You might also like
- Efficacy of Dexamethasone For Reducing Postoperative Nausea and Vomiting and Analgesic Requirements After ThyroidectomyDocument4 pagesEfficacy of Dexamethasone For Reducing Postoperative Nausea and Vomiting and Analgesic Requirements After ThyroidectomyDr shehwarNo ratings yet
- Section: Surgery: Category: B - Clinical SciencesDocument6 pagesSection: Surgery: Category: B - Clinical SciencesAbu TauhidNo ratings yet
- Apm009-02-07 2Document5 pagesApm009-02-07 2Kristine Lou Tan RualloNo ratings yet
- Effects of propofol versus sevoflurane anesthesia on postoperative pain after gastrectomyDocument33 pagesEffects of propofol versus sevoflurane anesthesia on postoperative pain after gastrectomyJuwita PratiwiNo ratings yet
- haloperidol combined with dexamethasoneDocument6 pageshaloperidol combined with dexamethasoneapi-741687858No ratings yet
- Early Postoperative ComplicationsDocument6 pagesEarly Postoperative Complications49hr84j7spNo ratings yet
- 与扑热息痛联用增效Document5 pages与扑热息痛联用增效zhuangemrysNo ratings yet
- BIS-Guided Propofol vs Etomidate Induction: Hypotension and Hypertension RiskDocument9 pagesBIS-Guided Propofol vs Etomidate Induction: Hypotension and Hypertension RiskGihan NakhlehNo ratings yet
- Effect of Intravenous Propacetamol On BL PDFDocument6 pagesEffect of Intravenous Propacetamol On BL PDFRahmat ullahNo ratings yet
- Relationship Between The Incidence and Risk Factors of Postoperative Nausea and Vomiting in Patients With Intravenous Patient-Controlled AnalgesiaDocument6 pagesRelationship Between The Incidence and Risk Factors of Postoperative Nausea and Vomiting in Patients With Intravenous Patient-Controlled AnalgesiaRandi KhampaiNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- ClonidineDocument4 pagesClonidineDR RAVI ANANDNo ratings yet
- RCT Parecoxib Acetaminophen...Document7 pagesRCT Parecoxib Acetaminophen...Paulina MuñozNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Anafilaxia MidazolamDocument3 pagesAnafilaxia MidazolamDiana PintorNo ratings yet
- Menadment of PainDocument4 pagesMenadment of PainMirza CoricNo ratings yet
- p6 High Risk PatientDocument6 pagesp6 High Risk Patientika lindaNo ratings yet
- MAC DexmethomidineDocument5 pagesMAC DexmethomidinedhitabwNo ratings yet
- Mounier - 2010Document10 pagesMounier - 2010Cindy KarmilaNo ratings yet
- Medical Treatment Versus Radiofrequency Ablation For Patients With Trigeminal Neuralgia: A Prospective Clinical StudyDocument5 pagesMedical Treatment Versus Radiofrequency Ablation For Patients With Trigeminal Neuralgia: A Prospective Clinical StudyasclepiuspdfsNo ratings yet
- Hidromorfona IV X Acetaminofeno IVDocument8 pagesHidromorfona IV X Acetaminofeno IVLucas CrahimNo ratings yet
- Indications and Outcomes of Nefopam Administration in Palliative Care PatientsDocument15 pagesIndications and Outcomes of Nefopam Administration in Palliative Care PatientsHamsa veniNo ratings yet
- Anes 10Document8 pagesAnes 10Fuchsia ZeinNo ratings yet
- Comparison of Analgesic Effects of Intravenous Nalbuphine and Pentazocine in Patients Posted For Short-Duration Surgeries A Prospective Randomized Double-Blinded StudyDocument4 pagesComparison of Analgesic Effects of Intravenous Nalbuphine and Pentazocine in Patients Posted For Short-Duration Surgeries A Prospective Randomized Double-Blinded StudyMuhammad AtifNo ratings yet
- 1828 1833Document6 pages1828 1833abdulNo ratings yet
- Ircmj 15 9267Document6 pagesIrcmj 15 9267samaraNo ratings yet
- 2017.multimodal Intrathecal Analgesia in Refractory Cancer PainDocument5 pages2017.multimodal Intrathecal Analgesia in Refractory Cancer Paintidarat.aimNo ratings yet
- 1576 Full PDFDocument8 pages1576 Full PDFRetno WidiastriNo ratings yet
- The Effects of Age On Neural Blockade and Hemodynamic Changes After Epidural Anesthesia With RopivacaineDocument6 pagesThe Effects of Age On Neural Blockade and Hemodynamic Changes After Epidural Anesthesia With RopivacaineAnonymous K9tmd7T0PzNo ratings yet
- A Change in Practice From Epidural To Intrathecal Morphine For Hepato Bilio SurgDocument7 pagesA Change in Practice From Epidural To Intrathecal Morphine For Hepato Bilio Surgvalerio.messinaNo ratings yet
- Epidural Analgesia - A Self-Directed Learning Module 3rdDocument41 pagesEpidural Analgesia - A Self-Directed Learning Module 3rdAnnisa Chaerani BurhanuddinNo ratings yet
- A Prospective, Randomized, Double-Blind, Multicenter Study Comparing Remifentanil With Fentanyl in Mechanically Ventilated PatientsDocument8 pagesA Prospective, Randomized, Double-Blind, Multicenter Study Comparing Remifentanil With Fentanyl in Mechanically Ventilated PatientsJosé Carlos Sánchez-RamirezNo ratings yet
- A Prospective, Randomized, Double-Blind, Multicenter Study Comparing Remifentanil With Fentanyl in Mechanically Ventilated PatientsDocument8 pagesA Prospective, Randomized, Double-Blind, Multicenter Study Comparing Remifentanil With Fentanyl in Mechanically Ventilated PatientsJosé Carlos Sánchez-RamirezNo ratings yet
- A Comparison of Intrathecal and Intravenous Morphine For Analgesia After HepatectomyDocument10 pagesA Comparison of Intrathecal and Intravenous Morphine For Analgesia After Hepatectomyvalerio.messinaNo ratings yet
- Original Papers: Prolonged Thiopentone Infusion For Neurosurgical Emergencies: Usefulness of Therapeutic Drug MonitoringDocument10 pagesOriginal Papers: Prolonged Thiopentone Infusion For Neurosurgical Emergencies: Usefulness of Therapeutic Drug MonitoringMohammedNo ratings yet
- Art 04Document6 pagesArt 04deboraNo ratings yet
- ComparisonOfDrooeridol&,metoclopramideDocument4 pagesComparisonOfDrooeridol&,metoclopramidemanishmandal1976No ratings yet
- Post Operative Effects Comparison of Total Intravenous and Inhalational Anesthesia 2155 6148.1000287Document7 pagesPost Operative Effects Comparison of Total Intravenous and Inhalational Anesthesia 2155 6148.1000287Taufik Sofist PresbomonetNo ratings yet
- Benefits and Risks of Dexamethasone in Noncardiac SurgeryDocument9 pagesBenefits and Risks of Dexamethasone in Noncardiac SurgeryHenry Gabriel HarderNo ratings yet
- Toradol To Reduce Ureteroscopy Symptoms Trial (TRUST)Document5 pagesToradol To Reduce Ureteroscopy Symptoms Trial (TRUST)Oscar GarciaNo ratings yet
- Is Granisetron-Dexamethasone Combination Better ThanDocument8 pagesIs Granisetron-Dexamethasone Combination Better ThanGustomo PanantroNo ratings yet
- Regional Versus General Anesthesia in Surgical Patients With Chronic Obstructive Pulmonary Disease: Does Avoiding General Anesthesia Reduce The Risk of Postoperative Complications?Document8 pagesRegional Versus General Anesthesia in Surgical Patients With Chronic Obstructive Pulmonary Disease: Does Avoiding General Anesthesia Reduce The Risk of Postoperative Complications?mluthfidunandNo ratings yet
- Midazolam Prevent AgitationDocument13 pagesMidazolam Prevent AgitationUzZySusFabregasNo ratings yet
- Pill in Pocket NEJMDocument8 pagesPill in Pocket NEJMn2coolohNo ratings yet
- KJAEDocument7 pagesKJAEM Wahyu UtomoNo ratings yet
- Comparing Spinal vs. General Anesthesia for Kidney Stone SurgeryDocument5 pagesComparing Spinal vs. General Anesthesia for Kidney Stone Surgerynaufal12345No ratings yet
- ScapeDocument7 pagesScapeRoshan MathewNo ratings yet
- Jurnal 2Document5 pagesJurnal 2Isle MotolandNo ratings yet
- Comparing Effects of Thiopental Induction Regimens in Hypertensive PatientsDocument6 pagesComparing Effects of Thiopental Induction Regimens in Hypertensive PatientschaNo ratings yet
- A ComparativeDocument5 pagesA ComparativedeadanandaNo ratings yet
- Neostigmine Administration After Spontaneous Recovery To A Train-of-Four Ratio of 0.9 To 1.0Document11 pagesNeostigmine Administration After Spontaneous Recovery To A Train-of-Four Ratio of 0.9 To 1.0Juan Jose Velasquez GutierrezNo ratings yet
- Jur DingDocument11 pagesJur DingI'am AjhaNo ratings yet
- The Analgesic Efficacy of Tramadol As A Pre-Emptive Analgesic in Pediatric Appendectomy Patients PDFDocument6 pagesThe Analgesic Efficacy of Tramadol As A Pre-Emptive Analgesic in Pediatric Appendectomy Patients PDFUmmu Qonitah AfnidawatiNo ratings yet
- Nitrous Oxide/oxygen Plus Acetaminophen Versus Morphine in ST Elevation Myocardial Infarction: Open-Label, Cluster-Randomized, Non-Inferiority StudyDocument9 pagesNitrous Oxide/oxygen Plus Acetaminophen Versus Morphine in ST Elevation Myocardial Infarction: Open-Label, Cluster-Randomized, Non-Inferiority StudyAkram KastiranNo ratings yet
- Adverse Events of Procedural Sedation and Analgesia in A Pediatric Emergency DepartmentDocument1 pageAdverse Events of Procedural Sedation and Analgesia in A Pediatric Emergency DepartmentRezza HaryNo ratings yet
- EtamolDocument5 pagesEtamolthonyyanmuNo ratings yet
- Anesthetic Management of A Patient With Myasthenia Gravis For Meningioma Surgery - A Case ReportDocument3 pagesAnesthetic Management of A Patient With Myasthenia Gravis For Meningioma Surgery - A Case ReportSushant AcharyaNo ratings yet
- Mammae 2 PDFDocument6 pagesMammae 2 PDFAdila YulianiNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- Anesthesia Technique and Mortality 2016Document8 pagesAnesthesia Technique and Mortality 2016John Portales ArmasNo ratings yet
- Service Manual: Freestanding Cooling Double Door ARC 2140Document5 pagesService Manual: Freestanding Cooling Double Door ARC 2140Sergio ZapataNo ratings yet
- 3 Sample Warranty: Sun Control Window FilmDocument1 page3 Sample Warranty: Sun Control Window FilmJanan AhmadNo ratings yet
- Entrepreneurship Macro Environment ForcesDocument26 pagesEntrepreneurship Macro Environment ForcesSivaNo ratings yet
- HymssheetDocument4 pagesHymssheettoby_wardmanNo ratings yet
- The Cactus and the SnowsDocument22 pagesThe Cactus and the SnowsCrisNo ratings yet
- Aam April 2023Document198 pagesAam April 2023Adhitya DewantaraNo ratings yet
- Ahmed Ali Alshehri Mobile 00966-508-217284 Address: P.O.Box 70132 Zipcode:31952 Riyadh Street, Al-Khobar, Saudi ArabiaDocument9 pagesAhmed Ali Alshehri Mobile 00966-508-217284 Address: P.O.Box 70132 Zipcode:31952 Riyadh Street, Al-Khobar, Saudi ArabiaShah KhalidNo ratings yet
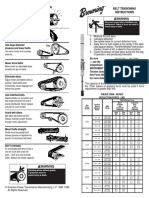
- Browning Belt Tension GaugeDocument2 pagesBrowning Belt Tension GaugeJasperken2xNo ratings yet
- Fundamentals of Wind EnergyDocument24 pagesFundamentals of Wind EnergyMas3odNo ratings yet
- Principles of Marketing - Product, Service and Experience DifferencesDocument26 pagesPrinciples of Marketing - Product, Service and Experience DifferencesVivien Leigh LopezNo ratings yet
- 2024 Drik Panchang Telugu Calendar v1.0.1Document25 pages2024 Drik Panchang Telugu Calendar v1.0.1Sreekara GsNo ratings yet
- Medical Terminology TermsDocument28 pagesMedical Terminology TermsNikka Moreen DagdagNo ratings yet
- Philips HD5 enDocument5 pagesPhilips HD5 enmohamed boufasNo ratings yet
- Rental Range Powered by YANMAR Diesel GeneratorDocument6 pagesRental Range Powered by YANMAR Diesel GeneratorJonathan CastilloNo ratings yet
- Training ManualDocument41 pagesTraining Manualemiliow_1100% (3)
- Magellans of The Sky - Prologue - Summer 2010Document12 pagesMagellans of The Sky - Prologue - Summer 2010Prologue MagazineNo ratings yet
- Assess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsDocument6 pagesAssess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsIJAR JOURNALNo ratings yet
- TheologicalDiscipleship English 2011-1Document144 pagesTheologicalDiscipleship English 2011-1bilnyangnatNo ratings yet
- Lab ReportDocument9 pagesLab ReportQi Yi TanNo ratings yet
- Design of Temporary Floating Road for Construction SiteDocument6 pagesDesign of Temporary Floating Road for Construction SiteAnonymous hRWwL7pZnCNo ratings yet
- Bernard BTB MIG GunsDocument8 pagesBernard BTB MIG GunsEdwin Mauricio Gallego OsorioNo ratings yet
- English HL Grade 8 Language Exam Nov 2017 MEMODocument12 pagesEnglish HL Grade 8 Language Exam Nov 2017 MEMOThegn's PicklesNo ratings yet
- BMK PDFDocument8 pagesBMK PDFHuỳnh Minh SángNo ratings yet
- Minitek Indore Profile 2Document9 pagesMinitek Indore Profile 2kunal agiwaleNo ratings yet
- CHAPTER-9, Respiration in Organisms.Document3 pagesCHAPTER-9, Respiration in Organisms.HarshitAhelani2379ScribdNo ratings yet
- Beneficiation of Cassiterite From Primary Tin OresDocument11 pagesBeneficiation of Cassiterite From Primary Tin OresSULMAGNo ratings yet
- BARACARBDocument2 pagesBARACARBYudha Satria50% (2)
- Tugas Bahasa Inggris-1Document8 pagesTugas Bahasa Inggris-1Nur KomariyahNo ratings yet
- Idioms and Phrases MCQs - English Grammar For Competitive ExamsDocument6 pagesIdioms and Phrases MCQs - English Grammar For Competitive ExamsgeologistlakhanNo ratings yet
- Bipolar I Disorder Case ExampleDocument6 pagesBipolar I Disorder Case ExampleGrape JuiceNo ratings yet