilizationJordan QuillNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- NCP OrthoDocument2 pagesNCP OrthoJeyser T. GamutiaNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care Planaprilkate banagodosNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument6 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationRenea Joy ArruejoNo ratings yet
- JournalDocument15 pagesJournalRodolfo CampoNo ratings yet
- Nursing ManagementDocument3 pagesNursing Managementjames quintoNo ratings yet
- NCP Rheumatoid Arthritis DX IpmDocument2 pagesNCP Rheumatoid Arthritis DX IpmPatty RomeroNo ratings yet
- NCPDocument2 pagesNCPsphinx809100% (2)
- Student Nurses' Community: Nursing Care Plan AmputationDocument3 pagesStudent Nurses' Community: Nursing Care Plan AmputationNur faizah bt azmiNo ratings yet
- Clinimetric Properties of The Motor Activity Log For The Assessment of Arm Use in Hemiparetic PatientsDocument6 pagesClinimetric Properties of The Motor Activity Log For The Assessment of Arm Use in Hemiparetic PatientsMunni KNo ratings yet
- Nursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationDocument3 pagesNursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationSheril Sularte CasanesNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanLjae NatinoNo ratings yet
- NCPDocument2 pagesNCPJanice SolamilloNo ratings yet
- Geria NCP, Dela CruzDocument7 pagesGeria NCP, Dela CruzStephany Dela CruzNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlanLaceth Joyce T. LASATNo ratings yet
- Nursing Care Plan (Surgical, CS)Document5 pagesNursing Care Plan (Surgical, CS)Nursing LectureNo ratings yet
- NCP For Gouty ArthritisDocument3 pagesNCP For Gouty ArthritisMolly HollyNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationLillabinNo ratings yet
- NCP For Breast CancerDocument2 pagesNCP For Breast Cancergeng gengNo ratings yet
- Assess Ment Nursing Diagnos IS Plannin G Nursing Interve Ntion Rationa LE Evaluat IONDocument2 pagesAssess Ment Nursing Diagnos IS Plannin G Nursing Interve Ntion Rationa LE Evaluat IONStephany Dela CruzNo ratings yet
- Assessment Nursing Diagnosis PlanningDocument2 pagesAssessment Nursing Diagnosis PlanningCamille RamosNo ratings yet
- Nursing Care Plan For Ischemic Stroke ProblemDocument2 pagesNursing Care Plan For Ischemic Stroke ProblemA HNo ratings yet
- NCPDocument3 pagesNCPShei LaNo ratings yet
- NCP CSDocument4 pagesNCP CSJM UncianoNo ratings yet
- Artillo NCP Renal Cell CarcinomaDocument5 pagesArtillo NCP Renal Cell CarcinomaAl TheóNo ratings yet
- Assessmen T Nursing Diagnosi S Nursing Goal Nursing Intervention Rationale Subjective Cues: Independent IndependentDocument3 pagesAssessmen T Nursing Diagnosi S Nursing Goal Nursing Intervention Rationale Subjective Cues: Independent IndependentKim Glaidyl BontuyanNo ratings yet
- Nursing Care Plan: Submitted By: Sabay, Kyle VDocument11 pagesNursing Care Plan: Submitted By: Sabay, Kyle VKYLE SABAYNo ratings yet
- Manguiat, Ncma 111 RomeoDocument4 pagesManguiat, Ncma 111 RomeoCiara ManguiatNo ratings yet
- Impaired MobilityDocument3 pagesImpaired MobilityAbegail QuintoNo ratings yet
- Dizon P NCP 1 08 11 22Document3 pagesDizon P NCP 1 08 11 22Patricia Ellyne DizonNo ratings yet
- Subjective Cues:: Nursing Care ProcessDocument8 pagesSubjective Cues:: Nursing Care ProcessBianca Marithè RejanoNo ratings yet
- S: "Masakit Ang Ulo at Tiyan Niya" As Verbalized byDocument2 pagesS: "Masakit Ang Ulo at Tiyan Niya" As Verbalized bydenise-iceNo ratings yet
- 2 Nursing Care PlanDocument3 pages2 Nursing Care PlanJay Ar YasolNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Name of Patient: IndependentDocument5 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Name of Patient: IndependentJoyce ManimtimNo ratings yet
- NCP CHDG DutyDocument2 pagesNCP CHDG DutyLara Flyn TeofiloNo ratings yet
- NCP (BD)Document5 pagesNCP (BD)Nursing LectureNo ratings yet
- Crioterapia Ou Exercícios de Recarga Gradual em Apresentações Agudas de Tendinopatia Do Manguito Rotador Um Estudo Controlado RandomizadoDocument8 pagesCrioterapia Ou Exercícios de Recarga Gradual em Apresentações Agudas de Tendinopatia Do Manguito Rotador Um Estudo Controlado RandomizadoRodrigo AristidesNo ratings yet
- Artillo NCP Renal Cell CarcinomaDocument5 pagesArtillo NCP Renal Cell CarcinomaAl TheóNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanKatrene Lequigan100% (1)
- Carry Out The Doctor's Order (E.g. Kardex, Meds Chart, Tickets)Document11 pagesCarry Out The Doctor's Order (E.g. Kardex, Meds Chart, Tickets)Yosef OxinioNo ratings yet
- Manual of Vibration Exercise and Vibration TherapyFrom EverandManual of Vibration Exercise and Vibration TherapyJörn RittwegerNo ratings yet
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodFrom EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNo ratings yet
- Bionic Limb ReconstructionFrom EverandBionic Limb ReconstructionOskar C. AszmannNo ratings yet
- ASSIGNMENT CHM557-mergedDocument3 pagesASSIGNMENT CHM557-mergedAhmad ZakwanNo ratings yet
- The Economic Infrastructure: Task 1a. VocabularyDocument5 pagesThe Economic Infrastructure: Task 1a. VocabularyPolina Nalistia IrawanNo ratings yet
- MSDS Capilene G 86 EDocument4 pagesMSDS Capilene G 86 Ezubair1951No ratings yet
- Schletter ProductSheet PitchedRoof Pro - N ENDocument2 pagesSchletter ProductSheet PitchedRoof Pro - N ENf789sgacanonNo ratings yet
- Cadbury Operations ProjectDocument28 pagesCadbury Operations Projectparulhrm80% (5)
- Lesson 1 - Basic Principles of PlumbingDocument12 pagesLesson 1 - Basic Principles of PlumbingNicholas Bonn Sing100% (1)
- Hong Kong KalachuchiDocument3 pagesHong Kong KalachuchigAARaNo ratings yet
- House Sitting AgreementDocument16 pagesHouse Sitting AgreementjamesNo ratings yet
- Stated ModulDocument3 pagesStated Modulweldy kurniawanNo ratings yet
- Unistrut P2072A SubmittalDocument1 pageUnistrut P2072A SubmittalPaing Phyo AungNo ratings yet
- Zincoseal 605 M - Data SheetDocument2 pagesZincoseal 605 M - Data SheetGANESHNo ratings yet
- Research Paper UCSPDocument7 pagesResearch Paper UCSPJohn Adrian PadriqueNo ratings yet
- Report On Attendance: Magwawa Integrated SchoolDocument2 pagesReport On Attendance: Magwawa Integrated SchoolEeve YhoungNo ratings yet
- Amendment 3 To AIS 156Document7 pagesAmendment 3 To AIS 156pranavNo ratings yet
- BEKS - Annual Report - 2017 - Revisi PDFDocument596 pagesBEKS - Annual Report - 2017 - Revisi PDFWilliam WongNo ratings yet
- Ground Mounts: SpeedDocument12 pagesGround Mounts: SpeedJ GilNo ratings yet
- HARTZELL P9EA - Rev17 PIPER PA30Document9 pagesHARTZELL P9EA - Rev17 PIPER PA30Enrique F. Zamalloa LeonNo ratings yet
- List of CarcinogensDocument3 pagesList of CarcinogensDisha TNo ratings yet
- District Issue Analysis Kathryn SmithDocument11 pagesDistrict Issue Analysis Kathryn Smithapi-456203716No ratings yet
- Drive Test Sim COF953MM - COMBATBALEREJO Offline Madiun, East Java November 30, 2020Document7 pagesDrive Test Sim COF953MM - COMBATBALEREJO Offline Madiun, East Java November 30, 2020Akhmad Hafid IrawanNo ratings yet