You might also like
- Case Paul Foster The Secret Doctrines of The Tarot PDFDocument157 pagesCase Paul Foster The Secret Doctrines of The Tarot PDFLinden100% (1)
- My Side of The Mountain PDFDocument61 pagesMy Side of The Mountain PDF12333% (3)
- Streamlit Interface For Multiple Disease DiagnosisDocument8 pagesStreamlit Interface For Multiple Disease DiagnosisIJRASETPublicationsNo ratings yet
- Hacking, Ian - Estilos de RazonamientoDocument18 pagesHacking, Ian - Estilos de RazonamientoBadtz MaruNo ratings yet
- ISO 14031 Environmental Performance EvaluationDocument65 pagesISO 14031 Environmental Performance EvaluationSanjayaNo ratings yet
- Exploring The Efficacy of Machine Learning Algorithms For Diabetes Prediction A Comparative PredictionDocument9 pagesExploring The Efficacy of Machine Learning Algorithms For Diabetes Prediction A Comparative PredictionIJRASETPublicationsNo ratings yet
- Paper-6 - Enhanced Fuzzy Verdict Mechanism For Diabetes Using Fuzzy Expert SystemDocument12 pagesPaper-6 - Enhanced Fuzzy Verdict Mechanism For Diabetes Using Fuzzy Expert SystemRachel WheelerNo ratings yet
- LibreView Guide - Italian PaperDocument12 pagesLibreView Guide - Italian PaperJesus MuñozNo ratings yet
- Research ProposalDocument13 pagesResearch Proposalsaby aroraNo ratings yet
- Projectreport Diabetes PredictionDocument22 pagesProjectreport Diabetes PredictionushavalsaNo ratings yet
- Paper 2 HighlightedDocument9 pagesPaper 2 HighlightedVaishnavi YacheNo ratings yet
- ML 2020Document18 pagesML 2020Bhaskar Rao PNo ratings yet
- Prediction of Cardiovascular Disease Using Machine Learning TechniquesDocument6 pagesPrediction of Cardiovascular Disease Using Machine Learning TechniquesNowreen HaqueNo ratings yet
- Robust PBPK/PD-Based Model PredictiveDocument13 pagesRobust PBPK/PD-Based Model PredictivenhatvpNo ratings yet
- Continuous Glucose Monitoring: Evidence and Consensus Statement For Clinical UseDocument20 pagesContinuous Glucose Monitoring: Evidence and Consensus Statement For Clinical UseBianca CosovanuNo ratings yet
- Application of Data Mining Methods in Diabetes PredictionDocument5 pagesApplication of Data Mining Methods in Diabetes PredictionAptechBhilaiNo ratings yet
- Accelerometer Data Collection and Processing Criteria To AssessDocument25 pagesAccelerometer Data Collection and Processing Criteria To AssessBJNo ratings yet
- Using Sentiment Analysis and Machine Learning Algorithms To Determine Citizens' PerceptionsDocument6 pagesUsing Sentiment Analysis and Machine Learning Algorithms To Determine Citizens' Perceptionss.bahliNo ratings yet
- Comparative Analysis of PID Tuning Techniques For Blood Glucose Level of Diabetic PatientDocument6 pagesComparative Analysis of PID Tuning Techniques For Blood Glucose Level of Diabetic Patient015Maulana Malik IbrahimNo ratings yet
- Prediction of Diabetes Disease Using Machine Learning Algorithms28 20782Document7 pagesPrediction of Diabetes Disease Using Machine Learning Algorithms28 20782IAES IJAINo ratings yet
- Alfian 2020 IOP Conf. Ser. Mater. Sci. Eng. 803 012012Document8 pagesAlfian 2020 IOP Conf. Ser. Mater. Sci. Eng. 803 012012Muhammad AnshariNo ratings yet
- Utilisation of Telemedicine To Assess Energy Expenditure and Stability in Older People With Chronic Kidney DiseaseDocument4 pagesUtilisation of Telemedicine To Assess Energy Expenditure and Stability in Older People With Chronic Kidney DiseaseSergio Raposo PerezNo ratings yet
- Thorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsDocument12 pagesThorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsgercampeNo ratings yet
- Performance Evaluation of The GlunovoR ContinuousDocument13 pagesPerformance Evaluation of The GlunovoR ContinuousshahirahNo ratings yet
- Decision Tree Discovery For The Diagnosis of Type II DiabetesDocument5 pagesDecision Tree Discovery For The Diagnosis of Type II DiabetesEka Panuju QuiñonesNo ratings yet
- Journal Pone 0248280 PDFDocument17 pagesJournal Pone 0248280 PDFHafis KafitNo ratings yet
- Predicción Longitudinal de La Aptitud Cardiorrespiratoria A Través de Dispositivos Portátiles en Entornos de Vida LibreDocument11 pagesPredicción Longitudinal de La Aptitud Cardiorrespiratoria A Través de Dispositivos Portátiles en Entornos de Vida Libremariojosehurtado3955No ratings yet
- Design of A Portable Urine Glucose Monitoring System For Health CareDocument12 pagesDesign of A Portable Urine Glucose Monitoring System For Health CareaksssudhakarNo ratings yet
- Improving Length of Stay Prediction Using A Hidden Markov ModelDocument10 pagesImproving Length of Stay Prediction Using A Hidden Markov ModelTanvin AyatNo ratings yet
- Prediction of Diabetes Paper July 2022Document6 pagesPrediction of Diabetes Paper July 2022PraveenNo ratings yet
- ThesisChap1 3Document12 pagesThesisChap1 3Precious YasayNo ratings yet
- Sensors: Advanced Diabetes Management Using Artificial Intelligence and Continuous Glucose Monitoring SensorsDocument18 pagesSensors: Advanced Diabetes Management Using Artificial Intelligence and Continuous Glucose Monitoring SensorsShujian ZhaoNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Wissanu Naruemon Ic2it ManuDocument9 pagesWissanu Naruemon Ic2it ManuWissanu ThungrutNo ratings yet
- Prediction of Diabetics Based On Machine LearningDocument8 pagesPrediction of Diabetics Based On Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ProjectDocument16 pagesProjectRitesh RathodNo ratings yet
- Diabetes Prediction ReportDocument16 pagesDiabetes Prediction Reportareeshaabass4No ratings yet
- Alm037 01 02Document10 pagesAlm037 01 02MarcelliaNo ratings yet
- Report DiabeticsDocument8 pagesReport DiabeticsBindhu NNo ratings yet
- Noninvasive Glocosa Subspace KNNDocument7 pagesNoninvasive Glocosa Subspace KNNhendranatjNo ratings yet
- Noninvasive Glocosa Subspace KNNDocument7 pagesNoninvasive Glocosa Subspace KNNhendranatjNo ratings yet
- ExempluDocument12 pagesExempluCristina ElenaNo ratings yet
- Báo KHDocument12 pagesBáo KHDUY VÕ HUỲNH NHẬTNo ratings yet
- Diabetes Research and Clinical Practice Volume Issue 2018Document37 pagesDiabetes Research and Clinical Practice Volume Issue 2018yayan_adiutama98No ratings yet
- Journal Reading Major Surgery Gastric BypassDocument12 pagesJournal Reading Major Surgery Gastric BypassLiza MPNo ratings yet
- Flash Glucose MonitoringDocument9 pagesFlash Glucose MonitoringAneed AnandNo ratings yet
- A Blood Pressure Prediction Method Based On Imaging Photoplethysmography in Combination With Machine LearningDocument11 pagesA Blood Pressure Prediction Method Based On Imaging Photoplethysmography in Combination With Machine LearningPING KWAN MANNo ratings yet
- On-Line Fetal Heart Rate Monitor by PhonocardiographyDocument4 pagesOn-Line Fetal Heart Rate Monitor by PhonocardiographyOscar Rosado RegaladoNo ratings yet
- Predicting Cardiovascular Disease Using Logistic Regression Research PaperDocument4 pagesPredicting Cardiovascular Disease Using Logistic Regression Research PaperSbobhuNo ratings yet
- Glucose Level Monitoring Arduino GlucometerDocument15 pagesGlucose Level Monitoring Arduino GlucometerNebitno UopsteNo ratings yet
- Artificial Pancreas Device Systems For The Closed-Loop Control of Type 1 Diabetes: What Systems Are in Development?Document10 pagesArtificial Pancreas Device Systems For The Closed-Loop Control of Type 1 Diabetes: What Systems Are in Development?efNo ratings yet
- Canadian Journal of Diabetes: Special ArticleDocument8 pagesCanadian Journal of Diabetes: Special ArticleUsee TvNo ratings yet
- s00125 024 06145 0 - 240426 - 192850Document12 pagess00125 024 06145 0 - 240426 - 192850lakshminivas PingaliNo ratings yet
- U WB DiabetesDocument9 pagesU WB DiabetesSindhuja SankaranNo ratings yet
- Predictive Analysis of Diabetes Without Data Pre-Processing Via The Evaluation of Tree AlgorithmsDocument11 pagesPredictive Analysis of Diabetes Without Data Pre-Processing Via The Evaluation of Tree AlgorithmsIJAR JOURNALNo ratings yet
- Non-Invasive Glucose Monitoring Using Optical Sensor and Machine Learning Techniques For Diabetes ApplicationsDocument17 pagesNon-Invasive Glucose Monitoring Using Optical Sensor and Machine Learning Techniques For Diabetes Applicationseswaramoorthy848No ratings yet
- Sensors 20 01705Document11 pagesSensors 20 01705QSilvaNo ratings yet
- Continuous Glucose MonitoringFrom EverandContinuous Glucose MonitoringWeiping JiaNo ratings yet
- 10.1007@s11695 020 05012 2Document9 pages10.1007@s11695 020 05012 2Andrés MaldonadoNo ratings yet
- Management Algorithm Patients Intracranial Pressure Monitoring Seattle International Severe Traumatic Brain Injury Consensus Conference Sibicc 2019Document12 pagesManagement Algorithm Patients Intracranial Pressure Monitoring Seattle International Severe Traumatic Brain Injury Consensus Conference Sibicc 2019maria arenas de itaNo ratings yet
- Physiological Differences Between Interstitial Glucose and Blood Glucose Measured in Human SubjectsDocument5 pagesPhysiological Differences Between Interstitial Glucose and Blood Glucose Measured in Human Subjectsmosca90No ratings yet
- Ijet V3i5p35Document6 pagesIjet V3i5p35International Journal of Engineering and TechniquesNo ratings yet
- SIBICCDocument12 pagesSIBICCnindyaNo ratings yet
- Voltage Intensity Based ImpDocument5 pagesVoltage Intensity Based ImpVirajRanawareNo ratings yet
- 2019 Mou HIU AEDocument6 pages2019 Mou HIU AEJagadish VenkataramanNo ratings yet
- TutorialOnWaveletsFromEEperspective PDFDocument22 pagesTutorialOnWaveletsFromEEperspective PDFJagadish VenkataramanNo ratings yet
- TOA Estimation in NLOS EnvtsDocument5 pagesTOA Estimation in NLOS EnvtsJagadish VenkataramanNo ratings yet
- Bayesian Filtering - From Kalman Filters To Particle Filters and BeyondDocument69 pagesBayesian Filtering - From Kalman Filters To Particle Filters and BeyondRamanan MuthuramanNo ratings yet
- Historical FoundationDocument13 pagesHistorical Foundationᜃᜒᜈ᜔ᜎᜒ ᜇᜒᜋᜈ᜔ᜇᜒᜋᜈ᜔No ratings yet
- Allama Iqbal Open University, Islamabad: WarningDocument3 pagesAllama Iqbal Open University, Islamabad: Warningمحمد کاشفNo ratings yet
- Expert-Verified: COMPETITIVE in NatureDocument1 pageExpert-Verified: COMPETITIVE in NatureBeibei LingNo ratings yet
- WO 2053 Handling Sec 5-1 Electric Diagram PreliminaryDocument245 pagesWO 2053 Handling Sec 5-1 Electric Diagram PreliminaryMinh TrầnNo ratings yet
- PSE PG Structure ModifedDocument61 pagesPSE PG Structure ModifedAnkit YadavNo ratings yet
- Đề MINH HỌA Số 11 Luyện Thi Tốt Nghiệp THPT 2023Document7 pagesĐề MINH HỌA Số 11 Luyện Thi Tốt Nghiệp THPT 2023Minh ThưNo ratings yet
- Statistics For Business and EconomicsDocument19 pagesStatistics For Business and EconomicsSai MeenaNo ratings yet
- Graded Assignment: Unit Test, Part 2: Radicals and Complex NumbersDocument3 pagesGraded Assignment: Unit Test, Part 2: Radicals and Complex NumbersManuk SogomonyanNo ratings yet
- Simulation-Using The Micrometer Screw GaugeDocument2 pagesSimulation-Using The Micrometer Screw GaugeAlejandro MohammedNo ratings yet
- Hydroelastic Analysis Procedure For ShipsDocument42 pagesHydroelastic Analysis Procedure For ShipsVictor DaggersNo ratings yet
- Housekeeping Services NCII Quarter 3 PDF HousekeepingDocument1 pageHousekeeping Services NCII Quarter 3 PDF HousekeepingSalve RegineNo ratings yet
- Quantity Surveying Division Assessment of Professional Competence Final Assessment 2015 Practice ProblemsDocument21 pagesQuantity Surveying Division Assessment of Professional Competence Final Assessment 2015 Practice ProblemsjackyNo ratings yet
- Technical Data Sheet: Davies Powerfloor Epoxy Floor CoatingDocument1 pageTechnical Data Sheet: Davies Powerfloor Epoxy Floor CoatingEnoki LiNo ratings yet
- Uttarakhand Open UniversityDocument308 pagesUttarakhand Open UniversityCommerce WhizNo ratings yet
- Institute of Southern Punjab Multan: Syed Zohair Quain Haider Lecturer ISP MultanDocument47 pagesInstitute of Southern Punjab Multan: Syed Zohair Quain Haider Lecturer ISP MultanCh MaaanNo ratings yet
- Report Group 1Document67 pagesReport Group 11706112No ratings yet
- Adams ST - Pierre Post Qualitative InquiryDocument7 pagesAdams ST - Pierre Post Qualitative InquiryJOOST VANMAELENo ratings yet
- Short CV RJCDocument3 pagesShort CV RJCShivani KhannaNo ratings yet
- Aug 7 IELTS Test 20Document10 pagesAug 7 IELTS Test 20Sunshine HannNo ratings yet
- One-Day Workshop Brochure - KHP - 10.02.2022Document1 pageOne-Day Workshop Brochure - KHP - 10.02.2022Ramya RajeshNo ratings yet
- Models of Cultural Heritage Management: Transformations in Business and Economics January 2014Document23 pagesModels of Cultural Heritage Management: Transformations in Business and Economics January 2014aaziNo ratings yet
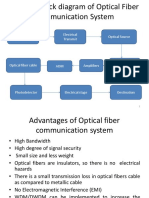
- Source of Information Electrical Transmit Optical SourceDocument37 pagesSource of Information Electrical Transmit Optical SourcesubashNo ratings yet
- Sonic Drive inDocument1 pageSonic Drive inWXYZ-TV Channel 7 DetroitNo ratings yet
- ASTM Manual Series, MNL 52 An IntroductionDocument73 pagesASTM Manual Series, MNL 52 An IntroductionPabel Gil Ramirez CamonesNo ratings yet
- Mark Scheme (Results) : Summer 2017Document22 pagesMark Scheme (Results) : Summer 2017Khalid AhmedNo ratings yet
- Theory of Corporate PersonalityDocument7 pagesTheory of Corporate PersonalityKabita SharmaNo ratings yet