You might also like
- 2019-2020 Full PPO 0 Deductible SBC PDFDocument9 pages2019-2020 Full PPO 0 Deductible SBC PDFrgbrbNo ratings yet
- Lactic AcidDocument6 pagesLactic AcidTaha AzNo ratings yet
- Kaiser Permanente HMO 20 California Region NorthernDocument12 pagesKaiser Permanente HMO 20 California Region NorthernAnonymous Wd0qp1X2UANo ratings yet
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument9 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument10 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersQFQEWFWQEFwqNo ratings yet
- A Grammar of Power in Psychotherapy Exploring The Dynamics of Privilege (Malin Fors)Document220 pagesA Grammar of Power in Psychotherapy Exploring The Dynamics of Privilege (Malin Fors)Andrea A. Ortiz Vázquez100% (1)
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument8 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- Aetna 1850 HD PlanDocument10 pagesAetna 1850 HD PlanNaveen ChintamaniNo ratings yet
- Current Issues On Construction Project ManagementDocument2 pagesCurrent Issues On Construction Project ManagementJoyce Abegail De PedroNo ratings yet
- Answer Key EXAM DRILL 2 - Community Health Nursing Nursing Practice Ii - CHN and Care of The Mother and ChildDocument24 pagesAnswer Key EXAM DRILL 2 - Community Health Nursing Nursing Practice Ii - CHN and Care of The Mother and Childbetiful83% (6)
- Substation Basic PDFDocument6 pagesSubstation Basic PDFSaraswatapalitNo ratings yet
- (Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Document589 pages(Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Andi sutandi100% (1)
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersDocument10 pagesHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- Bronze 60 PPO MJ002189 01-24 SBCDocument9 pagesBronze 60 PPO MJ002189 01-24 SBCwannieNo ratings yet
- Silver 70 Off Exchange Trio HMO MG014322 01-24 SBCDocument9 pagesSilver 70 Off Exchange Trio HMO MG014322 01-24 SBCwannieNo ratings yet
- Blue Shield Trio Bronze 60 Hmo 7000-70 Child Dental Alt m0033837 01-24 SBC 1Document9 pagesBlue Shield Trio Bronze 60 Hmo 7000-70 Child Dental Alt m0033837 01-24 SBC 1api-531507901No ratings yet
- 2024 Ifp 771747 - 18628FL0160034 06 - SBCDocument10 pages2024 Ifp 771747 - 18628FL0160034 06 - SBCNayluNo ratings yet
- Silver Trio HMO 2300-70 OffEx M0030308 01-23 SBCDocument10 pagesSilver Trio HMO 2300-70 OffEx M0030308 01-23 SBCjaroopaitummaiNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument11 pagesPlan Plan Plan Premium: Important Questions Answers Why This Matterseric.risnerNo ratings yet
- Oscar BenefitsDocument9 pagesOscar BenefitsDave TempleNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument8 pagesPlan Plan Plan Premium: Important Questions Answers Why This Mattersrocerev539No ratings yet
- BD Ca7xax 0624 SBCDocument10 pagesBD Ca7xax 0624 SBCMauricio VazquezNo ratings yet
- Important Questions Answers Why This MattersDocument7 pagesImportant Questions Answers Why This Matterssashank varmaNo ratings yet
- WWW - Healthcare.Gov/Sbc-Glossary/: Important Questions Answers Why This MattersDocument10 pagesWWW - Healthcare.Gov/Sbc-Glossary/: Important Questions Answers Why This MattersSai SandeepNo ratings yet
- Allowed Amount Balance Billing Coinsurance Copayment Deductible ProviderDocument7 pagesAllowed Amount Balance Billing Coinsurance Copayment Deductible Providergary kornegayNo ratings yet
- Summary BenefiDocument9 pagesSummary BenefiGita PatelNo ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersbrineshrimpNo ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersJunior GatbuntonNo ratings yet
- B634ADT Blue Advantage Bronze HMO 006: This Is Only A SummaryDocument8 pagesB634ADT Blue Advantage Bronze HMO 006: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Important Questions Answers Why This MattersDocument6 pagesImportant Questions Answers Why This Mattersఅభినయ్ రెడ్డి కేNo ratings yet
- Ambetter Secure C5 STDDocument9 pagesAmbetter Secure C5 STDanarepsdcNo ratings yet
- Plan Plan Plan Premium: Coverage Period: 01/01/2021-12/31/2021 Traditional PlanDocument12 pagesPlan Plan Plan Premium: Coverage Period: 01/01/2021-12/31/2021 Traditional PlanGina FelyaNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument6 pagesPlan Plan Plan Premium: Important Questions Answers Why This MattersDavid TranNo ratings yet
- Important Questions Answers Why This Matters:: IndividualDocument7 pagesImportant Questions Answers Why This Matters:: Individualsashank varmaNo ratings yet
- G622CHC Blue Choice Gold PPO 022: This Is Only A SummaryDocument8 pagesG622CHC Blue Choice Gold PPO 022: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- MVP Silver Summary of Benefits and CoverageDocument6 pagesMVP Silver Summary of Benefits and Coverageksenos.ukNo ratings yet
- B601CHC Blue Choice Bronze PPO 031: This Is Only A SummaryDocument8 pagesB601CHC Blue Choice Bronze PPO 031: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- BD BHFRKN 0624 SBCDocument10 pagesBD BHFRKN 0624 SBCMauricio VazquezNo ratings yet
- SHBP SBC Twin Cities Campus Student Only 2017-2018Document8 pagesSHBP SBC Twin Cities Campus Student Only 2017-2018hotshinhwanatecomNo ratings yet
- 2024 KP Bronze SummaryDocument16 pages2024 KP Bronze Summaryapi-531507901No ratings yet
- SumarioDocument9 pagesSumarioMiriangely GonzalezNo ratings yet
- S608CHC Blue Choice Silver PPO 024: This Is Only A SummaryDocument8 pagesS608CHC Blue Choice Silver PPO 024: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Summary BenefitsDocument9 pagesSummary BenefitsKenneth HunterNo ratings yet
- CJL 5000 Hsa Plan 2024 SBC Final 10182023Document8 pagesCJL 5000 Hsa Plan 2024 SBC Final 10182023dominicvjohnson03No ratings yet
- Gig Harbor Active Plan 11Document6 pagesGig Harbor Active Plan 11api-307235383No ratings yet
- 1500SBC2021Document8 pages1500SBC2021Carlos Andres Correa Gomez (Carlos Gomez)No ratings yet
- Sumario Every Day BrozeDocument9 pagesSumario Every Day BrozeMiriangely GonzalezNo ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersAnonymous KnnAxcNo ratings yet
- G622ADT Blue Advantage Gold HMO 016: This Is Only A SummaryDocument8 pagesG622ADT Blue Advantage Gold HMO 016: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This Mattersraj2642No ratings yet
- Bronze-7-Epo-1 1 22-12 31 22Document8 pagesBronze-7-Epo-1 1 22-12 31 22PSC RFQNo ratings yet
- SpdsDocument39 pagesSpdsVinod KumarNo ratings yet
- S608ADT Blue Advantage Silver HMO 018: This Is Only A SummaryDocument8 pagesS608ADT Blue Advantage Silver HMO 018: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Important Questions Answers Why This MattersDocument10 pagesImportant Questions Answers Why This MattersGeraldine HerreraNo ratings yet
- Cigna Open Access Plus Oap Buy Up Plan 3deo IncDocument11 pagesCigna Open Access Plus Oap Buy Up Plan 3deo IncLn TranNo ratings yet
- For In-Home Supportive Services Workers: PASC-SEIU Homecare Workers Health Care PlanDocument9 pagesFor In-Home Supportive Services Workers: PASC-SEIU Homecare Workers Health Care PlanMustaffah KabelyyonNo ratings yet
- Important Questions Answers Why This MattersDocument7 pagesImportant Questions Answers Why This MattersAdam CliftonNo ratings yet
- HDHPDocument10 pagesHDHPAnonymous KnnAxcNo ratings yet
- Administrator Benefits2020Document8 pagesAdministrator Benefits2020Thiago SilvaNo ratings yet
- This Is Only A Summary.: Important Questions Answers Why This MattersDocument10 pagesThis Is Only A Summary.: Important Questions Answers Why This MattersAnonymous D47ZzQZDtNo ratings yet
- Kaiser Summary of Benefits 2024Document16 pagesKaiser Summary of Benefits 2024vaidish1No ratings yet
- Important Questions Answers Why This Matters:: Plan Plan Plan Plan PremiumDocument12 pagesImportant Questions Answers Why This Matters:: Plan Plan Plan Plan PremiumscheriNo ratings yet
- Cigna Open Access Plus HDHP Hsa Plan 3deo IncDocument11 pagesCigna Open Access Plus HDHP Hsa Plan 3deo IncLn TranNo ratings yet
- Textbook of Urgent Care Management: Chapter 9, Insurance Requirements for the Urgent Care CenterFrom EverandTextbook of Urgent Care Management: Chapter 9, Insurance Requirements for the Urgent Care CenterNo ratings yet
- Dhmo PremierDocument10 pagesDhmo Premierapi-531507901No ratings yet
- 2024 KP Bronze SummaryDocument16 pages2024 KP Bronze Summaryapi-531507901No ratings yet
- Platinum Trio Hmo 0-25 Offex m0033963 01-24 SBCDocument9 pagesPlatinum Trio Hmo 0-25 Offex m0033963 01-24 SBCapi-531507901No ratings yet
- Slater Inc Vision 12052022Document5 pagesSlater Inc Vision 12052022api-531507901No ratings yet
- Slater Inc Vision 12052022Document5 pagesSlater Inc Vision 12052022api-531507901No ratings yet
- Slater Inc Dental EnglishDocument4 pagesSlater Inc Dental Englishapi-531507901No ratings yet
- Explain Why Seed Vigor Determination Is ImportantDocument5 pagesExplain Why Seed Vigor Determination Is ImportantSolomon MbeweNo ratings yet
- SM - Business PoliciesDocument46 pagesSM - Business PoliciesPrithvi AcharyaNo ratings yet
- Buy Lizol Floor Cleaner 5000 ML Online - GeMDocument4 pagesBuy Lizol Floor Cleaner 5000 ML Online - GeMHimanshu ShuklaNo ratings yet
- Separation of Plant Pigments PDFDocument3 pagesSeparation of Plant Pigments PDFneelNo ratings yet
- JSLHR Author InstructionsDocument14 pagesJSLHR Author InstructionsChanyanit CharoenpholNo ratings yet
- Ketone OxidationDocument20 pagesKetone OxidationNgurah MahasviraNo ratings yet
- Lab 2 - Capacitive ReactanceDocument4 pagesLab 2 - Capacitive Reactanceali basitNo ratings yet
- NURS FPX 6410 Assessment 2 Executive Summary To AdministrationDocument7 pagesNURS FPX 6410 Assessment 2 Executive Summary To Administrationzadem5266No ratings yet
- One Village One Product Movement in Laos: AbstractDocument5 pagesOne Village One Product Movement in Laos: Abstractoeleong19699685No ratings yet
- Reading Passage 1: IELTS Recent Actual Test With Answers Volume 1Document17 pagesReading Passage 1: IELTS Recent Actual Test With Answers Volume 1Amogha GadkarNo ratings yet
- Mem CalcDocument6 pagesMem CalcQruisedNo ratings yet
- ISO 9001 - 14001 - 2015 enDocument2 pagesISO 9001 - 14001 - 2015 enVĂN THÀNH TRƯƠNGNo ratings yet
- Unit of PowerDocument9 pagesUnit of PowerSarathrv RvNo ratings yet
- PGS 504 Notes Part IIDocument3 pagesPGS 504 Notes Part IISejal PriyaNo ratings yet
- SAVULESCU, Julian - A Simple Solution To The Puzzles of End of LifeDocument5 pagesSAVULESCU, Julian - A Simple Solution To The Puzzles of End of Lifediradosta_1992No ratings yet
- Soiltac Safety Data Sheet: Section 1 - IdentificationDocument9 pagesSoiltac Safety Data Sheet: Section 1 - IdentificationSameh AhmedNo ratings yet
- CORONADocument25 pagesCORONAMohammedNo ratings yet
- Request For New Tax DeclarationDocument2 pagesRequest For New Tax DeclarationAsterio MagootNo ratings yet
- Imaging-Guided Chest Biopsies: Techniques and Clinical ResultsDocument10 pagesImaging-Guided Chest Biopsies: Techniques and Clinical Resultsweni kartika nugrohoNo ratings yet
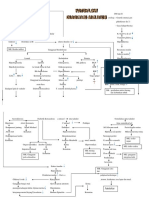
- Patoflow DMDocument2 pagesPatoflow DMAngel da CostaNo ratings yet
- MOLYKOTE 1000 Paste 71-0218H-01Document2 pagesMOLYKOTE 1000 Paste 71-0218H-01Victor PomboNo ratings yet
- Lab Manual For Series Parallel Rasonant CircuitDocument3 pagesLab Manual For Series Parallel Rasonant CircuitManoj PardhanNo ratings yet