You might also like
- Drug Administration in Nursing: A Comprehensive Guide to Drug Administration and Calculation in NursingFrom EverandDrug Administration in Nursing: A Comprehensive Guide to Drug Administration and Calculation in NursingNo ratings yet
- Faculty of Medicine, Novi Sad, SerbiaDocument5 pagesFaculty of Medicine, Novi Sad, SerbiaAnkete FNo ratings yet
- European J Cancer Care - 2018 - Riu Viladoms - Drug Interactions With Oral Antineoplastic Drugs The Role of The PharmacistDocument5 pagesEuropean J Cancer Care - 2018 - Riu Viladoms - Drug Interactions With Oral Antineoplastic Drugs The Role of The PharmacistCatalina Del CantoNo ratings yet
- Reducing Inappropriate Polypharmacy The Process of DeprescribingDocument8 pagesReducing Inappropriate Polypharmacy The Process of DeprescribingThiago SartiNo ratings yet
- Reconciliacao MedicamentosaDocument22 pagesReconciliacao MedicamentosapchrispimNo ratings yet
- Translator Apr2010 Vo4 Iss1Document4 pagesTranslator Apr2010 Vo4 Iss1Vina Angga RiniNo ratings yet
- Article Wjpps 1469869064Document10 pagesArticle Wjpps 1469869064Lucia SibiiNo ratings yet
- Fvalin,+06 CBR 42.4 OA 120920Document8 pagesFvalin,+06 CBR 42.4 OA 120920Dani PurgananNo ratings yet
- Improving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientsDocument13 pagesImproving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientstotoksaptantoNo ratings yet
- Computerized ProgramDocument7 pagesComputerized ProgramfatiisaadatNo ratings yet
- Medication Error Patients Admitted To Medical Ward in Primary Hospital, Ethiopia: Prospective Obserbetional StudyDocument18 pagesMedication Error Patients Admitted To Medical Ward in Primary Hospital, Ethiopia: Prospective Obserbetional StudybezieNo ratings yet
- Evaluation of Drug Related Problems in Patients With Chronic Disease at Tertiary Care Teaching HospitalDocument12 pagesEvaluation of Drug Related Problems in Patients With Chronic Disease at Tertiary Care Teaching HospitalenesNo ratings yet
- Vol 51 No 2 01 Prevalence Med PDFDocument4 pagesVol 51 No 2 01 Prevalence Med PDFJustin VergaraNo ratings yet
- Polypharmacy and Drug-Related Problems Among People Living With HIV-AIDS - A Single-Center Experience (#577802) - 735759Document8 pagesPolypharmacy and Drug-Related Problems Among People Living With HIV-AIDS - A Single-Center Experience (#577802) - 735759LauraNo ratings yet
- Ractice Nsights: The Critical Care Pharmacist: An Essential Intensive Care PractitionerDocument5 pagesRactice Nsights: The Critical Care Pharmacist: An Essential Intensive Care PractitionerDaniela HernandezNo ratings yet
- Artigo 2Document13 pagesArtigo 2Paulo TononNo ratings yet
- The Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaDocument11 pagesThe Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaSabrina JonesNo ratings yet
- 1268 PDFDocument5 pages1268 PDFCMargs ConceptsNo ratings yet
- Medication Knowledge, Certainty, and Risk of Errors in Health Care: A Cross-Sectional StudyDocument9 pagesMedication Knowledge, Certainty, and Risk of Errors in Health Care: A Cross-Sectional Studymeci_asyikNo ratings yet
- Algoritma Terapi Diabetes MellitusDocument9 pagesAlgoritma Terapi Diabetes MellitusriniNo ratings yet
- 2021 DallAgnol PharmInterventions2yoncologypediatric11Document10 pages2021 DallAgnol PharmInterventions2yoncologypediatric11Dara PrameswariNo ratings yet
- Original 8Document5 pagesOriginal 8majedNo ratings yet
- 1642-Article Text-7699-1-10-20200623Document5 pages1642-Article Text-7699-1-10-20200623mtgnzgaNo ratings yet
- TugasDocument16 pagesTugaselsarahmiNo ratings yet
- Rubio Valera2013Document10 pagesRubio Valera2013Marcus Fábio leite AndradeNo ratings yet
- ED Drug Prescribing TrendsDocument6 pagesED Drug Prescribing TrendsNiranjan ChapagainNo ratings yet
- Article Group ADocument18 pagesArticle Group Alollipop1234556677No ratings yet
- Incidence of Intravenous Drug Incompatibilities in Intensive Care UnitsDocument5 pagesIncidence of Intravenous Drug Incompatibilities in Intensive Care UnitsNeliydaMayantiNo ratings yet
- Eraker 1984Document11 pagesEraker 1984Lorena PăduraruNo ratings yet
- Diya BetDocument10 pagesDiya BetDERYANo ratings yet
- 2018 - Baraki Et AlDocument8 pages2018 - Baraki Et AlazeemathmariyamNo ratings yet
- Pharmacist EvaluationDocument1 pagePharmacist Evaluationosama nagarNo ratings yet
- Impact of Clinical Pharmacy Services in A Hematology/Oncology Inpatient SettingDocument4 pagesImpact of Clinical Pharmacy Services in A Hematology/Oncology Inpatient SettingRaja Mia SeptiaNo ratings yet
- IntroductionDocument2 pagesIntroductionasaad biqaiNo ratings yet
- The Impact of Clinical Pharmacists InterDocument7 pagesThe Impact of Clinical Pharmacists Interahmed1fkwnNo ratings yet
- Medication Errors 111765Document7 pagesMedication Errors 111765akko aliNo ratings yet
- Drug Adverse Effects in Medicine Outpatient Department (AHMED TANJIMUL ISLAM)Document4 pagesDrug Adverse Effects in Medicine Outpatient Department (AHMED TANJIMUL ISLAM)AHMED TANJIMUL ISLAMNo ratings yet
- Adherence of PatientDocument5 pagesAdherence of PatientexaNo ratings yet
- Value of A Community-Based Medication ManagementDocument12 pagesValue of A Community-Based Medication ManagementGetrudeNo ratings yet
- An Electronic Adherence Measurement Intervention To Reduce Clinical Inertia in The Treatment of Uncontrolled Hypertension - The MATCH Cluster Randomized Clinical TrialDocument7 pagesAn Electronic Adherence Measurement Intervention To Reduce Clinical Inertia in The Treatment of Uncontrolled Hypertension - The MATCH Cluster Randomized Clinical TrialcharmyshkuNo ratings yet
- Adverse Drug Reactions in Elderly: Challenges in Identification and Improving Preventative StrategiesDocument3 pagesAdverse Drug Reactions in Elderly: Challenges in Identification and Improving Preventative StrategiesManik WidariNo ratings yet
- Pediatric Anesthesiology Fellows' Perception of Quality of Attending Supervision and Medical ErrorsDocument5 pagesPediatric Anesthesiology Fellows' Perception of Quality of Attending Supervision and Medical ErrorsGio VandaNo ratings yet
- Adverse Drug Reactions in Elderly: Challenges in Identification and Improving Preventative StrategiesDocument3 pagesAdverse Drug Reactions in Elderly: Challenges in Identification and Improving Preventative StrategiesManik WidariNo ratings yet
- Critical Incident AnalysisDocument5 pagesCritical Incident Analysiszaim tech33% (3)
- Risk ManagementDocument6 pagesRisk Managementfaizanquresi12No ratings yet
- Wu 2008Document12 pagesWu 2008JoseNo ratings yet
- Chakelba 2013Document9 pagesChakelba 2013Nawang WulanNo ratings yet
- 2000, Antonow J. Medication Error Reporting PediatriaDocument7 pages2000, Antonow J. Medication Error Reporting PediatriaFilipa Salvador SalvadorNo ratings yet
- Decentralized Pharmacist' ServicesDocument21 pagesDecentralized Pharmacist' ServicesRaju NiraulaNo ratings yet
- Abughosh Et Al 2017 A Motivational Interviewing Intervention by Pharmacy Students To Improve Medication AdherenceDocument12 pagesAbughosh Et Al 2017 A Motivational Interviewing Intervention by Pharmacy Students To Improve Medication AdherenceKat HerNo ratings yet
- JurnalDocument7 pagesJurnalZulfa SalsabellaNo ratings yet
- Reducing Medication Errors in HospitalsDocument9 pagesReducing Medication Errors in Hospitalsakko aliNo ratings yet
- Article Without AbstractDocument8 pagesArticle Without AbstractEinshtabbaniNo ratings yet
- JC2Document15 pagesJC2Taory AnisNo ratings yet
- A Systematic Review On Medication Errors 2015Document3 pagesA Systematic Review On Medication Errors 2015Trang Hoàng ThịNo ratings yet
- Improving Primary Care in Rural Alabama With A Pharmacy InitiativeDocument7 pagesImproving Primary Care in Rural Alabama With A Pharmacy InitiativeBasilharbi HammadNo ratings yet
- Fernandes Medication Reconciliation Practical Tips Strategies and Tools For PharmacistsDocument10 pagesFernandes Medication Reconciliation Practical Tips Strategies and Tools For PharmacistsEvianti Dwi AgustinNo ratings yet
- Clinically Relevant Pharmacokinetic Knowledge On Antibiotic Dosing Among Intensive Care Professionals Is Insufficient: A Cross-Sectional StudyDocument9 pagesClinically Relevant Pharmacokinetic Knowledge On Antibiotic Dosing Among Intensive Care Professionals Is Insufficient: A Cross-Sectional StudyNguyễn Đức LongNo ratings yet
- Pharm Paper FinalDocument8 pagesPharm Paper FinalAnamta AkhtarNo ratings yet
- A Study To Assess The Impact of Pharmaceutical Care Services To Cancer Patients in A Tertiary Care HospitalDocument10 pagesA Study To Assess The Impact of Pharmaceutical Care Services To Cancer Patients in A Tertiary Care HospitalRaya PambudhiNo ratings yet
- Can Low-Fat Nutrition Labels Lead To Obesity PDFDocument15 pagesCan Low-Fat Nutrition Labels Lead To Obesity PDFSepti Lidya sariNo ratings yet
- Ocean Quest SSD Trainer Manual 2020Document109 pagesOcean Quest SSD Trainer Manual 2020Carmen LuckNo ratings yet
- Carestation 600 SeriesDocument3 pagesCarestation 600 SeriesABHINANDAN SHARMANo ratings yet
- Good WSH Practices Pictograms: Guide ToDocument7 pagesGood WSH Practices Pictograms: Guide Tobob juanNo ratings yet
- Growing Uganda's mushroom farming industryDocument2 pagesGrowing Uganda's mushroom farming industrymaboni ismaelNo ratings yet
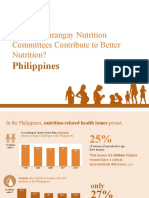
- How Do Barangay Nutrition Committees Contribute To Better Nutrition?Document20 pagesHow Do Barangay Nutrition Committees Contribute To Better Nutrition?Angelito CortunaNo ratings yet
- Beliefs About Obsessional Thoughts InventoryDocument21 pagesBeliefs About Obsessional Thoughts InventoryMarta CerdáNo ratings yet
- Journal Pre-Proof: Gait & PostureDocument35 pagesJournal Pre-Proof: Gait & PostureRogerDelaCernaNo ratings yet
- Tagaytay Es - Annex ADocument4 pagesTagaytay Es - Annex AEduardoAlejoZamoraJr.No ratings yet
- Alexthymia in Sexual Disorder Clinic PatientsDocument7 pagesAlexthymia in Sexual Disorder Clinic PatientsFélix Aníbal Acuña OlivosNo ratings yet
- IBH 6111 Final PresentationDocument13 pagesIBH 6111 Final PresentationSidney OxboroughNo ratings yet
- Effect of Ethanol Leaf Extract of Chromolaena Odorata On Lipid Profile of Streptozotocin Induced Diabetic Wistar Albino RatsDocument9 pagesEffect of Ethanol Leaf Extract of Chromolaena Odorata On Lipid Profile of Streptozotocin Induced Diabetic Wistar Albino RatsPUBLISHER JOURNALNo ratings yet
- ExampleDocument12 pagesExampleEmma May De MesaNo ratings yet
- Mikkelsen 2017 Diários em Crianças Estudo QualitativoDocument6 pagesMikkelsen 2017 Diários em Crianças Estudo QualitativoGabriela LealNo ratings yet
- Weeks 3 & 4 - Oral CommunicationDocument7 pagesWeeks 3 & 4 - Oral CommunicationClaire CaraigNo ratings yet
- Pelvic Organ Prolapse After Laparoscopic Hysterectomy Compared With Vaginal Hysterectomy: The POP-UP StudyDocument10 pagesPelvic Organ Prolapse After Laparoscopic Hysterectomy Compared With Vaginal Hysterectomy: The POP-UP Studymuhammadnurul asmiNo ratings yet
- NuRS 115 ResearchDocument15 pagesNuRS 115 ResearchD-Babygirl BlessedShorty DonnaNo ratings yet
- Curriculum Vitae: Amir E. Ibrahim, M.DDocument11 pagesCurriculum Vitae: Amir E. Ibrahim, M.DkendoNo ratings yet
- Ethics in DentistryDocument4 pagesEthics in DentistryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Writing Sample 2Document9 pagesWriting Sample 2api-582848179No ratings yet
- A Concept-Based Approach To Learning: DevelopmentDocument62 pagesA Concept-Based Approach To Learning: DevelopmentAli Nawaz AyubiNo ratings yet
- Uber CEO EmailDocument5 pagesUber CEO EmailKhristopher J. BrooksNo ratings yet
- Roth - From Free WombDocument19 pagesRoth - From Free WombNubss SSNo ratings yet
- Conceptual Understanding of OptimismDocument8 pagesConceptual Understanding of OptimismUDITA PARIKHNo ratings yet
- Patient's Profile: Doña Remedios Trinidad Romualdez Medical Foundation, Inc. 2 Semester, S.Y. 2020-2021Document16 pagesPatient's Profile: Doña Remedios Trinidad Romualdez Medical Foundation, Inc. 2 Semester, S.Y. 2020-2021Royce Vincent TizonNo ratings yet
- Ppt-Project Management Baia MareDocument35 pagesPpt-Project Management Baia MareMarchiș AlexandraNo ratings yet
- Leica Cryostat 1860 ManualDocument98 pagesLeica Cryostat 1860 ManualEmilio Fernandez LimónNo ratings yet
- Network QatarDocument48 pagesNetwork QatarMark NahasNo ratings yet
- 6.11 Bullying ReadyDocument41 pages6.11 Bullying ReadyAstraX EducationNo ratings yet
- Term Paper TitlesDocument6 pagesTerm Paper TitlesGOOD BATA WAY BITOKNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- Embrace Your Weird: Face Your Fears and Unleash CreativityFrom EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityRating: 4.5 out of 5 stars4.5/5 (124)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerFrom EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerRating: 4.5 out of 5 stars4.5/5 (16)
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)
- The Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.From EverandThe Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.Rating: 5 out of 5 stars5/5 (14)
- Triggers: How We Can Stop Reacting and Start HealingFrom EverandTriggers: How We Can Stop Reacting and Start HealingRating: 5 out of 5 stars5/5 (58)