You might also like
- ICU Hospital Assessment Form State Life V2Document4 pagesICU Hospital Assessment Form State Life V2Anwar Pervaiz PervaizNo ratings yet
- PICU Hospital Assessment Form State Life V3Document4 pagesPICU Hospital Assessment Form State Life V3Anwar Pervaiz PervaizNo ratings yet
- NicuDocument4 pagesNicuAnwar Pervaiz PervaizNo ratings yet
- Deluxe & Above /others - Single Room A/C Sharing / Single Non A/c General Ward / Multi SharingDocument13 pagesDeluxe & Above /others - Single Room A/C Sharing / Single Non A/c General Ward / Multi SharingSanket SahareNo ratings yet
- Abdomen X RayDocument4 pagesAbdomen X RaytimvrghsNo ratings yet
- Recent Final Frca Vascular Anaesthesia QuestionsDocument4 pagesRecent Final Frca Vascular Anaesthesia Questionslim sjNo ratings yet
- Spec Sheet Dharmais-FujiDocument36 pagesSpec Sheet Dharmais-FujiRendy Syauqy HasanNo ratings yet
- Do We Still Need A Stethoscope - Stats For Top 10 Cardiac Tests - Roland SabbaghDocument45 pagesDo We Still Need A Stethoscope - Stats For Top 10 Cardiac Tests - Roland SabbaghJason WongNo ratings yet
- FPSC No: 55 Mcqs On Submission Deadline: 19 November 2013 12 NoonDocument4 pagesFPSC No: 55 Mcqs On Submission Deadline: 19 November 2013 12 Noonhassanmurtazashah33No ratings yet
- Competition Scenario TemplateDocument2 pagesCompetition Scenario TemplatePCHANFANNo ratings yet
- Standardized Methods For Measuring Diagnostic X-Ray ExposuresDocument26 pagesStandardized Methods For Measuring Diagnostic X-Ray Exposuresmohadese EstajiNo ratings yet
- WPS Medicare IndexDocument14 pagesWPS Medicare IndexbkprodhNo ratings yet
- 7 Series (Radiology) : X-Ray Coding PointsDocument7 pages7 Series (Radiology) : X-Ray Coding PointsVijay UNo ratings yet
- PACS QuestionnaireDocument4 pagesPACS QuestionnaireakashniranjaneNo ratings yet
- Önemli ECLS Registry FormDocument9 pagesÖnemli ECLS Registry Formyowewe7363No ratings yet
- ACLS Recerti Cation Exam Quiz: (/my-Account/)Document6 pagesACLS Recerti Cation Exam Quiz: (/my-Account/)andres novoaNo ratings yet
- Probe Selection Machine Controls Equipment MGHillDocument14 pagesProbe Selection Machine Controls Equipment MGHilljohnalanNo ratings yet
- Radiology Exercises 08022013Document3 pagesRadiology Exercises 08022013anishrove2No ratings yet
- Cotabato Regional and Medical Center Diagnostic Procedures Stat/Requested Done at Emergency RoomDocument1 pageCotabato Regional and Medical Center Diagnostic Procedures Stat/Requested Done at Emergency RoomSeychelle DucusinNo ratings yet
- Multislice CT of The Abdomen PDFDocument11 pagesMultislice CT of The Abdomen PDFnguyenNo ratings yet
- Why TR-PintaricDocument55 pagesWhy TR-PintaricHrvojeNo ratings yet
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- National Accreditation Board For Hospitals and Health Care Providers - Quality Council of IndiaDocument21 pagesNational Accreditation Board For Hospitals and Health Care Providers - Quality Council of IndiashrithyNo ratings yet
- Safety Code 35 Talk Rps Feb 200976109Document34 pagesSafety Code 35 Talk Rps Feb 200976109ahmed_galal_waly1056No ratings yet
- Cardiology Department: Iccu and WardsDocument12 pagesCardiology Department: Iccu and WardsPoojaNo ratings yet
- Euroscore IiDocument5 pagesEuroscore IiYadira SantosNo ratings yet
- Check List For SNCUDocument5 pagesCheck List For SNCUpriyahospitalNo ratings yet
- 6519 2011bme 502 (5115) PDFDocument4 pages6519 2011bme 502 (5115) PDFNoor AhmedNo ratings yet
- 6519 2011bme 502 (5115) PDFDocument4 pages6519 2011bme 502 (5115) PDFNoor AhmedNo ratings yet
- CardiothoracicsurgicallogbookrevisedDocument8 pagesCardiothoracicsurgicallogbookrevisedprofarmah6150No ratings yet
- 2011 Appendix A UpdatesDocument65 pages2011 Appendix A UpdatesfaithNo ratings yet
- Body CT - Chest HRCTDocument5 pagesBody CT - Chest HRCTKelum BuddhikaNo ratings yet
- Brivo CT385 GEHW E-CatalogDocument1 pageBrivo CT385 GEHW E-CatalogHarry Febryanto100% (1)
- Spesifikasi Philips AZURION 7 M12-M20 ADVANCEDDocument3 pagesSpesifikasi Philips AZURION 7 M12-M20 ADVANCEDRSUD SLGNo ratings yet
- Cheklist Keamanan InsisiDocument1 pageCheklist Keamanan InsisiRiska AsafitriNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Body CT - Pancreas 3 Phase PelvisDocument5 pagesBody CT - Pancreas 3 Phase PelvisHeriNo ratings yet
- Icd 9 CM (Tabulasi) 2012Document263 pagesIcd 9 CM (Tabulasi) 2012M Taufik Harahap100% (1)
- Current Techniques in Canine and Feline NeurosurgeryFrom EverandCurrent Techniques in Canine and Feline NeurosurgeryAndy ShoresNo ratings yet
- Spec ACUSON Juniper CV - FinalDocument1 pageSpec ACUSON Juniper CV - FinalBenny SNo ratings yet
- Clinical Audit On Code BlueDocument7 pagesClinical Audit On Code BlueSunny AnthonyNo ratings yet
- Field Descriptions For Patient and Treatment CharacteristicsDocument2 pagesField Descriptions For Patient and Treatment Characteristicsrenesouza.odontoNo ratings yet
- Clinical Service AreasDocument4 pagesClinical Service AreasR SheeNo ratings yet
- Updated Pmjay List-1Document10,143 pagesUpdated Pmjay List-1Siddhant SinghNo ratings yet
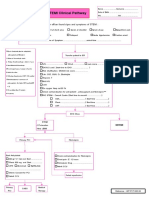
- STEMI Clinical PathwayDocument1 pageSTEMI Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- Emergency Radiology With QuizDocument115 pagesEmergency Radiology With QuizAndre PrawiradinataNo ratings yet
- Procedure ChargesDocument5 pagesProcedure ChargesSyed RuksarNo ratings yet
- Free Radiography Test and The ARRT WheelDocument37 pagesFree Radiography Test and The ARRT WheelEskadmas Belay100% (1)
- Spesifikasi Artis Icono BiplaneDocument2 pagesSpesifikasi Artis Icono Biplanerahmatsutanpangulu100% (1)
- Imaging Protocol of ChestDocument11 pagesImaging Protocol of ChestAsmita BhattNo ratings yet
- Spesifikasi ACUSON SC2000 EchocardiographyDocument2 pagesSpesifikasi ACUSON SC2000 EchocardiographyRizki Try AtmantiNo ratings yet
- ADEM Aortic-Diseases 2014Document12 pagesADEM Aortic-Diseases 2014Wayan GunawanNo ratings yet
- Schedule of Charges-Holy Family - Sep 08Document64 pagesSchedule of Charges-Holy Family - Sep 08Quirinevv100% (1)
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- Artigo - Valve Heart Surgery in BrazilDocument12 pagesArtigo - Valve Heart Surgery in BrazilRBonrukNo ratings yet
- Application Form For HospitalDocument5 pagesApplication Form For HospitalRhodora BenipayoNo ratings yet
- Bedside Ultrasound: Level 1 - Second EditionFrom EverandBedside Ultrasound: Level 1 - Second EditionRating: 5 out of 5 stars5/5 (1)
- Body CT - Liver 4 Phase PelvisDocument5 pagesBody CT - Liver 4 Phase PelvisppgpcsNo ratings yet
- Clinical Applications: Syngo Vessel ViewDocument8 pagesClinical Applications: Syngo Vessel ViewMarwan Al-ShaikhliNo ratings yet
- Resuscitation Volume 78 Issue 3 2008Document10 pagesResuscitation Volume 78 Issue 3 2008Abhishek jNo ratings yet
- Sonos Outdoor by Sonance Installation ManualDocument4 pagesSonos Outdoor by Sonance Installation Manualvlad111No ratings yet
- PNAPDocument79 pagesPNAPYu chung yinNo ratings yet
- Literature Review Topics RadiographyDocument8 pagesLiterature Review Topics Radiographyea7w32b0100% (1)
- Benjamin Gomez v. Enrico PalomarDocument11 pagesBenjamin Gomez v. Enrico PalomarUlyung DiamanteNo ratings yet
- Reading 40 Introduction To Industry and Company AnalysisDocument23 pagesReading 40 Introduction To Industry and Company AnalysisNeerajNo ratings yet
- AY2017 2018CourseworkFees MOEDocument22 pagesAY2017 2018CourseworkFees MOEYotrisno LangNo ratings yet
- Adding Rows Dynamically in A Table Using Interactive Adobe FormsDocument5 pagesAdding Rows Dynamically in A Table Using Interactive Adobe Formsbharath_sajjaNo ratings yet
- Sokkia MagnetDocument9 pagesSokkia Magnetbbutros_317684077No ratings yet
- H2S Personal Gas MonitorDocument14 pagesH2S Personal Gas Monitormaher mansiNo ratings yet
- Level 5 Part 1: Listening Comprehension (V.9) : Nro. de Control: ......Document16 pagesLevel 5 Part 1: Listening Comprehension (V.9) : Nro. de Control: ......Maco cacoseNo ratings yet
- m5q3w2 Las 4Document5 pagesm5q3w2 Las 4ronaldNo ratings yet
- Catalogue For TubingDocument1 pageCatalogue For Tubingprabhakaran.cNo ratings yet
- Server Preparation Details LinuxDocument9 pagesServer Preparation Details Linuxbharatreddy9No ratings yet
- 3.3 Motherboard SchematicsDocument49 pages3.3 Motherboard SchematicsJoanna WęgielNo ratings yet
- Multiple Choice Questions: This Activity Contains 15 QuestionsDocument4 pagesMultiple Choice Questions: This Activity Contains 15 QuestionsRaman Kulkarni100% (1)
- Nasser Al AmryDocument31 pagesNasser Al AmrymohamadNo ratings yet
- 05 N141 31673Document21 pages05 N141 31673priya thakurNo ratings yet
- Forward Planning DocumentDocument24 pagesForward Planning Documentapi-396981495No ratings yet
- A New Approach To Air Quality in Hospitals: Www.p3italy - ItDocument19 pagesA New Approach To Air Quality in Hospitals: Www.p3italy - ItMuneer Ahmed ShaikNo ratings yet
- Nursing Education Field TripDocument5 pagesNursing Education Field TripIshika Roy67% (3)
- Procreate GuideDocument283 pagesProcreate GuideDiego D'Andrea100% (2)
- Bridge Operation Maintenance COWIDocument19 pagesBridge Operation Maintenance COWIAhmadKhattabNo ratings yet
- Name - ESM 2104 Sample Final ExamDocument7 pagesName - ESM 2104 Sample Final ExamCOCO12432345No ratings yet
- 04.1 Foreign Graduates1Document30 pages04.1 Foreign Graduates1Frederico CavalcanteNo ratings yet
- GIS Unit 2 Class TestDocument7 pagesGIS Unit 2 Class TestPrathamesh BhosaleNo ratings yet
- WINTER 2023 Course Outline: ENME 479 Mechanics of Deformable Bodies IIDocument8 pagesWINTER 2023 Course Outline: ENME 479 Mechanics of Deformable Bodies IIKai McDermottNo ratings yet
- CN Mod1 Ppt-FinalDocument56 pagesCN Mod1 Ppt-FinalkkNo ratings yet
- PATMD-LW Series Trifold 20200212Document2 pagesPATMD-LW Series Trifold 20200212Taacsa MatrizNo ratings yet
- Certificate of Software AcceptanceDocument6 pagesCertificate of Software AcceptanceVince PepañaNo ratings yet
- 08 LCD Slide Handout 1Document5 pages08 LCD Slide Handout 1Jana Gabrielle Canonigo0% (1)