You might also like
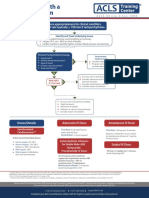
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612YassarNo ratings yet
- AdultTachycardiaWithPulse AlgorithmDocument1 pageAdultTachycardiaWithPulse AlgorithmIsmail SlimNo ratings yet
- 2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmRyggie ComelonNo ratings yet
- Tachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDocument1 pageTachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDendy Frannuzul RamadhanNo ratings yet
- AlgorithmACLStachycardiawithapulse PDFDocument1 pageAlgorithmACLStachycardiawithapulse PDFDendy Frannuzul RamadhanNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612must dietNo ratings yet
- Adult Tachycardia With A Pulse Algorithm: Doses/DetailsDocument1 pageAdult Tachycardia With A Pulse Algorithm: Doses/DetailsZakiyahulfahdwNo ratings yet
- Adult Tachycardia With A Pulse Algorithm: Doses/DetailsDocument1 pageAdult Tachycardia With A Pulse Algorithm: Doses/DetailsAlexis HospitalNo ratings yet
- Tachycardia AlgorythmDocument1 pageTachycardia AlgorythmUZNAPMNo ratings yet
- Algoritma Ambulance - PHCDocument11 pagesAlgoritma Ambulance - PHCYassarNo ratings yet
- Website Tachycardia Algorithm DiagramDocument1 pageWebsite Tachycardia Algorithm Diagramcolette zgheibNo ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFibbs91No ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFPlabber JuneNo ratings yet
- Adult Tachycardia (With Pulse) AlgorithmDocument1 pageAdult Tachycardia (With Pulse) AlgorithmJames ChoiNo ratings yet
- Managemen Disritmia: Dr. Rofika Hanifa, SPPDDocument20 pagesManagemen Disritmia: Dr. Rofika Hanifa, SPPDavivlabirdNo ratings yet
- Algoritmos AHA ACLS AdultoDocument4 pagesAlgoritmos AHA ACLS AdultoChristianFelipePorrasCastroNo ratings yet
- AlgorithmsDocument16 pagesAlgorithmsirish laglevaNo ratings yet
- Pediatric Tachycardia With A Pulse Algorithm: Yes NoDocument1 pagePediatric Tachycardia With A Pulse Algorithm: Yes NoRatna TambaNo ratings yet
- With A Pulse and Poor Perfusion: Pediatric TachycardiaDocument1 pageWith A Pulse and Poor Perfusion: Pediatric TachycardiaIin-Ignasia Diahayujulindah Mujiman0% (1)
- Obat-Obatan Dalam Bantuan Hidup LanjutDocument16 pagesObat-Obatan Dalam Bantuan Hidup LanjutTheresia SihotangNo ratings yet
- Tachycardia AlgorithmDocument1 pageTachycardia AlgorithmGideon BahuleNo ratings yet
- 5.ALS Algorithms TachycardiaDocument1 page5.ALS Algorithms TachycardiaMassimo Di BenedettoNo ratings yet
- ALS Algorithms LS Tachycardia 2.0Document1 pageALS Algorithms LS Tachycardia 2.0Lucian Alin DinuNo ratings yet
- Initial Recommended Doses NarrowDocument1 pageInitial Recommended Doses NarrowwisgeorgekwokNo ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- Adenosine: Scheduling BLS (CPR/First Aid) Acls PalsDocument4 pagesAdenosine: Scheduling BLS (CPR/First Aid) Acls PalsPhilippe Ceasar C. BascoNo ratings yet
- Pediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmDocument1 pagePediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmRadhiatul MardhiahNo ratings yet
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDocument1 pageACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniNo ratings yet
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pages3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- ACLS 2015 Guidelines Upate Nov 2016 For PostingDocument2 pagesACLS 2015 Guidelines Upate Nov 2016 For PostingOana - Andreea CristeaNo ratings yet
- Note: Dosage May Be Gradually Increased Over: AmlodipineDocument4 pagesNote: Dosage May Be Gradually Increased Over: Amlodipineanette katrinNo ratings yet
- Adult BradycardiaDocument1 pageAdult BradycardiaTista ApriyanaNo ratings yet
- ACLS Tachycardia Algorithm For Managing Stable TachycardiaDocument4 pagesACLS Tachycardia Algorithm For Managing Stable TachycardiaLady MuffinsNo ratings yet
- Cardiology Exam 2 - Lecture Notes: Treating Adult BradycardiaDocument5 pagesCardiology Exam 2 - Lecture Notes: Treating Adult BradycardiaAddieNo ratings yet
- Name of Drug Dosage/ Frequency / Timing/ Route Mechanism of Action Indication Contraindic Ation Adverse Effect Nursing ResponsibilitiesDocument3 pagesName of Drug Dosage/ Frequency / Timing/ Route Mechanism of Action Indication Contraindic Ation Adverse Effect Nursing ResponsibilitiesphoebeNo ratings yet
- Adult BradycardiaDocument1 pageAdult BradycardiaTista ApriyanaNo ratings yet
- Generic Name: Adult: IVDocument3 pagesGeneric Name: Adult: IVBasema HashhashNo ratings yet
- Dx. StudyDocument3 pagesDx. Studymayumitanaka8042No ratings yet
- Drug Study - AmlodipineDocument2 pagesDrug Study - AmlodipineKian HerreraNo ratings yet
- AdenosineDocument2 pagesAdenosinegovind_soni_150% (1)
- Algo Bradycardia DikonversiDocument5 pagesAlgo Bradycardia DikonversiDaniel SitungkirNo ratings yet
- Drug Classification of AmlodepineDocument5 pagesDrug Classification of Amlodepineshai raNo ratings yet
- Ecgs and Acute Cardiac Events: Yuniardi Alriyanto, MD Doris Sylvanus Hospital PalangkarayaDocument47 pagesEcgs and Acute Cardiac Events: Yuniardi Alriyanto, MD Doris Sylvanus Hospital PalangkarayaAuliaRusdiAllmuttaqienNo ratings yet
- Tachycardia Algorithm 2021Document1 pageTachycardia Algorithm 2021Ravin DebieNo ratings yet
- AlgorithmACLSBradycardiawithapulse PDFDocument1 pageAlgorithmACLSBradycardiawithapulse PDFjohndoe1995No ratings yet
- Pals Pediatric BradycardiaDocument1 pagePals Pediatric BradycardiadarlingcarvajalduqueNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- Ecg Dysrythmias Nursing Responsibilitu Sinus Node 1.) Sinus BradycardiaDocument2 pagesEcg Dysrythmias Nursing Responsibilitu Sinus Node 1.) Sinus BradycardiaNickha LazoNo ratings yet
- Pals TachycardiaDocument1 pagePals TachycardiadarlingcarvajalduqueNo ratings yet
- ACLS Drug TherapyDocument8 pagesACLS Drug TherapySahrensNo ratings yet
- Bradycardia AlgorithmDocument1 pageBradycardia AlgorithmGideon BahuleNo ratings yet
- DRUG STUDY ICU and ACSDocument22 pagesDRUG STUDY ICU and ACSSheila Mae ReyesNo ratings yet
- Drug Study On Emergency DrugsDocument28 pagesDrug Study On Emergency DrugsRaidis PangilinanNo ratings yet
- Nursing CS Treatment-Of-Atrial-Dysrhythmias 02Document1 pageNursing CS Treatment-Of-Atrial-Dysrhythmias 02frankshro156No ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- DRAFT V1.0 - 2/26/04: Memorandum of UnderstandingDocument4 pagesDRAFT V1.0 - 2/26/04: Memorandum of UnderstandingYudhistira AdiNo ratings yet
- Subject-Verb Agreement: Brenham Writing Room Created by D. HerringDocument13 pagesSubject-Verb Agreement: Brenham Writing Room Created by D. HerringYudhistira AdiNo ratings yet
- Dundee Epidemiology and Biostatistics Unit: Measures of AgreementDocument36 pagesDundee Epidemiology and Biostatistics Unit: Measures of AgreementYudhistira AdiNo ratings yet
- AP Graduate Admissions Form 2016Document4 pagesAP Graduate Admissions Form 2016Yudhistira AdiNo ratings yet
- Protocol AddendumDocument9 pagesProtocol AddendumYudhistira AdiNo ratings yet
- Quot Myanmar Type DDocument1 pageQuot Myanmar Type DYudhistira AdiNo ratings yet
- 160802Document1 page160802Yudhistira AdiNo ratings yet
- Graduate Instruction and Research in Astronomy at Bologna UniversityDocument25 pagesGraduate Instruction and Research in Astronomy at Bologna UniversityYudhistira AdiNo ratings yet
- Berdikari 2296Document1 pageBerdikari 2296Yudhistira AdiNo ratings yet
- Higgs Boson and Beyond:: The Quest For New Laws of PhysicsDocument1 pageHiggs Boson and Beyond:: The Quest For New Laws of PhysicsYudhistira AdiNo ratings yet
- Agreement On Cooperation in Astrophysics: Article 1Document9 pagesAgreement On Cooperation in Astrophysics: Article 1Yudhistira AdiNo ratings yet
- Higgs QNDocument40 pagesHiggs QNYudhistira AdiNo ratings yet
- 14.1 The Hole Inside The Heart ABSTRAKDocument11 pages14.1 The Hole Inside The Heart ABSTRAKYudhistira AdiNo ratings yet
- Case Report:: Cystic MeningiomaDocument11 pagesCase Report:: Cystic MeningiomaYudhistira AdiNo ratings yet
- Case ReportDocument8 pagesCase ReportYudhistira AdiNo ratings yet
- Introduction To Mobile RobotsDocument45 pagesIntroduction To Mobile RobotsSELVAKUMAR RNo ratings yet
- GEBCO's Global Gridded Bathymetric Data Sets: Seabed 2030 Project Nippon Foundation GebcoDocument13 pagesGEBCO's Global Gridded Bathymetric Data Sets: Seabed 2030 Project Nippon Foundation GebcoJulrialdinNo ratings yet
- Personal Action Plan PDFDocument28 pagesPersonal Action Plan PDFClaire ThrelfallNo ratings yet
- Ce1999 Cairo MetroDocument15 pagesCe1999 Cairo MetroPlannerNo ratings yet
- Music Tech Focus - Ableton Live - 2015-2016Document132 pagesMusic Tech Focus - Ableton Live - 2015-2016PDFingHellNo ratings yet
- Technical Report Format (MID SEMESTER 2021)Document13 pagesTechnical Report Format (MID SEMESTER 2021)Jay ParmaniNo ratings yet
- Evolution of Human-Natural System of Coast LandDocument329 pagesEvolution of Human-Natural System of Coast LandPasha FaishalNo ratings yet
- Douglas 2002 - Rockmasses Shear StrengthDocument543 pagesDouglas 2002 - Rockmasses Shear StrengthsamiNo ratings yet
- AIM CompaniesDocument48 pagesAIM CompaniesSanjay KoriNo ratings yet
- Lecture 10: Power-Flow Studies: Instructor: Dr. Gleb V. Tcheslavski Contact: Office HoursDocument28 pagesLecture 10: Power-Flow Studies: Instructor: Dr. Gleb V. Tcheslavski Contact: Office HoursAn00pgadzillaNo ratings yet
- Pleiger Tank Measuring SystemDocument12 pagesPleiger Tank Measuring SystemPamellaNo ratings yet
- (Ancient Peoples and Places) J. G. MacQueen - The Hittites - and Their Contemporaries in Asia Minor-Thames & Hudson (1986) PDFDocument184 pages(Ancient Peoples and Places) J. G. MacQueen - The Hittites - and Their Contemporaries in Asia Minor-Thames & Hudson (1986) PDFEfecan Anaz100% (1)
- Invoice ScissorsDocument1 pageInvoice ScissorsAlex ClunieNo ratings yet
- ME1202-Tutorial 2Document1 pageME1202-Tutorial 2manarajNo ratings yet
- Pythagoras' & Trigonometry Past Paper QuestionsDocument46 pagesPythagoras' & Trigonometry Past Paper QuestionsinternationalmakkhayarNo ratings yet
- Cereal CropsDocument34 pagesCereal CropsJe-ar ColipanoNo ratings yet
- Defense Laboratories and Centers: AFRL: Air Force Research LaboratoryDocument2 pagesDefense Laboratories and Centers: AFRL: Air Force Research LaboratoryIan S Ryu100% (1)
- CFI 3 Statement Model CompleteDocument9 pagesCFI 3 Statement Model CompleteMuhammadSiddiqNo ratings yet
- Madison County Inspection ReportsDocument5 pagesMadison County Inspection ReportsMike BrownNo ratings yet
- Power System Simulation Lab ManualDocument41 pagesPower System Simulation Lab ManualArivumani86% (14)
- Creating A Catalyst For Thinking The Integrated Curriculum PDFDocument212 pagesCreating A Catalyst For Thinking The Integrated Curriculum PDFhoangdongNo ratings yet
- Digital Image Processing: Lecture # 2 FundamentalsDocument41 pagesDigital Image Processing: Lecture # 2 FundamentalsAhsanNo ratings yet
- List SpecificationDocument10 pagesList Specificationpuri16No ratings yet
- EnglishDocument32 pagesEnglishVilitzaNo ratings yet
- Age of IndustrialisationDocument10 pagesAge of IndustrialisationsssssssssssNo ratings yet
- BD100 16Document57 pagesBD100 16stavros_stergNo ratings yet
- Medical Education - 2017 - Rossettini - Effective Teaching of Manual Skills To Physiotherapy Students A RandomisedDocument13 pagesMedical Education - 2017 - Rossettini - Effective Teaching of Manual Skills To Physiotherapy Students A Randomisedemad tawfiq ahmedNo ratings yet
- Ic Engines and Gas TurbineDocument3 pagesIc Engines and Gas TurbineLippin PaulyNo ratings yet
- Bexitrol F Dpi PDFDocument4 pagesBexitrol F Dpi PDFTahia Rahman JuhiNo ratings yet
- Thesis AcarDocument111 pagesThesis AcarSara CortezNo ratings yet