You might also like
- Beaba Babycook Recipe BookDocument10 pagesBeaba Babycook Recipe BookFlorina Ciorba50% (2)
- Theories of Labor Ons-EtDocument19 pagesTheories of Labor Ons-EtHeron BayaninNo ratings yet
- Alex Tissandier Affirming Divergence PDFDocument194 pagesAlex Tissandier Affirming Divergence PDFDwi PlatomoNo ratings yet
- NASA: 181330main Jun29colorDocument8 pagesNASA: 181330main Jun29colorNASAdocumentsNo ratings yet
- Term 2 Examination Pointers For MCN LectureDocument11 pagesTerm 2 Examination Pointers For MCN Lecturezyyw.abello.uiNo ratings yet
- revkeDocument11 pagesrevkeLowellyn Grezen VillaflorNo ratings yet
- 1-Pre-Natal PeriodDocument61 pages1-Pre-Natal PeriodLady Mairyl N. BrigondoNo ratings yet
- Clinical Activities: A. Pre - ConsultationDocument13 pagesClinical Activities: A. Pre - ConsultationerykafadsNo ratings yet
- 2021 Fetal Growth and Assessment Student FileDocument95 pages2021 Fetal Growth and Assessment Student FileSheryll Ann DacayoNo ratings yet
- Obstetrical Nursing LaborDocument12 pagesObstetrical Nursing LaborJhen BasinilloNo ratings yet
- NCM 101 LectureDocument6 pagesNCM 101 LectureGrace Sabater CAragayNo ratings yet
- MCN Lec Reviewer FinalsDocument7 pagesMCN Lec Reviewer Finalszyyw.abello.uiNo ratings yet
- Charles Z. Ariola JR., MSN., LPT, Rn. Instructor IDocument22 pagesCharles Z. Ariola JR., MSN., LPT, Rn. Instructor ICharlz ZipaganNo ratings yet
- Maternity Nursing Review Part 2 1 6Document76 pagesMaternity Nursing Review Part 2 1 6yzaNo ratings yet
- Maternal and Child Health Nursing (NCM 101 Lect) Part 1Document4 pagesMaternal and Child Health Nursing (NCM 101 Lect) Part 1yunjung0518100% (7)
- Maternity Nursing Lecture on Fetal DevelopmentDocument580 pagesMaternity Nursing Lecture on Fetal DevelopmentknotstmNo ratings yet
- Fetal Circulation Development StagesDocument44 pagesFetal Circulation Development StagesMarc BantilanNo ratings yet
- German Measles Infection During Pregnancy Can Damage Fetal DevelopmentDocument5 pagesGerman Measles Infection During Pregnancy Can Damage Fetal DevelopmentJacobNo ratings yet
- OB & GyneDocument24 pagesOB & GyneJohn Christopher LucesNo ratings yet
- Nur 214 HandoutsDocument6 pagesNur 214 HandoutsCharlz ZipaganNo ratings yet
- REVIEWERDocument14 pagesREVIEWERMaria Lejani TerencioNo ratings yet
- Pregnancy Health Promotion and DevelopmentDocument11 pagesPregnancy Health Promotion and DevelopmentKathy Wollschleger100% (1)
- RACE Annotated ObsDocument35 pagesRACE Annotated ObsIsmath JahangirNo ratings yet
- TUGAS T1 A - Ukuran Serviks, Cardinal MovementDocument5 pagesTUGAS T1 A - Ukuran Serviks, Cardinal MovementHanan FareziNo ratings yet
- Case Study of Cesarean SectionDocument9 pagesCase Study of Cesarean SectionErika Joy Imperio0% (1)
- NCLEX Pregnancy NotesDocument3 pagesNCLEX Pregnancy NotesrustiejadeNo ratings yet
- DEATH AND INJURY IN INFANCYDocument186 pagesDEATH AND INJURY IN INFANCYQuarmina HesseNo ratings yet
- FertilizationDocument6 pagesFertilizationKristine Castillo100% (1)
- SwineDocument6 pagesSwineKimmy PusaNo ratings yet
- Maternal and Child Health IDocument772 pagesMaternal and Child Health Ikarendelarosa06100% (6)
- MCN Topic 1 Basic ConceptsDocument7 pagesMCN Topic 1 Basic ConceptsDiana CalderonNo ratings yet
- VETERINARY GYNECOLOGY AND OBSTETRICS (VGO 411 & 421) by H.M.BAROT (28-01-2018)-1Document39 pagesVETERINARY GYNECOLOGY AND OBSTETRICS (VGO 411 & 421) by H.M.BAROT (28-01-2018)-1Riya AdhangleNo ratings yet
- Foetal DevelopmentDocument50 pagesFoetal Developmentdipendrakumarkushawaha44No ratings yet
- Neonatology: By:W.G MokhlesDocument30 pagesNeonatology: By:W.G MokhlesWaris BarimanNo ratings yet
- DystociaDocument3 pagesDystociaRiajoy AsisNo ratings yet
- 107 Lec Prelim TopicsDocument22 pages107 Lec Prelim TopicsMary Ann SacramentoNo ratings yet
- PROM Case Analysis at Velez CollegeDocument43 pagesPROM Case Analysis at Velez Collegeinah krizia lagueNo ratings yet
- Nursing Bullets (Obstetrics & Gynaecology)Document17 pagesNursing Bullets (Obstetrics & Gynaecology)RF RFNo ratings yet
- Fertilization To Conception: Maternal and Child Health Nursing PregnancyDocument8 pagesFertilization To Conception: Maternal and Child Health Nursing PregnancyNikki M. Arapol100% (1)
- OB 2 Terms ExplainedDocument4 pagesOB 2 Terms ExplainedDragana AbramovicNo ratings yet
- Labor & DeliveryDocument14 pagesLabor & DeliveryNiña Eleana FranciscoNo ratings yet
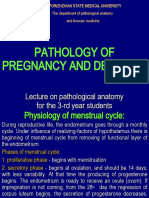
- Pathology of Pregnancy and Delivery: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocument35 pagesPathology of Pregnancy and Delivery: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- The Growing Fetus For CPDocument19 pagesThe Growing Fetus For CPyzaNo ratings yet
- Ob Peds Lecture Notes Nurse NursingDocument70 pagesOb Peds Lecture Notes Nurse Nursinglilchibaby3161100% (2)
- MCN NotesDocument20 pagesMCN Noteslyzzythasenci23No ratings yet
- Sexual Reproduction NotesDocument35 pagesSexual Reproduction NotesZelNo ratings yet
- Fetal DevelopmentDocument51 pagesFetal DevelopmentLhiet Aguilar Hipolito50% (2)
- Case Study (Placenta Previa)Document5 pagesCase Study (Placenta Previa)Jai - HoNo ratings yet
- Normal OB Notes. ReviewerDocument9 pagesNormal OB Notes. ReviewerNicole Danielle MallariNo ratings yet
- Maternal and Child NursingDocument9 pagesMaternal and Child NursingWarrenSandoval100% (12)
- OB Lec ArellanoDocument834 pagesOB Lec Arellanoervin_agena394No ratings yet
- Scrotal Conditions: Done By: Enas Almazraway Sarah Al-HawamdehDocument65 pagesScrotal Conditions: Done By: Enas Almazraway Sarah Al-HawamdehMohammad GharaibehNo ratings yet
- Reproductive Physiology and Anatomy of The Sow PDFDocument4 pagesReproductive Physiology and Anatomy of The Sow PDFCarol OrequesNo ratings yet
- Stages of Human Development Before BirthDocument3 pagesStages of Human Development Before BirthAaronotix GamingNo ratings yet
- DR - Sumeya: Normal Fetal Development and GrowthDocument42 pagesDR - Sumeya: Normal Fetal Development and Growthhussain AltaherNo ratings yet
- Profile of A NewbornDocument92 pagesProfile of A NewbornAirene AalaNo ratings yet
- EMBRYO DEVELOPMENT STAGESDocument31 pagesEMBRYO DEVELOPMENT STAGESSHEMAR STEWARTNo ratings yet
- Stages of Fetal Growth and DevelopmentDocument10 pagesStages of Fetal Growth and DevelopmentGrant KhangabNo ratings yet
- Mother and Child HealthDocument33 pagesMother and Child HealthJennifer Solano CruelNo ratings yet
- Maternity Study Guide 1Document14 pagesMaternity Study Guide 1Rob Davila100% (2)
- Empty ScrotumDocument36 pagesEmpty ScrotumemirilejlaNo ratings yet
- Session 11 Nur 098Document2 pagesSession 11 Nur 098zyyw.abello.uiNo ratings yet
- Lesson 8 - Fire and EarthQuake PreparednessDocument2 pagesLesson 8 - Fire and EarthQuake Preparednesszyyw.abello.uiNo ratings yet
- Lesson 4-6, Gen 003 Abello, Zydryhc GioDocument6 pagesLesson 4-6, Gen 003 Abello, Zydryhc Giozyyw.abello.uiNo ratings yet
- Activity 5 Sts Adam Joshua A. SaycoDocument1 pageActivity 5 Sts Adam Joshua A. Saycozyyw.abello.uiNo ratings yet
- Answer For Pharma QuizDocument11 pagesAnswer For Pharma Quizzyyw.abello.uiNo ratings yet
- Lesson 7-Mental Health MattersDocument1 pageLesson 7-Mental Health Matterszyyw.abello.uiNo ratings yet
- National Geographic USA - 01 2019Document145 pagesNational Geographic USA - 01 2019Minh ThuNo ratings yet
- Architecture Floor Plan Abbreviations AnDocument11 pagesArchitecture Floor Plan Abbreviations AnGraphitti Koncepts and DesignsNo ratings yet
- Application Registry Edits: Customize Windows Media Player Title BarDocument29 pagesApplication Registry Edits: Customize Windows Media Player Title BarSuseendran SomasundaramNo ratings yet
- Food and Beverages Service: Learning MaterialsDocument24 pagesFood and Beverages Service: Learning MaterialsJoshua CondeNo ratings yet
- Json Cache 1Document5 pagesJson Cache 1Emmanuel AmoahNo ratings yet
- Hacking Web ApplicationsDocument5 pagesHacking Web ApplicationsDeandryn RussellNo ratings yet
- 2010 Christian Religious Education Past Paper - 1Document1 page2010 Christian Religious Education Past Paper - 1lixus mwangiNo ratings yet
- Mora Solvendi (Delay of The Debtor)Document11 pagesMora Solvendi (Delay of The Debtor)John Paul100% (1)
- SriRaghavendra StotraDocument15 pagesSriRaghavendra StotravedanthiNo ratings yet
- Moldavian DressDocument16 pagesMoldavian DressAnastasia GavrilitaNo ratings yet
- Processing, Handling and Storage of Agricultural Product 2Document6 pagesProcessing, Handling and Storage of Agricultural Product 2LittleagleNo ratings yet
- Quality Management in Apparel Industry PDFDocument9 pagesQuality Management in Apparel Industry PDFJyoti Rawal0% (1)
- USA V Brandon Hunt - April 2021 Jury VerdictDocument3 pagesUSA V Brandon Hunt - April 2021 Jury VerdictFile 411No ratings yet
- Wiring Diagram Obp 1 v2Document5 pagesWiring Diagram Obp 1 v2Jorge Luis Vera AlmeidaNo ratings yet
- Masai School Code of Conduct - Prefinal 11.10.2019Document3 pagesMasai School Code of Conduct - Prefinal 11.10.2019xavigatorNo ratings yet
- Petroleum Research: Khalil Shahbazi, Amir Hossein Zarei, Alireza Shahbazi, Abbas Ayatizadeh TanhaDocument15 pagesPetroleum Research: Khalil Shahbazi, Amir Hossein Zarei, Alireza Shahbazi, Abbas Ayatizadeh TanhaLibya TripoliNo ratings yet
- 1967 Painting Israeli VallejoDocument1 page1967 Painting Israeli VallejoMiloš CiniburkNo ratings yet
- Og FMTDocument5 pagesOg FMTbgkinzaNo ratings yet
- Thesis Chapter 123Document15 pagesThesis Chapter 123Chesca Mae PenalosaNo ratings yet
- Common Expressions in Business 2Document2 pagesCommon Expressions in Business 2abdeljelil manelNo ratings yet
- The Definition and Unit of Ionic StrengthDocument2 pagesThe Definition and Unit of Ionic StrengthDiego ZapataNo ratings yet
- Soil Penetrometer ManualDocument4 pagesSoil Penetrometer Manualtag_jNo ratings yet
- Chapter 3 Professional Practices in Nepal ADocument20 pagesChapter 3 Professional Practices in Nepal Amunna smithNo ratings yet
- Ume Mri GuideDocument1 pageUme Mri GuideHiba AhmedNo ratings yet
- Free Easy Autopilot BTC Method 2Document4 pagesFree Easy Autopilot BTC Method 2Adderall 30MG XRNo ratings yet
- Touch TypingDocument49 pagesTouch TypingCris Tin100% (2)
- Student (Mechanical Engineering), JECRC FOUNDATION, Jaipur (2) Assistant Professor, Department of Mechanical Engineering, JECRC FOUNDATION, JaipurDocument7 pagesStudent (Mechanical Engineering), JECRC FOUNDATION, Jaipur (2) Assistant Professor, Department of Mechanical Engineering, JECRC FOUNDATION, JaipurAkash yadavNo ratings yet