You might also like
- Concrete Epoxy HV PDFDocument2 pagesConcrete Epoxy HV PDFGeovanni Mabiscay0% (1)
- Ats, TT, Tig: Anti Tetanus Serum, Tetanus Toxoid, Tetanus Immuno-GlobulinDocument15 pagesAts, TT, Tig: Anti Tetanus Serum, Tetanus Toxoid, Tetanus Immuno-Globulinjisoo100% (2)
- Kaiser Permanente HMO 20 California Region NorthernDocument12 pagesKaiser Permanente HMO 20 California Region NorthernAnonymous Wd0qp1X2UANo ratings yet
- Important Questions Answers Why This Matters:: IndividualDocument7 pagesImportant Questions Answers Why This Matters:: Individualsashank varmaNo ratings yet
- Healthyblue Advantage Platinum 500: Important Questions Answers Why This MattersDocument12 pagesHealthyblue Advantage Platinum 500: Important Questions Answers Why This MattersBertrandNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument8 pagesPlan Plan Plan Premium: Important Questions Answers Why This Mattersrocerev539No ratings yet
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument10 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- Important Questions Answers Why This MattersDocument6 pagesImportant Questions Answers Why This Mattersఅభినయ్ రెడ్డి కేNo ratings yet
- Oscar BenefitsDocument9 pagesOscar BenefitsDave TempleNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument6 pagesPlan Plan Plan Premium: Important Questions Answers Why This MattersDavid TranNo ratings yet
- 2019-2020 Full PPO 0 Deductible SBC PDFDocument9 pages2019-2020 Full PPO 0 Deductible SBC PDFrgbrbNo ratings yet
- Platinum Trio Hmo 0-25 Offex m0033963 01-24 SBCDocument9 pagesPlatinum Trio Hmo 0-25 Offex m0033963 01-24 SBCapi-531507901No ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersJunior GatbuntonNo ratings yet
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument8 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument11 pagesPlan Plan Plan Premium: Important Questions Answers Why This Matterseric.risnerNo ratings yet
- 2024 Ifp 771747 - 18628FL0160034 06 - SBCDocument10 pages2024 Ifp 771747 - 18628FL0160034 06 - SBCNayluNo ratings yet
- Kaiser Permanente HMO Plan Summary of Benefits and CoverageDocument12 pagesKaiser Permanente HMO Plan Summary of Benefits and CoverageGina FelyaNo ratings yet
- What This Health Plan CoversDocument10 pagesWhat This Health Plan CoversQFQEWFWQEFwqNo ratings yet
- B634ADT Blue Advantage Bronze HMO 006: This Is Only A SummaryDocument8 pagesB634ADT Blue Advantage Bronze HMO 006: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- 2024 KP Bronze SummaryDocument16 pages2024 KP Bronze Summaryapi-531507901No ratings yet
- CJL 5000 Hsa Plan 2024 SBC Final 10182023Document8 pagesCJL 5000 Hsa Plan 2024 SBC Final 10182023dominicvjohnson03No ratings yet
- Gig Harbor Active Plan 11Document6 pagesGig Harbor Active Plan 11api-307235383No ratings yet
- Silver 70 Off Exchange Trio HMO MG014322 01-24 SBCDocument9 pagesSilver 70 Off Exchange Trio HMO MG014322 01-24 SBCwannieNo ratings yet
- Kaiser Summary of Benefits 2024Document16 pagesKaiser Summary of Benefits 2024vaidish1No ratings yet
- Bronze 60 PPO MJ002189 01-24 SBCDocument9 pagesBronze 60 PPO MJ002189 01-24 SBCwannieNo ratings yet
- G622CHC Blue Choice Gold PPO 022: This Is Only A SummaryDocument8 pagesG622CHC Blue Choice Gold PPO 022: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- S608ADT Blue Advantage Silver HMO 018: This Is Only A SummaryDocument8 pagesS608ADT Blue Advantage Silver HMO 018: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument9 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- SumarioDocument9 pagesSumarioMiriangely GonzalezNo ratings yet
- Important Questions Answers Why This MattersDocument7 pagesImportant Questions Answers Why This Matterssashank varmaNo ratings yet
- Publix BCBS PPO Plan Coverage SummaryDocument7 pagesPublix BCBS PPO Plan Coverage SummaryAdam CliftonNo ratings yet
- University of Minnesota Student Health Insurance Plan SummaryDocument8 pagesUniversity of Minnesota Student Health Insurance Plan SummaryhotshinhwanatecomNo ratings yet
- This Is Only A Summary.: Important Questions Answers Why This MattersDocument10 pagesThis Is Only A Summary.: Important Questions Answers Why This MattersAnonymous D47ZzQZDtNo ratings yet
- WWW - Healthcare.Gov/Sbc-Glossary/: Important Questions Answers Why This MattersDocument10 pagesWWW - Healthcare.Gov/Sbc-Glossary/: Important Questions Answers Why This MattersSai SandeepNo ratings yet
- G622ADT Blue Advantage Gold HMO 016: This Is Only A SummaryDocument8 pagesG622ADT Blue Advantage Gold HMO 016: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Summary of Benefits and CoverageDocument155 pagesSummary of Benefits and CoverageTom HookNo ratings yet
- AMBETTER SECURE C5 STDDocument9 pagesAMBETTER SECURE C5 STDanarepsdcNo ratings yet
- Blue Shield Trio Bronze 60 Hmo 7000-70 Child Dental Alt m0033837 01-24 SBC 1Document9 pagesBlue Shield Trio Bronze 60 Hmo 7000-70 Child Dental Alt m0033837 01-24 SBC 1api-531507901No ratings yet
- Silver Trio HMO 2300-70 OffEx M0030308 01-23 SBCDocument10 pagesSilver Trio HMO 2300-70 OffEx M0030308 01-23 SBCjaroopaitummaiNo ratings yet
- WWW Healthcare Gov/sbc-GlossaryDocument6 pagesWWW Healthcare Gov/sbc-Glossarytroubledcutie1987No ratings yet
- 2024 KP Platinum SummaryDocument16 pages2024 KP Platinum Summaryapi-531507901No ratings yet
- S608CHC Blue Choice Silver PPO 024: This Is Only A SummaryDocument8 pagesS608CHC Blue Choice Silver PPO 024: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Summary BenefiDocument9 pagesSummary BenefiGita PatelNo ratings yet
- HDHPDocument10 pagesHDHPAnonymous KnnAxcNo ratings yet
- Allowed Amount Balance Billing Coinsurance Copayment Deductible ProviderDocument7 pagesAllowed Amount Balance Billing Coinsurance Copayment Deductible Providergary kornegayNo ratings yet
- For In-Home Supportive Services Workers: PASC-SEIU Homecare Workers Health Care PlanDocument9 pagesFor In-Home Supportive Services Workers: PASC-SEIU Homecare Workers Health Care PlanMustaffah KabelyyonNo ratings yet
- B601CHC Blue Choice Bronze PPO 031: This Is Only A SummaryDocument8 pagesB601CHC Blue Choice Bronze PPO 031: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- 2024 KP Gold SummaryDocument16 pages2024 KP Gold Summaryapi-531507901No ratings yet
- BD-CA7XAX-0624-SBCDocument10 pagesBD-CA7XAX-0624-SBCMauricio VazquezNo ratings yet
- Summary BenefitsDocument9 pagesSummary BenefitsKenneth HunterNo ratings yet
- BlueSelect 1456B Coverage SummaryDocument10 pagesBlueSelect 1456B Coverage SummarybrineshrimpNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument9 pagesPlan Plan Plan Premium: Important Questions Answers Why This MattersIvan GrondonaNo ratings yet
- SBC - Cdo - 2019 2Document6 pagesSBC - Cdo - 2019 2Dinko KajtezovićNo ratings yet
- BD-BHFRKN-0624-SBCDocument10 pagesBD-BHFRKN-0624-SBCMauricio VazquezNo ratings yet
- Plan Plan Plan: Important Questions Answers Why This MattersDocument5 pagesPlan Plan Plan: Important Questions Answers Why This MattersGerardo LeonNo ratings yet
- Aetna SBC 2024 Standard Plan Express ScriptsDocument15 pagesAetna SBC 2024 Standard Plan Express Scriptskatika3011No ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersAnonymous KnnAxcNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument12 pagesPlan Plan Plan Premium: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- Sumario Every Day BrozeDocument9 pagesSumario Every Day BrozeMiriangely GonzalezNo ratings yet
- Sakshijain75.Final ProDocument46 pagesSakshijain75.Final ProOm AherNo ratings yet
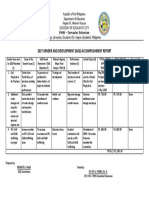
- GAD Accomplishment ReportDocument1 pageGAD Accomplishment ReportRenante Naga100% (6)
- Flashcards - CP4 Preparation of A Standard Solution and Titration - Edexcel IAL Chemistry A-LevelDocument37 pagesFlashcards - CP4 Preparation of A Standard Solution and Titration - Edexcel IAL Chemistry A-LevelTravel UnlimitedNo ratings yet
- Shandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23Document130 pagesShandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23mliugong94% (16)
- Plane Bearings: Material Indicator Shape or SeriesDocument4 pagesPlane Bearings: Material Indicator Shape or SeriesJuan LoaizaNo ratings yet
- Government Schemes Current Affairs PDF E Book PDFDocument106 pagesGovernment Schemes Current Affairs PDF E Book PDFRohini VjNo ratings yet
- Galati penitentiary historyDocument2 pagesGalati penitentiary historyLupu IonutNo ratings yet
- SITE. Defining Project Goals & ObjectivesDocument1 pageSITE. Defining Project Goals & Objectivescoach balaNo ratings yet
- Deliver VALUE and RENEWABLE FUTUREDocument30 pagesDeliver VALUE and RENEWABLE FUTUREAlexandru SuciuNo ratings yet
- Round-The-clock Acid Control of Rabeprazole On Acid Related DisorderDocument8 pagesRound-The-clock Acid Control of Rabeprazole On Acid Related DisorderRabeprazole SodiumNo ratings yet
- Effectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsDocument8 pagesEffectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsPutra SpNo ratings yet
- General Conditions of Contracts For NLNG 2018Document28 pagesGeneral Conditions of Contracts For NLNG 2018AF Dowell MirinNo ratings yet
- IRC Girl Shine Part 4 DigitalDocument124 pagesIRC Girl Shine Part 4 DigitalMónica SalesNo ratings yet
- Mcimt NDT Kids at 1Document12 pagesMcimt NDT Kids at 1api-485106673No ratings yet
- CSC 101-CSC 111 - Introduction To Computer Science - Lecture 1Document23 pagesCSC 101-CSC 111 - Introduction To Computer Science - Lecture 1CODE100% (1)
- Water Hammer PDFDocument30 pagesWater Hammer PDFbhavesh shuklaNo ratings yet
- Menu Baru Kopi GandapoeraDocument7 pagesMenu Baru Kopi GandapoeraAlwan AhpNo ratings yet
- Pre-Final Exam in Audit 2-3Document5 pagesPre-Final Exam in Audit 2-3Shr BnNo ratings yet
- Physics Investigatory Project Class 12Document12 pagesPhysics Investigatory Project Class 12shivanginirai7No ratings yet
- Chemistry Units 8 12Document29 pagesChemistry Units 8 12reg speckNo ratings yet
- Public Health EngineeringDocument10 pagesPublic Health EngineeringOmkar DeshpandeNo ratings yet
- Science Activity Sheet Quarter 4 - MELC 2 Week 2: Uses of WaterDocument13 pagesScience Activity Sheet Quarter 4 - MELC 2 Week 2: Uses of WaterShareinne TeamkNo ratings yet
- Tutorial Sheet 4Document2 pagesTutorial Sheet 4Syed YousufuddinNo ratings yet
- REBA Employee Assessment Worksheet: A. Neck, Trunk and Leg AnalysisDocument1 pageREBA Employee Assessment Worksheet: A. Neck, Trunk and Leg AnalysisAgni JayantiNo ratings yet
- MKT421 New Product Development PDFDocument26 pagesMKT421 New Product Development PDFNass AzwadiNo ratings yet
- 02 - Purulent Inflammatory DiseaseDocument60 pages02 - Purulent Inflammatory Diseaseshekhawatyuvraj051No ratings yet
- A Project Report: Maya Engineering WorksDocument2 pagesA Project Report: Maya Engineering WorksVishwendra SinghNo ratings yet
- 2.factory Price - Alarm Accessories-Complete 20150325Document15 pages2.factory Price - Alarm Accessories-Complete 20150325FREE BUSINESS INTELLIGENCENo ratings yet