You might also like
- How Do Humans Breathe? Science Book Age 8 | Children's Biology BooksFrom EverandHow Do Humans Breathe? Science Book Age 8 | Children's Biology BooksNo ratings yet
- Respiration NotesDocument4 pagesRespiration NotesJana AldourNo ratings yet
- Chap 12 RespirationDocument48 pagesChap 12 RespirationFungai MuganhuNo ratings yet
- Breathing and Exchange of GasesDocument5 pagesBreathing and Exchange of Gaseslpc4944No ratings yet
- Breathing and RespirationDocument30 pagesBreathing and Respirationhamzahazard527No ratings yet
- Gas Exchange Notes ExplainedDocument6 pagesGas Exchange Notes ExplainedKai TongNo ratings yet
- Respiratory SystemDocument6 pagesRespiratory SystemCraigNo ratings yet
- Respiratory System: Dr. Agung Kurniawan, MkesDocument31 pagesRespiratory System: Dr. Agung Kurniawan, MkesJojo BodhoNo ratings yet
- BREATHING & GASES EXCHANGEDocument7 pagesBREATHING & GASES EXCHANGEKankana Biswas100% (1)
- Respiratory SystemDocument7 pagesRespiratory SystemNgenyi ChiarittaNo ratings yet
- Respiratory System VocabularyDocument9 pagesRespiratory System VocabularyAgustín Bravo ArreyesNo ratings yet
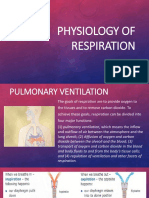
- Physiology of RespirationDocument26 pagesPhysiology of Respirationrevaniwati100% (1)
- Theory of LungDocument7 pagesTheory of LungAndres Dario R LozNo ratings yet
- 11 Biology Notes ch17-pdf1Document9 pages11 Biology Notes ch17-pdf1LishaNo ratings yet
- CBSE Quick Revision Notes on Breathing and Exchange of GasesDocument4 pagesCBSE Quick Revision Notes on Breathing and Exchange of GasesParimala deviNo ratings yet
- Gas ExchangeDocument6 pagesGas Exchangerasha nadaNo ratings yet
- Breathing and Exchange of GasesDocument8 pagesBreathing and Exchange of GasesgoswamiuwuNo ratings yet
- Gas Exchange NewDocument30 pagesGas Exchange Newmariaamkhaann22No ratings yet
- Human Respiratory System ExplainedDocument4 pagesHuman Respiratory System ExplainedSheehan MathurNo ratings yet
- BIO 2701 Lecture Notes Exchange With The EnvironmentDocument11 pagesBIO 2701 Lecture Notes Exchange With The EnvironmentDorothy MayakaNo ratings yet
- Respiratory System 8Document32 pagesRespiratory System 8Naanmatha PuspanathanNo ratings yet
- Dr. Sunita Saxena - Breathing and Exchange of GassesDocument48 pagesDr. Sunita Saxena - Breathing and Exchange of GassesDivya AgarawalNo ratings yet
- The Respiratory System or Pulmonary SystemDocument53 pagesThe Respiratory System or Pulmonary Systemfharidaismail47No ratings yet
- The Respiratory SystemDocument2 pagesThe Respiratory SystemconnievelardeNo ratings yet
- Biology Notes - Respiratory SystemDocument9 pagesBiology Notes - Respiratory SystemnoorbdeirNo ratings yet
- Gaseous ExchangeDocument37 pagesGaseous ExchangeSolángé MirembeNo ratings yet
- Respiratory System OkDocument36 pagesRespiratory System Okakselerasi10No ratings yet
- BreathingDocument5 pagesBreathingvictory IsaacNo ratings yet
- Anatomy and Physiology of Animals-121-150Document30 pagesAnatomy and Physiology of Animals-121-150Pavan PatilNo ratings yet
- Human Respiratory SystemDocument13 pagesHuman Respiratory SystemJue Hazea GoldshopNo ratings yet
- Gas Exchange in the Lungs: Oxygen Absorption and Carbon Dioxide ReleaseDocument23 pagesGas Exchange in the Lungs: Oxygen Absorption and Carbon Dioxide ReleaseVNo ratings yet
- Anaphy Lab ReviewerDocument12 pagesAnaphy Lab ReviewerCamille ParedesNo ratings yet
- Breathing and gas exchangeDocument10 pagesBreathing and gas exchangeramakant chobheNo ratings yet
- Reflection Respiratory SystemDocument4 pagesReflection Respiratory SystemAin Sufiza0% (1)
- For Other Uses, See - "Lunged" Redirects Here. For Other Uses, SeeDocument12 pagesFor Other Uses, See - "Lunged" Redirects Here. For Other Uses, Seefifa92_piscesNo ratings yet
- Notes of Human Physiology Class 11Document9 pagesNotes of Human Physiology Class 11ADWAITH LALUNo ratings yet
- Module 2: Respiratory System SEM 2 SESI 2019/2020 Group: A: Name: Mohamad Aiman Iqbal Bin Nordin MATRIC NO: D20192091516Document8 pagesModule 2: Respiratory System SEM 2 SESI 2019/2020 Group: A: Name: Mohamad Aiman Iqbal Bin Nordin MATRIC NO: D20192091516muhd ariffNo ratings yet
- Johnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-141-160Document20 pagesJohnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-141-160toanbauNo ratings yet
- The Human Respiratory SystemDocument19 pagesThe Human Respiratory SystemChelsea EdwardsNo ratings yet
- The Respiratory System: Gas Exchange and ControlDocument38 pagesThe Respiratory System: Gas Exchange and Controlglenn johnstonNo ratings yet
- The Human Respiratory SystemDocument5 pagesThe Human Respiratory SystemnekromadavidNo ratings yet
- The Respiratory SystemDocument55 pagesThe Respiratory SystemChuy Cantu RdzNo ratings yet
- The Human Breathing SystemDocument5 pagesThe Human Breathing SystemHarry Cianne Luther Sayon100% (1)
- The Respiratory System: An OverviewDocument33 pagesThe Respiratory System: An OverviewCess Abad AgcongNo ratings yet
- Breathing and Exchange of Gases: A Guide to RespirationDocument4 pagesBreathing and Exchange of Gases: A Guide to RespirationSreeyansu RajNo ratings yet
- Notes On Respiratory System, Gaseous ExchangeDocument4 pagesNotes On Respiratory System, Gaseous Exchangeshelter musasaNo ratings yet
- Fundamentalof Ventilation & PacemakerDocument22 pagesFundamentalof Ventilation & PacemakerLucila Lugo100% (1)
- Pulmnonary SystemDocument13 pagesPulmnonary Systemnatalie muyengwaNo ratings yet
- Breathing & Exchange of GasesDocument5 pagesBreathing & Exchange of GasesMamta TiwariNo ratings yet
- Respiratory Physiology GuideDocument21 pagesRespiratory Physiology GuideKingsley UdeajaNo ratings yet
- Respiratory System ExplainedDocument42 pagesRespiratory System ExplainedSohailriazNo ratings yet
- Respiratory System Functions and PhysiologyDocument11 pagesRespiratory System Functions and PhysiologyElleNo ratings yet
- CH 11 Gas Exchange in HumansDocument4 pagesCH 11 Gas Exchange in HumansPranitha RaviNo ratings yet
- Respiratory System OverviewDocument4 pagesRespiratory System Overviewbunso padillaNo ratings yet
- CHAPTER 17 Breathing &exchange of Gases-NotesDocument9 pagesCHAPTER 17 Breathing &exchange of Gases-Notessukaina mumtazNo ratings yet
- TARIQUL - ISLAM - GOLDARMechanism of Respiration.2021-04-30mechanism of RespirationDocument10 pagesTARIQUL - ISLAM - GOLDARMechanism of Respiration.2021-04-30mechanism of RespirationJuwairiyya AliyuNo ratings yet
- Module 7-11 The Respiratory SystemDocument52 pagesModule 7-11 The Respiratory SystemAlfred James SorianoNo ratings yet
- Anatomi Saluran PernapasanDocument6 pagesAnatomi Saluran PernapasanfidyaNo ratings yet
- Breathing and Exchange of GasesDocument10 pagesBreathing and Exchange of GasesAnonymous 9uu04elNo ratings yet
- Gaseous ExchangeDocument83 pagesGaseous ExchangeChai Kah ChunNo ratings yet
- Astm D3648 - 2014Document28 pagesAstm D3648 - 2014alferedNo ratings yet
- TheEconomist 2020 12 10Document296 pagesTheEconomist 2020 12 10merlindebergNo ratings yet
- Smartyou 21 Day PDF PlannerDocument9 pagesSmartyou 21 Day PDF PlannerYarelis Montero Mercado100% (1)
- HIST2601 HSienaDocument6 pagesHIST2601 HSienaQuinn HarringtonNo ratings yet
- PowerStop Shock Absorber CatalogDocument24 pagesPowerStop Shock Absorber CatalogAfiyat Nur100% (1)
- Nust Hostel Rules H-12 Campus IslamabadDocument10 pagesNust Hostel Rules H-12 Campus IslamabadNeha KhanNo ratings yet
- Uwezo-SAT-W-L-In Class-SET 1 - WMDocument15 pagesUwezo-SAT-W-L-In Class-SET 1 - WMAditya KantipudiNo ratings yet
- The Logic of Immunity Deciphering An EnigmaDocument204 pagesThe Logic of Immunity Deciphering An EnigmaSatyabrataSahaNo ratings yet
- Intro To Psychology Crash Course Psychology 1Document3 pagesIntro To Psychology Crash Course Psychology 1Hahaha YeahNo ratings yet
- Cased Hole LoggingDocument131 pagesCased Hole LoggingEbenezer Amoah-Kyei100% (1)
- NBC-Building Evacuation - SeminarDocument23 pagesNBC-Building Evacuation - SeminarRemer JalbunaNo ratings yet
- Valtek Beta Positioners: For Control ValvesDocument8 pagesValtek Beta Positioners: For Control Valvesابزار دقیقNo ratings yet
- hc2019 Re Use Recycle To Reduce CarbonDocument68 pageshc2019 Re Use Recycle To Reduce CarbonFatemeh DavariNo ratings yet
- Caldwell Schizophrenizing LacanDocument10 pagesCaldwell Schizophrenizing LacanaxisofelvisNo ratings yet
- English Speaking BasicsDocument52 pagesEnglish Speaking BasicsMukesh Verma100% (1)
- Classification: HypertensionDocument13 pagesClassification: HypertensiontermskipopNo ratings yet
- Senior Citizens and Human RightsDocument16 pagesSenior Citizens and Human RightsRiya SinghNo ratings yet
- Academic Procrastination, Self Efficacy and Anxiety of StudentsDocument7 pagesAcademic Procrastination, Self Efficacy and Anxiety of Studentscharvi didwania100% (3)
- Gas/Liquids Separators - Part 2: Quantifying Separation PerformanceDocument13 pagesGas/Liquids Separators - Part 2: Quantifying Separation PerformanceLizbeth Ramirez AlanyaNo ratings yet
- Chapter - 08 Civics Confronting Marginalisation: Invoking Fundamental RightsDocument2 pagesChapter - 08 Civics Confronting Marginalisation: Invoking Fundamental Rightsnbs saraswathiNo ratings yet
- Three Vital Elements of Qigong Exercise by Master Chunyi LinDocument3 pagesThree Vital Elements of Qigong Exercise by Master Chunyi LinTengriNo ratings yet
- Dip Zinc 7-Tank ProcessDocument3 pagesDip Zinc 7-Tank ProcessAmit Chauhan100% (1)
- Reviewer Ansc 111Document6 pagesReviewer Ansc 111Jeric MadroñoNo ratings yet
- New Balance 5k Training AdvancedDocument7 pagesNew Balance 5k Training Advancedijonilisha100% (1)
- JnaDocument34 pagesJnaDeepak KumarNo ratings yet
- Pulseless Arrest Algorithm For Managing AsystoleDocument1 pagePulseless Arrest Algorithm For Managing AsystoleLady MuffinsNo ratings yet
- The McKenzie Method Powerpoint - 2008Document57 pagesThe McKenzie Method Powerpoint - 2008aslooclt100% (2)
- CSFDocument5 pagesCSFjalan_zNo ratings yet
- Tle9agricropproduction q1 m5 ProvidingworksupportinaccordancewithOHSforhorticulturalproductionwork v3Document26 pagesTle9agricropproduction q1 m5 ProvidingworksupportinaccordancewithOHSforhorticulturalproductionwork v3Marycon Lao NacitoNo ratings yet
- Pest Management Practices of Farmers in PambujanDocument13 pagesPest Management Practices of Farmers in PambujanLucille MoralesNo ratings yet