You might also like
- Observations on Abortion: Containing an account of the manner in which it is accomplished, the causes which produced it, and the method of preventing or treating itFrom EverandObservations on Abortion: Containing an account of the manner in which it is accomplished, the causes which produced it, and the method of preventing or treating itNo ratings yet
- Placental ExaminationDocument13 pagesPlacental ExaminationAnuradha Maurya50% (2)
- Placenta ExaminationDocument26 pagesPlacenta ExaminationBharat Thapa100% (1)
- Delivery of PlacentaDocument8 pagesDelivery of PlacentaAbdullahi Suleiman MakaNo ratings yet
- Assignment ON PLACENTAL EXAMINATIONDocument4 pagesAssignment ON PLACENTAL EXAMINATIONPriya100% (2)
- Placenta ExaminationDocument18 pagesPlacenta ExaminationAbi RajanNo ratings yet
- Examination of PlacentaDocument15 pagesExamination of PlacentaIrene Territory ChannelNo ratings yet
- Placental ExaminationDocument2 pagesPlacental Examinationsagi mu50% (2)
- Placental Examination: Mrs - Muthulakshmi.C Assistant Professor Department of Obgn Scon, SimatsDocument13 pagesPlacental Examination: Mrs - Muthulakshmi.C Assistant Professor Department of Obgn Scon, SimatsMonika shankar100% (1)
- Examination of PlacentaDocument2 pagesExamination of PlacentaAnju MargaretNo ratings yet
- Placenta ChecklistDocument2 pagesPlacenta ChecklistNidhi Shivam Ahlawat100% (3)
- Umblical Cord AbnormalitiesDocument54 pagesUmblical Cord AbnormalitiesKeerti Patel100% (5)
- Clin TG Abnormalities of The Placenta & CordDocument13 pagesClin TG Abnormalities of The Placenta & CordTami Selvi100% (2)
- Stages of Fetal Growth and DevelopmentDocument10 pagesStages of Fetal Growth and DevelopmentGrant KhangabNo ratings yet
- Placenta & Fetal CirculationDocument32 pagesPlacenta & Fetal CirculationFarxan Da Napolian BwoyNo ratings yet
- The Antenatal Care-Maternal Changes During Pregnancy 7Document75 pagesThe Antenatal Care-Maternal Changes During Pregnancy 795kscbyqxmNo ratings yet
- Research 5Document2 pagesResearch 5api-297205880No ratings yet
- Embryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesDocument13 pagesEmbryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesAudrey100% (5)
- OB Definition of TermsDocument9 pagesOB Definition of TermsWarrenSandovalNo ratings yet
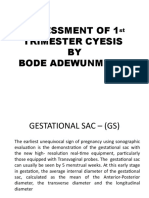
- Assessment of 1ST Trimester CyesisDocument46 pagesAssessment of 1ST Trimester CyesisKEN KIZITONo ratings yet
- Anomalies of The Placenta and The CordDocument38 pagesAnomalies of The Placenta and The CordDN Sly Litang DumangasNo ratings yet
- The Placenta BDocument48 pagesThe Placenta BLulano MbasuNo ratings yet
- Fetal Period PDFDocument40 pagesFetal Period PDFAdvin BurkeNo ratings yet
- ChecklistDocument5 pagesChecklistjoaguilarNo ratings yet
- Abnormalities of Placenta, Amniotic Fluid and Cord: Prepared By, B. Ezhilarasi, Nursing TutorDocument21 pagesAbnormalities of Placenta, Amniotic Fluid and Cord: Prepared By, B. Ezhilarasi, Nursing TutorGopala KrishnanNo ratings yet
- Assessment of PlacentaDocument21 pagesAssessment of PlacentaAarti RajputNo ratings yet
- The Gynaecological ExaminationDocument3 pagesThe Gynaecological ExaminationpogimudaNo ratings yet
- Carnige Stages EmbryologyDocument2 pagesCarnige Stages EmbryologyDark Melanin Fineapple XoXoNo ratings yet
- 2021.2 - Practical Skills Q&ADocument22 pages2021.2 - Practical Skills Q&ALucas Victor AlmeidaNo ratings yet
- ch.8 Embryo PDFDocument22 pagesch.8 Embryo PDFMohammad GhannamNo ratings yet
- Female Pelvis and MeasurementsDocument21 pagesFemale Pelvis and MeasurementsBia KhanNo ratings yet
- Procedure Right Onplacental ExaminationDocument3 pagesProcedure Right Onplacental ExaminationPriyanka SheoranNo ratings yet
- Procedure Right Onplacental ExaminationDocument3 pagesProcedure Right Onplacental ExaminationPriyanka SheoranNo ratings yet
- د.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)Document29 pagesد.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)MohammedNo ratings yet
- PV CasebookDocument2 pagesPV CasebookPreeti ChouhanNo ratings yet
- Fetal Membrane and PlacentaDocument77 pagesFetal Membrane and PlacentaIssa AvenaNo ratings yet
- The Growing Fetus For CPDocument19 pagesThe Growing Fetus For CPyzaNo ratings yet
- Fetal Membranes and PlacentaDocument53 pagesFetal Membranes and PlacentaALFAHRUL CAHYADINo ratings yet
- Placenta: DR Nimco A Hassan Obstetrics and GynaecologyDocument62 pagesPlacenta: DR Nimco A Hassan Obstetrics and GynaecologyMahad Maxamed AxmedNo ratings yet
- Placental Development - Implantation - Transfer - Clinical RelevanceDocument3 pagesPlacental Development - Implantation - Transfer - Clinical RelevanceLiridon SopajNo ratings yet
- 51 Lecture The Gynecological ExamDocument69 pages51 Lecture The Gynecological ExamTarek TarekNo ratings yet
- OB-GYN ExaminationDocument9 pagesOB-GYN ExaminationsalmaNo ratings yet
- Perkembangan Plasenta (Autosaved) .En - IdDocument18 pagesPerkembangan Plasenta (Autosaved) .En - IdFATIMAHNo ratings yet
- The Problem Mare - Clinical PerspectivesDocument9 pagesThe Problem Mare - Clinical PerspectivesLaura RojasNo ratings yet
- Hydra Mi NosDocument8 pagesHydra Mi NosSudha DeviNo ratings yet
- BNS Pregnancy Diagnosis of MareDocument34 pagesBNS Pregnancy Diagnosis of Marevasant kalariya100% (1)
- Assessment of The Breast: Jonalyn Sotero Esco RN., MANDocument41 pagesAssessment of The Breast: Jonalyn Sotero Esco RN., MANVan MaverickNo ratings yet
- CuldocentesisDocument16 pagesCuldocentesisvalerie obehiNo ratings yet
- Parturition, Foetal Membranes and Multiple PregnanciesDocument38 pagesParturition, Foetal Membranes and Multiple PregnanciesGeoffreyNo ratings yet
- Placenta and Placental ProblemsDocument13 pagesPlacenta and Placental ProblemsLuvita Ronteltap100% (1)
- Extraembryonic Mebranes PDFDocument34 pagesExtraembryonic Mebranes PDFJhestine AbayanNo ratings yet
- Umbilical Cord ProlapseDocument6 pagesUmbilical Cord ProlapseJules Cantal100% (3)
- Management of LabourDocument38 pagesManagement of LabourAnjali Rahul AjmeriNo ratings yet
- OSCE On 14/3/2008: Describe Gynaecoid PelvisDocument82 pagesOSCE On 14/3/2008: Describe Gynaecoid PelvisKahing LiNo ratings yet
- Basics of UltrasoundDocument55 pagesBasics of UltrasoundDrChauhan100% (2)
- Midwifery Revision Questions-1Document8 pagesMidwifery Revision Questions-1kariuki90406978No ratings yet
- Rabbit Spay and Neuter TechniquesDocument4 pagesRabbit Spay and Neuter TechniquesSebastián Ordóñez RamírezNo ratings yet
- PlacentaDocument11 pagesPlacentasubashikNo ratings yet
- Bovine Reproduction Booklet UK A5 16pp Text 10Document20 pagesBovine Reproduction Booklet UK A5 16pp Text 10lenn chandNo ratings yet
- PlacentaDocument24 pagesPlacentaNibedita 2015No ratings yet
- Admit Card-NOWE 2023Document3 pagesAdmit Card-NOWE 2023Kuleshwar SahuNo ratings yet
- A Front Pages ResearchDocument11 pagesA Front Pages ResearchKuleshwar SahuNo ratings yet
- CH 4,5,6 FINALDocument36 pagesCH 4,5,6 FINALKuleshwar SahuNo ratings yet
- Part5MCQSpecialQuestionPDF 14991 14991 1802003Document3 pagesPart5MCQSpecialQuestionPDF 14991 14991 1802003Kuleshwar SahuNo ratings yet
- GLOSSARYDocument1 pageGLOSSARYKuleshwar SahuNo ratings yet
- A Front Pages ResearchDocument1 pageA Front Pages ResearchKuleshwar SahuNo ratings yet
- CH 2Document17 pagesCH 2Kuleshwar SahuNo ratings yet
- VapsiDocument3 pagesVapsiKuleshwar SahuNo ratings yet
- OncologyDPP 13038 12074 1345119Document4 pagesOncologyDPP 13038 12074 1345119Kuleshwar SahuNo ratings yet
- Corrigendum Notice: King George Medical University Lucknow Nursing Officers Recruitment Examination 2023Document2 pagesCorrigendum Notice: King George Medical University Lucknow Nursing Officers Recruitment Examination 2023Kuleshwar SahuNo ratings yet
- MusculoskeletalSystemDPP 13038 12074 1345120Document8 pagesMusculoskeletalSystemDPP 13038 12074 1345120Kuleshwar SahuNo ratings yet
- 2.uterine AbnormalitiesDocument11 pages2.uterine AbnormalitiesKuleshwar SahuNo ratings yet
- Tickets Raipur - PyjDocument3 pagesTickets Raipur - PyjKuleshwar SahuNo ratings yet
- 400 881 1 SMDocument11 pages400 881 1 SMroloheNo ratings yet
- 32OR Set2Document4 pages32OR Set2Niraj BhansaliNo ratings yet
- Total Total Total Tota L Total Total Total Total Total T-Score T - Score T - Scor e T - Score T - Score T - Score T - Score T - ScoreDocument2 pagesTotal Total Total Tota L Total Total Total Total Total T-Score T - Score T - Scor e T - Score T - Score T - Score T - Score T - Scorethelegend 2022No ratings yet
- Mou (Nickel)Document16 pagesMou (Nickel)MANOJ PANNASENo ratings yet
- The Verb TO BE (Affirmative - Negative) in Simple PresentDocument2 pagesThe Verb TO BE (Affirmative - Negative) in Simple PresentEisya AbdullahNo ratings yet
- RA 8371 Key PointsDocument6 pagesRA 8371 Key PointsKristine DiamanteNo ratings yet
- Vuyo's Funerals: Social Media Post (Funeral Rituals)Document2 pagesVuyo's Funerals: Social Media Post (Funeral Rituals)LCNo ratings yet
- Business LetterDocument4 pagesBusiness LetterEli Abram Dini-ay CabilinNo ratings yet
- Endodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda SahaDocument6 pagesEndodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda Sahanovia chantikaNo ratings yet
- BC548 - Datashet PDFDocument2 pagesBC548 - Datashet PDFBraian KonzgenNo ratings yet
- Biography of 16th Karmapa and 3d Jamgon KongtrulDocument16 pagesBiography of 16th Karmapa and 3d Jamgon KongtrulSergey SergeyNo ratings yet
- Texto para Discussão: Departamento de EconomiaDocument43 pagesTexto para Discussão: Departamento de EconomiaAna ScaletNo ratings yet
- Bservation of A Commonplace Phenomenon,: Theory of Vortex SoundDocument19 pagesBservation of A Commonplace Phenomenon,: Theory of Vortex SoundQianZHNo ratings yet
- Agency QuestionnaireDocument5 pagesAgency QuestionnaireUlaine Gayle EsnaraNo ratings yet
- Manonmaniam Sundaranar University Tirunelveli-12 FOR THE YEAR 2016 - 2017Document10 pagesManonmaniam Sundaranar University Tirunelveli-12 FOR THE YEAR 2016 - 2017David MillerNo ratings yet
- BGS, ViDocument13 pagesBGS, ViBla& BlaNo ratings yet
- Discipline and Ideas in Applied Social Science Quarter 1 - Module 5: The Clientele and Audiences in Counseling and The Counseling ProcessesDocument17 pagesDiscipline and Ideas in Applied Social Science Quarter 1 - Module 5: The Clientele and Audiences in Counseling and The Counseling ProcessesBenilda Pensica SevillaNo ratings yet
- The Human Self and The Divine SelfDocument2 pagesThe Human Self and The Divine SelfPatricia Laura Kenney100% (2)
- Mirza Ghalib - Poems - 2Document5 pagesMirza Ghalib - Poems - 2Navdeep GillNo ratings yet
- Top 50 Russophobe Myths - Anatoly KarlinDocument29 pagesTop 50 Russophobe Myths - Anatoly KarlinLevantineANo ratings yet
- Basic Immunology PDFDocument6 pagesBasic Immunology PDFAnastasia ENo ratings yet
- 22 23 34Document20 pages22 23 34anilmathew244No ratings yet
- Toddle 034dff16 035b 4364 b371 6ec2a3cdedd7 Edited Eye of The Wolf InsertDocument2 pagesToddle 034dff16 035b 4364 b371 6ec2a3cdedd7 Edited Eye of The Wolf Insertamogh vorugantiNo ratings yet
- Specific Features of The Decathlon PDFDocument5 pagesSpecific Features of The Decathlon PDFBrandy MaloneNo ratings yet
- Book - Python - Hands-On Simulation Model PythonDocument347 pagesBook - Python - Hands-On Simulation Model PythonKiều Nhi Nguyễn100% (3)
- Thesis MelsonDocument160 pagesThesis MelsonVincent CucumazzøNo ratings yet
- Book Blast 23 June 2023Document2 pagesBook Blast 23 June 2023ionaNo ratings yet
- Davao Sawmill v. CastilloDocument1 pageDavao Sawmill v. CastilloJulie AnnNo ratings yet
- MODULE-4 Life and Works of Rizal For SDocument12 pagesMODULE-4 Life and Works of Rizal For SKyle CuiNo ratings yet
- Wix Singular and PluralDocument9 pagesWix Singular and PluralbashayerNo ratings yet