You might also like
- SmofKabiven DetailsDocument21 pagesSmofKabiven DetailskelgroryNo ratings yet
- Follow Up LabDocument2 pagesFollow Up LabnellieauthorNo ratings yet
- Neutralizer ChartDocument1 pageNeutralizer ChartJUAN FELIPE ORTIZ PARRANo ratings yet
- Divisi Nutrisi dan Penyakit Metabolik Susu HipoalergenikDocument13 pagesDivisi Nutrisi dan Penyakit Metabolik Susu HipoalergenikIndah KhairaniNo ratings yet
- Update MSDSDocument10 pagesUpdate MSDSShabir MansuriNo ratings yet
- Kilauea Major ElementsDocument17 pagesKilauea Major ElementsRennyCahyanyTrijayaNo ratings yet
- Aqueous Solubility of Inorganic Compounds at Various TemperaturesDocument9 pagesAqueous Solubility of Inorganic Compounds at Various TemperaturesterrorfordNo ratings yet
- Final Dairy NoteDocument230 pagesFinal Dairy NoteRahul SenchuriNo ratings yet
- Properties of Amino Acids: M T, PK, PKDocument2 pagesProperties of Amino Acids: M T, PK, PKantonioNo ratings yet
- Common Impurities in NMR PDFDocument2 pagesCommon Impurities in NMR PDFhirjosh15No ratings yet
- Indeks PolaritasDocument15 pagesIndeks PolaritasIga PramuditaNo ratings yet
- F&EI Calculation WorkbookDocument43 pagesF&EI Calculation WorkbookAchmad RahmawanNo ratings yet
- Grafcbn 12Document1 pageGrafcbn 12khoirul abidinNo ratings yet
- Berries and Health Review: Evidence of BenefitsDocument20 pagesBerries and Health Review: Evidence of BenefitsAndreea CraciunNo ratings yet
- Susu Hipoalergenik Nutrisi KomparatifDocument13 pagesSusu Hipoalergenik Nutrisi KomparatifIndah KhairaniNo ratings yet
- No. Jenis Tes B. B B.A Rerata h1 h2 h3 h4Document5 pagesNo. Jenis Tes B. B B.A Rerata h1 h2 h3 h4Laboratorium KlinikNo ratings yet
- Natrium Taurokolat Leticin Glyceryl Mono-Oleat Natrium Oleat Pankreatin KH Po Nah PoDocument7 pagesNatrium Taurokolat Leticin Glyceryl Mono-Oleat Natrium Oleat Pankreatin KH Po Nah PoViviane AnnisaNo ratings yet
- Limited Asam Amino Thurain PunyaDocument1 pageLimited Asam Amino Thurain PunyaThurain LeoNo ratings yet
- Kabiven G11 PIDocument13 pagesKabiven G11 PIMeidistya Ayu MardhianiNo ratings yet
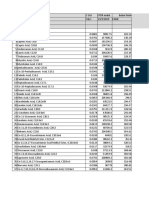
- Most Up-To-Date Table Is Available From: Internet E-Mail Last Update 20-Feb-03Document7 pagesMost Up-To-Date Table Is Available From: Internet E-Mail Last Update 20-Feb-03Saddy KhanNo ratings yet
- N O R M: TotalDocument6 pagesN O R M: TotalAntonioMissonGodoyGodoyNo ratings yet
- Nutritive Value of Indian Foods (IFCT) C. GopalanDocument21 pagesNutritive Value of Indian Foods (IFCT) C. Gopalanxinc.192007No ratings yet
- NMR Chemical Shifts of Common ImpuritiesDocument19 pagesNMR Chemical Shifts of Common ImpuritiesSana IqbalNo ratings yet
- Anorthite Hydrolysis: Mike Borr Geol 428 Geochemistry NDSU Fall 2012Document25 pagesAnorthite Hydrolysis: Mike Borr Geol 428 Geochemistry NDSU Fall 2012yuri huamanguillas saenzNo ratings yet
- Book1(AutoRecovered)Document9 pagesBook1(AutoRecovered)ritokaizeniiiiiNo ratings yet
- Susu HipoalergenikDocument14 pagesSusu HipoalergenikStella NoviaNo ratings yet
- Lampiran TDPKDocument17 pagesLampiran TDPKAnas GhozaliNo ratings yet
- Solvent Physical PropertiesDocument1 pageSolvent Physical PropertiesJaime Alejandro Martinez AcostaNo ratings yet
- Cangrejos Batholit and PorphyryDocument8 pagesCangrejos Batholit and PorphyryJohn F. Cerron ZarccoNo ratings yet
- Producto Rotacion Rentabilidad: % Part. % PartDocument2 pagesProducto Rotacion Rentabilidad: % Part. % Partfrank lopezNo ratings yet
- COA for Certified Reference Material OREAS 503eDocument24 pagesCOA for Certified Reference Material OREAS 503eHugo RodriguezNo ratings yet
- Corrections To Static BookDocument6 pagesCorrections To Static Bookmrullah1984No ratings yet
- Cacao So La TablasDocument10 pagesCacao So La Tablaskaoru9010-1No ratings yet
- Nutritional Composition: Values From 2003-2004 Feedstuffs Ingredient Analysis Table: Nick M. Dale and Amy B. BatalDocument2 pagesNutritional Composition: Values From 2003-2004 Feedstuffs Ingredient Analysis Table: Nick M. Dale and Amy B. Batalasole azoxNo ratings yet
- Acidbase ConcDocument1 pageAcidbase ConcAaron ParkinsonNo ratings yet
- 1-Mix Design UHPGC (W-B (0.35) (Ca 0.3) - Effect of MolarityDocument93 pages1-Mix Design UHPGC (W-B (0.35) (Ca 0.3) - Effect of MolaritySawa Zayia MichaelNo ratings yet
- Glaze ForwardDocument24 pagesGlaze Forwardaonegodman100% (2)
- Bam m384b eDocument6 pagesBam m384b eterecuaNo ratings yet
- NMR Chemical Shifts of Impurities ChartsDocument6 pagesNMR Chemical Shifts of Impurities ChartsNozha HammamiNo ratings yet
- Watch a video and write sentences about a familyDocument3 pagesWatch a video and write sentences about a familyJhon Villajuan LlactaNo ratings yet
- CHEM Experiment 7Document11 pagesCHEM Experiment 7Mary Gencel EstrellaNo ratings yet
- A. Identification of Unknown Amino Acid by Titration 1. Titration of The Unknown Amino Acid Vol. Naoh, ML PH Vol. Naoh, ML PHDocument4 pagesA. Identification of Unknown Amino Acid by Titration 1. Titration of The Unknown Amino Acid Vol. Naoh, ML PH Vol. Naoh, ML PHJohn Francis FernandezNo ratings yet
- Standard Chemical Exergy SubstancesDocument8 pagesStandard Chemical Exergy SubstancesKESAVARAPU UMA SAI MAHESHNo ratings yet
- Tabel Asam LemakDocument9 pagesTabel Asam Lemakdony abram simanjuntakNo ratings yet
- Amino AcidsDocument2 pagesAmino AcidsArkapravo ChattopadhyayNo ratings yet
- Properties of Common Liquids Solids and Foods 2Document2 pagesProperties of Common Liquids Solids and Foods 2Šhëënà de LeonNo ratings yet
- Raw Mix Design-Dalmia Cement LimitedDocument2 pagesRaw Mix Design-Dalmia Cement LimitedNihar Ranjan Tripathy50% (2)
- Determination of Titratable Acidity in White Wine Using Standard and Potentiometric MethodsDocument17 pagesDetermination of Titratable Acidity in White Wine Using Standard and Potentiometric MethodsKannan RanganathanNo ratings yet
- Titulação Ácido Glutâmico: V Naoh (ML) Eq Naoh (ML) PHDocument5 pagesTitulação Ácido Glutâmico: V Naoh (ML) Eq Naoh (ML) PHMonick CruzNo ratings yet
- NV (Table 1)Document12 pagesNV (Table 1)abigeevel2000No ratings yet
- OREAS 928 CertificateDocument11 pagesOREAS 928 CertificateGilang PamungkasNo ratings yet
- Requerimientos de Calidad 2008 95%, 97% y 99%Document18 pagesRequerimientos de Calidad 2008 95%, 97% y 99%emmanuel alonsoNo ratings yet
- OREAS 999 CertificateDocument17 pagesOREAS 999 Certificatepatriciad08652986No ratings yet
- Soalan Test 3 Semester 2 Sesi 2022 - 2023Document8 pagesSoalan Test 3 Semester 2 Sesi 2022 - 2023y15zrcdu1823No ratings yet
- 2017 09 17 - Periodic Trends Spreadsheet StudentDocument8 pages2017 09 17 - Periodic Trends Spreadsheet StudentKennyChiangNo ratings yet
- Microwave digestion atomic absorption method for metals in foodsDocument3 pagesMicrowave digestion atomic absorption method for metals in foodsJuan Felipe Romero RojasNo ratings yet
- Carbonated Soft Drinks: Formulation and ManufactureFrom EverandCarbonated Soft Drinks: Formulation and ManufactureDr. David SteenNo ratings yet
- Ionic Equilibria: pH CalculationsDocument37 pagesIonic Equilibria: pH CalculationsUchiha YogesNo ratings yet
- Astm D 2896Document8 pagesAstm D 2896waqas ahmad100% (1)
- CP 4Document6 pagesCP 4Yaping ZhangNo ratings yet
- Esomeprazole Magnesium Dihydrate EP 11.0Document3 pagesEsomeprazole Magnesium Dihydrate EP 11.0noschNo ratings yet
- SWAS Presentation1Document15 pagesSWAS Presentation1ranjaniNo ratings yet
- Metales Pesados Ph. Eur.Document4 pagesMetales Pesados Ph. Eur.sarasaNo ratings yet
- Acid Base Equilibria and Application PDFDocument32 pagesAcid Base Equilibria and Application PDFNicole Ann Pedriña100% (1)
- REAGENTS AND CONSUMABLES FOR LABORATORY EQUIPMENTDocument86 pagesREAGENTS AND CONSUMABLES FOR LABORATORY EQUIPMENTAjish joNo ratings yet
- JBL Brochure Biotope Aquarium Water en PDFDocument21 pagesJBL Brochure Biotope Aquarium Water en PDFGeorge PotoleaNo ratings yet
- Buffers Notes1Document3 pagesBuffers Notes1Lara MonevaNo ratings yet
- HBPH Ammonia Detetion in Brine v2Document2 pagesHBPH Ammonia Detetion in Brine v2MaxiwendelNo ratings yet
- Chemistry Course Outline SLDocument18 pagesChemistry Course Outline SLpuneetaNo ratings yet
- D 4319 - 93 Standard Test Method For KD Batch TestDocument7 pagesD 4319 - 93 Standard Test Method For KD Batch TestJ_BellineNo ratings yet
- Laboratory Equipment and Procedures ExamDocument6 pagesLaboratory Equipment and Procedures ExamJose Marie AsuncionNo ratings yet
- Lab Report IonizationDocument6 pagesLab Report IonizationJasmeetSinghNo ratings yet
- Generic Name: Suspension: Calcium Phosphate & Vitamin-D3 Composition:-Each 5ml ContainsDocument2 pagesGeneric Name: Suspension: Calcium Phosphate & Vitamin-D3 Composition:-Each 5ml Containsiloveit52252No ratings yet
- Sucrose/D-Glucose: Test-Combination For 22 Determinations EachDocument6 pagesSucrose/D-Glucose: Test-Combination For 22 Determinations EachVeronica DrgNo ratings yet
- WTW SenTix 940 - pH-GolderDocument8 pagesWTW SenTix 940 - pH-GolderAlexander Alza ZamudioNo ratings yet
- Solutions AIATS Medical-2018 (RM) Test-2 (Code-E & F) (17!12!2017)Document12 pagesSolutions AIATS Medical-2018 (RM) Test-2 (Code-E & F) (17!12!2017)Deeksha pathak100% (2)
- Analytical Chemistry I Laboratory Manual - 001Document30 pagesAnalytical Chemistry I Laboratory Manual - 001Chacha AlexNo ratings yet
- Develop soil salinity and pH monitoring systemDocument10 pagesDevelop soil salinity and pH monitoring systemShubham PaliwalNo ratings yet
- Offset Printing - The Dampening System PDFDocument87 pagesOffset Printing - The Dampening System PDFNBA100% (2)
- Investigating Factors that Affect Fat Hydrolysis RatesDocument4 pagesInvestigating Factors that Affect Fat Hydrolysis RatesAjay Rawat100% (1)
- Cambridge International Advanced Subsidiary and Advanced LevelDocument8 pagesCambridge International Advanced Subsidiary and Advanced LevelAfrina FatihahNo ratings yet
- Factors affecting boiling points and melting points of organic compoundsDocument5 pagesFactors affecting boiling points and melting points of organic compoundsARIAR, Jyllianne Kyla C.No ratings yet
- Electrochemical Study of A Commercial SoapDocument4 pagesElectrochemical Study of A Commercial Soap12jagNo ratings yet
- Assessmentofgroundwaterqualityusing GISin Thane Municipal Corporation Maharashtra IndiaDocument14 pagesAssessmentofgroundwaterqualityusing GISin Thane Municipal Corporation Maharashtra IndiaShoonyaNo ratings yet
- Antibiotic working concentrations catalog numbersDocument1 pageAntibiotic working concentrations catalog numbersBodhi DharmaNo ratings yet
- Limestone Dissolution in FGD Effect of Sulfite RochelleDocument11 pagesLimestone Dissolution in FGD Effect of Sulfite RochellemsoyoralNo ratings yet
- B. Protons and Neutrons: General ChemistryDocument76 pagesB. Protons and Neutrons: General ChemistryAmpolNo ratings yet