You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Congenital Heart DiseaseDocument20 pagesCongenital Heart DiseaseAbhishek KumarNo ratings yet
- Peds Shelf NotesDocument73 pagesPeds Shelf NotesTanyaMusonza100% (1)
- Peds Shelf NotesDocument88 pagesPeds Shelf Notesγιαννης παπαςNo ratings yet
- Coronary Artery DiseaseDocument3 pagesCoronary Artery DiseaseRitz CelsoNo ratings yet
- Congenital Heart DefectsDocument6 pagesCongenital Heart DefectsJohiarra Madanglog TabigneNo ratings yet
- Anak 2Document107 pagesAnak 2Nency PurmayaNo ratings yet
- Pediatric Cardiology II Lecture SummaryDocument5 pagesPediatric Cardiology II Lecture SummaryMedisina101No ratings yet
- Right to Left Shunts: Tetralogy of Fallot, Transposition of Great Arteries, Tricuspid AtresiaDocument5 pagesRight to Left Shunts: Tetralogy of Fallot, Transposition of Great Arteries, Tricuspid AtresiaIgwe SolomonNo ratings yet
- Congenital Heart DiseaseDocument3 pagesCongenital Heart DiseaseKarisaNo ratings yet
- AV - Congenital Heart DiseaseDocument10 pagesAV - Congenital Heart DiseasebakiralhamdaniNo ratings yet
- Congenital Heart DefectsDocument7 pagesCongenital Heart DefectsJulia Rae Delos SantosNo ratings yet
- Cardiovascular Dysfunction: (Patent Ductus Arteriosus)Document6 pagesCardiovascular Dysfunction: (Patent Ductus Arteriosus)Jc MacujaNo ratings yet
- Obstructive LesionsDocument7 pagesObstructive LesionsMaikka IlaganNo ratings yet
- Congenital Heart Defect Diagnosis and TreatmentDocument5 pagesCongenital Heart Defect Diagnosis and TreatmentPrincess LegansonNo ratings yet
- Congenital Heart Disease (CHD)Document89 pagesCongenital Heart Disease (CHD)jefferyNo ratings yet
- 1.conginital Cardiac DefectsDocument39 pages1.conginital Cardiac DefectsJõsëph Jåy MîthNo ratings yet
- Congenital Heart DiseaseDocument12 pagesCongenital Heart DiseaseNinna Isabel VictorioNo ratings yet
- CHD Lecture for C-I StudentsDocument89 pagesCHD Lecture for C-I StudentsGomathi ShankarNo ratings yet
- ch28 Notes Part 2Document9 pagesch28 Notes Part 2Monica JubaneNo ratings yet
- Understanding Congenital Heart DiseaseDocument54 pagesUnderstanding Congenital Heart DiseaseYemata HailuNo ratings yet
- Presented by Dona Mathew MSC (N) Govt - College of Nursing KottayamDocument221 pagesPresented by Dona Mathew MSC (N) Govt - College of Nursing KottayamSumathi GopinathNo ratings yet
- UWorld Notes - Peds 2Document38 pagesUWorld Notes - Peds 2Dylan GerlachNo ratings yet
- Nursing Care of The Child Born With Congenital Heart DisordersDocument3 pagesNursing Care of The Child Born With Congenital Heart DisordersElijah GarciaNo ratings yet
- Heart - PathologyDocument22 pagesHeart - Pathologyjmosser100% (1)
- ASD Aortic StenosisDocument3 pagesASD Aortic Stenosis[161]Shuaib AktherNo ratings yet
- Congenital Heart Disease ExplainedDocument74 pagesCongenital Heart Disease ExplainedKeith LajotNo ratings yet
- Diagnosis Depend On: 1-Clinical Features: - Palpation - Auscultation 2 - CXR: - Chamber Enlargement - Plethoric LungDocument11 pagesDiagnosis Depend On: 1-Clinical Features: - Palpation - Auscultation 2 - CXR: - Chamber Enlargement - Plethoric LungYasir Al-KhateebNo ratings yet
- Congenital Heart Disease Types and TreatmentsDocument9 pagesCongenital Heart Disease Types and Treatmentsdr_alfuNo ratings yet
- Congenital Heart DiseaseDocument6 pagesCongenital Heart DiseaseSamah KhanNo ratings yet
- Cardiopatii Congenitale 17-18 enDocument74 pagesCardiopatii Congenitale 17-18 enMatei PopescuNo ratings yet
- MAGCAR 12 - Cardiopatías CongénitasDocument61 pagesMAGCAR 12 - Cardiopatías CongénitasMovil Maria 2No ratings yet
- CCHDDocument69 pagesCCHDchebetnaomi945No ratings yet
- Surgery II: Congenital Heart DiseaseDocument10 pagesSurgery II: Congenital Heart DiseaseRea Dominique CabanillaNo ratings yet
- Clinical Congenital Heart Disease: Prof M S Ranjit MD DCH Senior Consultant Paed. Cardiologist ChennaiDocument78 pagesClinical Congenital Heart Disease: Prof M S Ranjit MD DCH Senior Consultant Paed. Cardiologist ChennaiAnişoara FrunzeNo ratings yet
- Pulmonary Embolism: Risks, Symptoms & DiagnosisDocument39 pagesPulmonary Embolism: Risks, Symptoms & DiagnosisAsmaa ahmedNo ratings yet
- Pediatric Cardiovascular Disorders GuideDocument4 pagesPediatric Cardiovascular Disorders GuideWendy EscalanteNo ratings yet
- Dr. RSK - Cyanotic Congenital Heart DiseaseDocument44 pagesDr. RSK - Cyanotic Congenital Heart Diseasemanjunath182019No ratings yet
- CN 118 - Lecture ReviewerDocument20 pagesCN 118 - Lecture ReviewerCamille SanguyoNo ratings yet
- Aortic StenosisDocument8 pagesAortic Stenosisdr.moni.co.ukNo ratings yet
- Congenital Heart Disease NotesDocument7 pagesCongenital Heart Disease NotesFarisa Jane BanggoNo ratings yet
- Management of Cyanotic Child BivinDocument48 pagesManagement of Cyanotic Child BivinChippy BivinNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument48 pagesAcyanotic Congenital Heart DiseasenabillagusrinaNo ratings yet
- Acyanotic Congenital Heart DiseasesDocument7 pagesAcyanotic Congenital Heart DiseasesAlvin De LunaNo ratings yet
- CHD Diagnosis and TypesDocument70 pagesCHD Diagnosis and Typesjulis muharamNo ratings yet
- Cardio NotesDocument2 pagesCardio NotesMagdaraog Gabrielle A.No ratings yet
- Congenital Heart Disease: Causes, Types, Symptoms and TreatmentDocument69 pagesCongenital Heart Disease: Causes, Types, Symptoms and TreatmentAswathy AswathyNo ratings yet
- Endocarditis: (Post Strep Infection)Document8 pagesEndocarditis: (Post Strep Infection)Eben Ezar Dela CruzNo ratings yet
- 10 1016@j CCL 2020 04 008Document12 pages10 1016@j CCL 2020 04 008Linda Silvana SariNo ratings yet
- Heart: Exam 2Document46 pagesHeart: Exam 2ChristinePagsisihanNo ratings yet
- CME Cyanotic Heart DiseaseDocument38 pagesCME Cyanotic Heart DiseaseTan Zhi HongNo ratings yet
- Zuñega - Congenital Heart Disease Educational MaterialsDocument13 pagesZuñega - Congenital Heart Disease Educational MaterialsAprilene Angel Balaque ZunegaNo ratings yet
- Module No. Date: Topic:: Cues/Questions/ Keywords Notes Congenital Heart DisordersDocument28 pagesModule No. Date: Topic:: Cues/Questions/ Keywords Notes Congenital Heart Disordersanon ymousNo ratings yet
- Peds Shelf NotesDocument74 pagesPeds Shelf NotesRandy BornmannNo ratings yet
- Congenital Heart Disease 1Document14 pagesCongenital Heart Disease 1OzzeyNo ratings yet
- Pulmonary Thrombo EmbolismDocument3 pagesPulmonary Thrombo EmbolismTom MallinsonNo ratings yet
- HCM PDA: Disease Signalment Pathophysiology CSX TXDocument1 pageHCM PDA: Disease Signalment Pathophysiology CSX TXhalf_frozen_cho6435No ratings yet
- Approach To Congenital Heart DiseaseDocument26 pagesApproach To Congenital Heart DiseaseffNo ratings yet
- Pharmacology of Antipsychotic Agents Cheat SheetDocument3 pagesPharmacology of Antipsychotic Agents Cheat SheetCrystal MarloweNo ratings yet
- Psych Meds 2Document2 pagesPsych Meds 2Cole SchaferNo ratings yet
- Lizzie Heisler - Hypertension MedsDocument2 pagesLizzie Heisler - Hypertension MedsTricia Kaye IblanNo ratings yet
- Adrenergic Drugs Cheat SheetDocument3 pagesAdrenergic Drugs Cheat SheetThư PhạmNo ratings yet
- Carmilaa - Introduction To PharmacologyDocument2 pagesCarmilaa - Introduction To PharmacologyTricia Kaye IblanNo ratings yet
- Ksellybelly - MSK I Arthritis RheumDocument4 pagesKsellybelly - MSK I Arthritis RheumTricia Kaye IblanNo ratings yet
- Reuben - Drug Classes and Actions NsaidsDocument2 pagesReuben - Drug Classes and Actions NsaidsTricia Kaye IblanNo ratings yet
- Pharmacology of Antipsychotic Agents Cheat SheetDocument3 pagesPharmacology of Antipsychotic Agents Cheat SheetCrystal MarloweNo ratings yet
- X0xheather - Principles of Antimicrobial Chemotherapy PDFDocument3 pagesX0xheather - Principles of Antimicrobial Chemotherapy PDFAbdul RaufNo ratings yet
- Phychem Chapter 3 Part 1Document14 pagesPhychem Chapter 3 Part 1Skye DiazNo ratings yet
- Fi & EiDocument3 pagesFi & EiPrasanna S Kulkarni100% (1)
- Chapter 1 and 2Document67 pagesChapter 1 and 2Tle SupawidNo ratings yet
- 6kW V2G EV Charger Module Datasheet (2018)Document2 pages6kW V2G EV Charger Module Datasheet (2018)pysogaNo ratings yet
- Training ManualDocument41 pagesTraining Manualemiliow_1100% (3)
- Aula 4 - Wooten - Organizational FieldsDocument28 pagesAula 4 - Wooten - Organizational FieldsferreiraccarolinaNo ratings yet
- Analog Layout Design (Industrial Training)Document10 pagesAnalog Layout Design (Industrial Training)Shivaksh SharmaNo ratings yet
- Bathymetry and Its Applications PDFDocument158 pagesBathymetry and Its Applications PDFArseni MaximNo ratings yet
- Entry-Exit Arrangement With Service RoadDocument1 pageEntry-Exit Arrangement With Service RoadRamBhuvan SonkarNo ratings yet
- Urban Ecology: Concept of Ecology and Its Importance in ArchitectureDocument12 pagesUrban Ecology: Concept of Ecology and Its Importance in ArchitectureNamrata JitendraNo ratings yet
- K2N Final Internship ReportDocument55 pagesK2N Final Internship ReportAceZeta0% (1)
- Assignment 12Document7 pagesAssignment 12Anonymous mqIqN5zNo ratings yet
- Wemco Depurator 2003Document2 pagesWemco Depurator 20031mmahoneyNo ratings yet
- CHAPT 12a PDFDocument2 pagesCHAPT 12a PDFindocode100% (1)
- Steel Grid StructureDocument2 pagesSteel Grid StructureKusum RawatNo ratings yet
- A Feminist Analysis of Habba Khatoon'S Poetry: Dr. Mir Rifat NabiDocument7 pagesA Feminist Analysis of Habba Khatoon'S Poetry: Dr. Mir Rifat NabiShabir AhmadNo ratings yet
- MUSCULAR SYSTEM WORKSHEET Slides 1 To 4Document4 pagesMUSCULAR SYSTEM WORKSHEET Slides 1 To 4kwaiyuen ohnNo ratings yet
- Airway Management in The Critically Ill: ReviewDocument9 pagesAirway Management in The Critically Ill: ReviewQuarmina HesseNo ratings yet
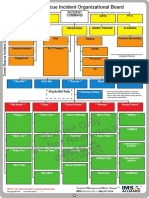
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- Altivar ATV61HU55N4 CatalogueDocument4 pagesAltivar ATV61HU55N4 CatalogueEugen Marius BadescuNo ratings yet
- AAB 075323 EPDM Waterproofing Membrane (For RC Roof Build-Up Inc. Insulation)Document3 pagesAAB 075323 EPDM Waterproofing Membrane (For RC Roof Build-Up Inc. Insulation)tewodrosNo ratings yet
- dSPACE CLP1104 Manual 201663013420Document172 pagesdSPACE CLP1104 Manual 201663013420meghraj01No ratings yet
- Capacitores Electroliticos SMDDocument8 pagesCapacitores Electroliticos SMDalvaro marrugoNo ratings yet
- The Following Functional Health Pattern Assessment Is Based On A 65 Year Old Scottish Woman Who Lives Independently With Her Husband in Their Home at Happy ValleyDocument9 pagesThe Following Functional Health Pattern Assessment Is Based On A 65 Year Old Scottish Woman Who Lives Independently With Her Husband in Their Home at Happy ValleyJajangNo ratings yet
- Preventive Maintenance Service Concept For SPACOM Product FamilyDocument27 pagesPreventive Maintenance Service Concept For SPACOM Product FamilyMiguel MarquesNo ratings yet
- How To Attract Love and Powerful Soul ConnectionsDocument5 pagesHow To Attract Love and Powerful Soul Connectionskinzaali71916No ratings yet
- Quest The Last RemnantDocument67 pagesQuest The Last Remnantding suheNo ratings yet
- Solitaire Premier - Presentation (Small File)Document18 pagesSolitaire Premier - Presentation (Small File)Shrikant BadheNo ratings yet
- Line Pack Presentation - Dec 2018Document7 pagesLine Pack Presentation - Dec 2018Goran JakupovićNo ratings yet
- Global Resort List by Country (38 charactersDocument51 pagesGlobal Resort List by Country (38 charactersMaulik ShahNo ratings yet