You might also like
- The Molecular Biology of Cancer: A Bridge from Bench to BedsideFrom EverandThe Molecular Biology of Cancer: A Bridge from Bench to BedsideStella PelengarisNo ratings yet
- Oeq 3Document6 pagesOeq 3Sara JosephNo ratings yet
- BSR Supertrans Block 2Document9 pagesBSR Supertrans Block 2Mavic VillanuevaNo ratings yet
- Neoplasia Summer 2020Document38 pagesNeoplasia Summer 2020Sharif HossainNo ratings yet
- Diagnóstico Integral Del Cáncer Clases 2-3Document5 pagesDiagnóstico Integral Del Cáncer Clases 2-3Nerea OteguiNo ratings yet
- Cancer Genetics and GenomesDocument98 pagesCancer Genetics and GenomesAnonymous HNTNhspNo ratings yet
- Kanker 1Document30 pagesKanker 1agengbsNo ratings yet
- 13 GMppt-chapter16-2019 (Ok)Document17 pages13 GMppt-chapter16-2019 (Ok)Kw ChanNo ratings yet
- Abeloff Clinical Oncology 2020 (Part 1)Document22 pagesAbeloff Clinical Oncology 2020 (Part 1)Emiliana LarionesiNo ratings yet
- Cc2 - MidtermDocument3 pagesCc2 - MidtermMika SusadaNo ratings yet
- Principles of OncologyDocument81 pagesPrinciples of OncologyAbidisHereNo ratings yet
- Tumour Immunology: Von Ryan F. Lingcallo, RMTDocument20 pagesTumour Immunology: Von Ryan F. Lingcallo, RMTJuan SalenNo ratings yet
- Unit 3 Chapter 9 DNA-Based Technologies LectureDocument20 pagesUnit 3 Chapter 9 DNA-Based Technologies LectureNeedBooksDontSueNo ratings yet
- Neuroblastoma: Biological Insights Into A Clinical Enigma: Garrett M. BrodeurDocument14 pagesNeuroblastoma: Biological Insights Into A Clinical Enigma: Garrett M. BrodeurMouris DwiputraNo ratings yet
- Tema 4Document13 pagesTema 4Nerea OteguiNo ratings yet
- Method 1: Gene Mapping - Definition: Gene Mapping Refers To The Process of Determining The Location of Genes OnDocument7 pagesMethod 1: Gene Mapping - Definition: Gene Mapping Refers To The Process of Determining The Location of Genes OnYến NguyễnNo ratings yet
- OnkologieDocument41 pagesOnkologieNatz BatzNo ratings yet
- Sensetivity of Karyotyping and MicroarrayDocument5 pagesSensetivity of Karyotyping and MicroarrayDr Ahmed Al AmriNo ratings yet
- Chapter 16-JnuCancer - 複本Document42 pagesChapter 16-JnuCancer - 複本Wai Kwong ChiuNo ratings yet
- Uterin Sarcoma - MolecularDocument15 pagesUterin Sarcoma - MolecularDoctor LifeNo ratings yet
- Genetics of CancerDocument64 pagesGenetics of CancerErin HillNo ratings yet
- Detection of Mutations in EGFR in Circulating Lung-Cancer Cells.Document12 pagesDetection of Mutations in EGFR in Circulating Lung-Cancer Cells.Joonseok ParkNo ratings yet
- Bisc 3150 General Pathology: Neoplasia Wednesday, January 31, 2018 Friday, February 2, 2018 Judy Maloney, PHDDocument62 pagesBisc 3150 General Pathology: Neoplasia Wednesday, January 31, 2018 Friday, February 2, 2018 Judy Maloney, PHDEvan PfeiferNo ratings yet
- Profound Tissue Specifity in Proliferation Control Underlies Cancer Drivers and Aneuploidy PatternsDocument40 pagesProfound Tissue Specifity in Proliferation Control Underlies Cancer Drivers and Aneuploidy PatternsDAYANA ERAZONo ratings yet
- Roylance 1997Document8 pagesRoylance 1997barti koksNo ratings yet
- 212F - Oncology L1 - 2104Document25 pages212F - Oncology L1 - 2104Tyler LiuNo ratings yet
- Mutational Landscape of Cancer-Driver Genes Across Human CancersDocument14 pagesMutational Landscape of Cancer-Driver Genes Across Human CancersbiolabpartnerNo ratings yet
- Chapter 7 - NeoplasiaDocument23 pagesChapter 7 - NeoplasiaAgnieszka WisniewskaNo ratings yet
- Tugas DR KamalDocument7 pagesTugas DR KamalZarin SafanahNo ratings yet
- Is Module 8Document26 pagesIs Module 8gladyskheyagamNo ratings yet
- Neoplasms What Is A Tumor? ClonalityDocument2 pagesNeoplasms What Is A Tumor? ClonalityRosey WhtNo ratings yet
- 2012 - Intra-Tumour Heterogeneity - A Looking Glass For CancerDocument12 pages2012 - Intra-Tumour Heterogeneity - A Looking Glass For CancerFreddy A. ManayayNo ratings yet
- Genetics, Reproduction & Female HealthcareDocument30 pagesGenetics, Reproduction & Female Healthcareronwest1990No ratings yet
- Angiogenesis and Metastasis 10.11 - ColourDocument7 pagesAngiogenesis and Metastasis 10.11 - Colourboffin2rulezNo ratings yet
- Cytogenetic Analysis in The Diagnosis of Acute Leukemia: Sverre Heim, FelixDocument9 pagesCytogenetic Analysis in The Diagnosis of Acute Leukemia: Sverre Heim, FelixEnas KharbotlyNo ratings yet
- Thursday, 3 November 2022 10:14 PMDocument5 pagesThursday, 3 November 2022 10:14 PMAdiel CalsaNo ratings yet
- Chapter 1 - The Cancer GenomeDocument35 pagesChapter 1 - The Cancer GenomeCynthia LopesNo ratings yet
- C & M Bio CancerDocument32 pagesC & M Bio CancerA PNo ratings yet
- Biology of Cancer Exam 1 Study GuideDocument13 pagesBiology of Cancer Exam 1 Study GuidesahilaminNo ratings yet
- Review: Tumor Markers in Clinical OncologyDocument11 pagesReview: Tumor Markers in Clinical OncologySergio Rodríguez MolinaNo ratings yet
- 8 Cancer Stem Cells Basic Concepts and Therapeutic ImplicationsDocument29 pages8 Cancer Stem Cells Basic Concepts and Therapeutic Implicationsrihamazim2018No ratings yet
- M5 BIO111 Assignment1Document7 pagesM5 BIO111 Assignment1Kyle DunnNo ratings yet
- Shlien 2010 A Comon Molecular Mechanism Underlies 17p13Document12 pagesShlien 2010 A Comon Molecular Mechanism Underlies 17p13Katherine Lemus SepúlvedaNo ratings yet
- NehaDocument91 pagesNehaPawan MeenaNo ratings yet
- Cybulska 2019Document8 pagesCybulska 2019ZULMA MADELINE LIBNY GUTARRA TICANo ratings yet
- Serological Tests For Cancer DetectionDocument22 pagesSerological Tests For Cancer DetectionShreeyaNo ratings yet
- BM 8-9 OncogenesisDocument139 pagesBM 8-9 OncogenesisabdullahshiddiqadamNo ratings yet
- Are Ad 041Document26 pagesAre Ad 041brnrNo ratings yet
- Dinosaurs Before DarkDocument9 pagesDinosaurs Before DarkIna SimacheNo ratings yet
- Neoplasia: Benito K. Lim Hong III, M.DDocument51 pagesNeoplasia: Benito K. Lim Hong III, M.DGokul PoudelNo ratings yet
- Hematolrep 03 E2 v2Document3 pagesHematolrep 03 E2 v2772450336No ratings yet
- Methods For Detecting Mutations Types of InheritanceDocument16 pagesMethods For Detecting Mutations Types of InheritanceRinkiNo ratings yet
- 13 ChemoDocument40 pages13 ChemoSweet SunNo ratings yet
- Bases Moleculares Del CáncerDocument15 pagesBases Moleculares Del Cáncerkarina morenoNo ratings yet
- 1 s2.0 S0304383523000083 MainDocument9 pages1 s2.0 S0304383523000083 MainMericia Guadalupe Sandoval ChavezNo ratings yet
- Li Et Al. 2022 - Untangling The Web of Intratumour HeterogeneityDocument10 pagesLi Et Al. 2022 - Untangling The Web of Intratumour HeterogeneitysodiogoesNo ratings yet
- Neoplasia: Dr. Dyah Marianingrum Mkes, SP - PADocument35 pagesNeoplasia: Dr. Dyah Marianingrum Mkes, SP - PANdari DyaekaNo ratings yet
- Principles of Clinical CytogeneticsDocument34 pagesPrinciples of Clinical CytogeneticsZainab Jamal SiddiquiNo ratings yet
- Mutagen, Karsinogen Dan Karsinogenesis: DR. Muhammad Da'i, M.Si., AptDocument37 pagesMutagen, Karsinogen Dan Karsinogenesis: DR. Muhammad Da'i, M.Si., ApthafidzNo ratings yet
- Cancer Pathophysiology Nursing NotesDocument8 pagesCancer Pathophysiology Nursing Notesgrad_nurse_2015100% (2)
- Lectura S3.2. Benign and Malignant Lesions of The Stomach - Evaluation of CT Criteria For DifferentiationDocument6 pagesLectura S3.2. Benign and Malignant Lesions of The Stomach - Evaluation of CT Criteria For DifferentiationJohnattan Javier Espinoza CastañedaNo ratings yet
- WEEK 8 CHAPTER 3-SUFFIXES p1Document21 pagesWEEK 8 CHAPTER 3-SUFFIXES p1rahafNo ratings yet
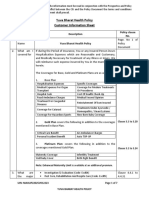
- CIS Yuva Bharat Health PolicyDocument7 pagesCIS Yuva Bharat Health PolicyS PNo ratings yet
- Table of Surgical)Document98 pagesTable of Surgical)Bilal AhmadNo ratings yet
- 2 Diseases of The BreastDocument109 pages2 Diseases of The Breastrere choiNo ratings yet
- Sact Passport Final Aug 2020Document68 pagesSact Passport Final Aug 2020ryze.ahmedNo ratings yet
- Vet Comparative Oncology - 2022 - Smedley - Diagnosis and Histopathologic Prognostication of Canine Melanocytic NeoplasmsDocument13 pagesVet Comparative Oncology - 2022 - Smedley - Diagnosis and Histopathologic Prognostication of Canine Melanocytic NeoplasmsDaniela Angel CortesNo ratings yet
- Cancer Answer Sheet PDFDocument2 pagesCancer Answer Sheet PDFamandeep251702No ratings yet
- 57-2-3 BiologyDocument19 pages57-2-3 BiologyRavneet KaurNo ratings yet
- Health 7 4th Quarter LasDocument17 pagesHealth 7 4th Quarter Lassarah jane ocenar100% (2)
- BF LosaDocument32 pagesBF LosaTEMOCATIANo ratings yet
- General Basis of Pathologic ConditionDocument24 pagesGeneral Basis of Pathologic Conditionallexa jimlaniNo ratings yet
- C Is New India Floater Medi Claim PolicyDocument12 pagesC Is New India Floater Medi Claim PolicyDeepan ManojNo ratings yet
- Chest Wall Tumors - Saad HamwiehDocument31 pagesChest Wall Tumors - Saad HamwiehKhaled AlshoufiNo ratings yet
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocument9 pages2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangNo ratings yet
- (10920684 - Neurosurgical Focus) Factors Associated With Survival in Patients With MeningiomaDocument17 pages(10920684 - Neurosurgical Focus) Factors Associated With Survival in Patients With MeningiomaDarlene LebasteNo ratings yet
- PSMA in Seminal Vesicle AmyloidDocument2 pagesPSMA in Seminal Vesicle AmyloidGaurav MalhotraNo ratings yet
- 8 Lacrimal Drainage System Diseases by James PMDocument63 pages8 Lacrimal Drainage System Diseases by James PMCharles AntonyNo ratings yet
- Poster Paper Foo Kota Bengkulu NewDocument1 pagePoster Paper Foo Kota Bengkulu NewPoppy WulandariNo ratings yet
- Math IA FinalDocument33 pagesMath IA FinalPratham ChopraNo ratings yet
- OncologyDocument3 pagesOncologyMichtropolisNo ratings yet
- Spiritual - Science.and - Medicine.GA312.Lecture XIVDocument12 pagesSpiritual - Science.and - Medicine.GA312.Lecture XIVtomNo ratings yet
- Brain Tumors - KY Cancer RegistryDocument45 pagesBrain Tumors - KY Cancer RegistryMohammad Galih PratamaNo ratings yet
- 2.7 Cell Division Going Wrong - Cancer PDFDocument8 pages2.7 Cell Division Going Wrong - Cancer PDFAntoline Natasha RayappanNo ratings yet
- Pathology Course Audit-3Document26 pagesPathology Course Audit-3Joana Marie PalatanNo ratings yet
- Major Project ReportDocument62 pagesMajor Project ReportRashmithaNo ratings yet
- Profile-Of-Neuron SutomoDocument4 pagesProfile-Of-Neuron Sutomodini kusmaharaniNo ratings yet
- Role of Mother Tincture in OncologyDocument4 pagesRole of Mother Tincture in OncologyEditor IJTSRD100% (1)
- Tumour MarkersDocument34 pagesTumour MarkersAbdulelah MurshidNo ratings yet
- PYQ Patho MPMSU MBBSDocument20 pagesPYQ Patho MPMSU MBBSShahzaib Gouri100% (1)