You might also like
- Koch 2010Document6 pagesKoch 2010groot marvelNo ratings yet
- Prevalence of Hepatitis B Virus Infection and Related Risk Factors in A Rural Community of MexicoDocument5 pagesPrevalence of Hepatitis B Virus Infection and Related Risk Factors in A Rural Community of MexicoEmmanuel LawerNo ratings yet
- V32n3a07 217-25Document9 pagesV32n3a07 217-25Tejinder SinghNo ratings yet
- Perfil de Personas Con Infección Por VIH/SIDA: Diferencial Étnico, Económico y Socio-Cultural en ChileDocument7 pagesPerfil de Personas Con Infección Por VIH/SIDA: Diferencial Étnico, Económico y Socio-Cultural en ChileGerty Steffany López RichterNo ratings yet
- 5365 Project FinalDocument13 pages5365 Project FinalDIVYA RANI KOLLINo ratings yet
- Lopez2006 PDFDocument11 pagesLopez2006 PDFMarcos AndradaNo ratings yet
- Under Five and Infant Mortality in ChileDocument17 pagesUnder Five and Infant Mortality in ChileuctimousprimeNo ratings yet
- Incidence of Chilhood Cancer in LatinoamericaDocument12 pagesIncidence of Chilhood Cancer in Latinoamericazuloagaisabel6No ratings yet
- Cardenas-Cardenas-2015-Maternal Mortality IDocument14 pagesCardenas-Cardenas-2015-Maternal Mortality Iangel.paternina423No ratings yet
- An Epidemiologic Analysis of Diabetes in Colombi 2015 Annals of Global HealtDocument12 pagesAn Epidemiologic Analysis of Diabetes in Colombi 2015 Annals of Global HealtarmanNo ratings yet
- Salud Publica 14Document8 pagesSalud Publica 14JavierPenagosNo ratings yet
- Research Proposal FinalDocument13 pagesResearch Proposal Finalapi-326037307No ratings yet
- Descripción Epidemiológica de La Mortalidad Por Cáncer de Mama en Mujeres en ChileDocument9 pagesDescripción Epidemiológica de La Mortalidad Por Cáncer de Mama en Mujeres en ChileJuan Pablo OyarzunNo ratings yet
- 01 - Estudio Chileno de Prevalencia Dr. VIcenteDocument9 pages01 - Estudio Chileno de Prevalencia Dr. VIcenteJuan M LavadosNo ratings yet
- Child Cohort StudiesDocument13 pagesChild Cohort Studiesk_dias6701No ratings yet
- The Impact of Social Vulnerability On COVID-19 in The U.S.: An Analysis of Spatially Varying RelationshipsDocument9 pagesThe Impact of Social Vulnerability On COVID-19 in The U.S.: An Analysis of Spatially Varying RelationshipsAdheni RezaNo ratings yet
- Sexual Behavior - Challenges For Prevention and Control Among Medical Students in MexicoDocument9 pagesSexual Behavior - Challenges For Prevention and Control Among Medical Students in MexicoMiguel BoonaparteNo ratings yet
- Reading Tests For OetDocument17 pagesReading Tests For OetJohn Cao72% (29)
- Necessary Conditions For Restarting LAUSD SCHOOLS IN 2020-2021Document1 pageNecessary Conditions For Restarting LAUSD SCHOOLS IN 2020-2021Ari El VoyagerNo ratings yet
- National, Regional, and Global Causes of Mortality in 5-19-Year-Olds From 2000 To 2019: A Systematic AnalysisDocument11 pagesNational, Regional, and Global Causes of Mortality in 5-19-Year-Olds From 2000 To 2019: A Systematic AnalysisXingran ChenNo ratings yet
- The Adult Mortality Profile by Cause of Death in 10 Latin American Countries (2000-2016)Document9 pagesThe Adult Mortality Profile by Cause of Death in 10 Latin American Countries (2000-2016)Diego Felipe Herrera ParraNo ratings yet
- International Review of Psychiatry 2010 22 (4) 355-362Document8 pagesInternational Review of Psychiatry 2010 22 (4) 355-362Rodrigo Chamorro OschilewskyNo ratings yet
- Chapter 1 Reproductive Health EpidemiologyyDocument13 pagesChapter 1 Reproductive Health EpidemiologyyAnnisa NurrachmawatiNo ratings yet
- Jurnal Study AsmaDocument1 pageJurnal Study AsmaIndri PuspasariNo ratings yet
- Measurement in EpidemiologyDocument14 pagesMeasurement in EpidemiologySaluja Chettri PradhanNo ratings yet
- Diseases of Poverty: Epidemiology, Infectious Diseases, and Modern PlaguesFrom EverandDiseases of Poverty: Epidemiology, Infectious Diseases, and Modern PlaguesNo ratings yet
- At The Intersection of Health, Health Care and PolicyDocument9 pagesAt The Intersection of Health, Health Care and PolicyxaxuelmcNo ratings yet
- Literature Review On Infant Mortality RateDocument4 pagesLiterature Review On Infant Mortality Rateaflsjfmwh100% (1)
- 0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesDocument11 pages0.1 Chapter 1 - Overview of Public Health Nursing in The Philippinesaajeno10No ratings yet
- 0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesDocument11 pages0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesJerreca DasasNo ratings yet
- Epidemiology MCH 101Document96 pagesEpidemiology MCH 101Christiaan Gaye B. PilayNo ratings yet
- Chapter 2 Covid 19 Pandemic and Global Demography Handout SimplifiedDocument3 pagesChapter 2 Covid 19 Pandemic and Global Demography Handout SimplifiedGil TolentinoNo ratings yet
- Module 2Document3 pagesModule 2Annie JoeNo ratings yet
- Understanding Mapuche-Williche Conceptions of Diabetes Mellitus and Arterial Hypertension From The Perspective of Intercultural HealthDocument10 pagesUnderstanding Mapuche-Williche Conceptions of Diabetes Mellitus and Arterial Hypertension From The Perspective of Intercultural HealthSergio Hernan Bermedo MuñozNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptjimakosjpNo ratings yet
- 1 Ehp3889Document9 pages1 Ehp3889MichelleNo ratings yet
- Diabetes Prevention Knowledge and Perception of Risk AmongDocument7 pagesDiabetes Prevention Knowledge and Perception of Risk AmongMuhammad AgussalimNo ratings yet
- Fiches Cours AnglaisDocument8 pagesFiches Cours AnglaisaxelleolieroNo ratings yet
- Burden of Disease-Implications For Future ResearchDocument5 pagesBurden of Disease-Implications For Future ResearchKaren Lizette ÑañezNo ratings yet
- Homicides in Mexico Reversed Life Expectancy Gains For Men and Slowed Them For Women, 2000 - 10Document8 pagesHomicides in Mexico Reversed Life Expectancy Gains For Men and Slowed Them For Women, 2000 - 10javiNo ratings yet
- Epidemiology and Prevention of Cancer: LearningDocument20 pagesEpidemiology and Prevention of Cancer: LearningWeiLinNo ratings yet
- Case Control Study of Risk Factors For Meningococcal Disease in ChileDocument9 pagesCase Control Study of Risk Factors For Meningococcal Disease in ChilemateusglehnNo ratings yet
- DMGS SSK 12982.editedDocument7 pagesDMGS SSK 12982.editedSreeparna ChandaNo ratings yet
- Jawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthDocument18 pagesJawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthIvan OliveiraNo ratings yet
- 2022-11 SUEMOTO Et Al - Risk Factors For Dementia in Brazil Differences by RegionDocument9 pages2022-11 SUEMOTO Et Al - Risk Factors For Dementia in Brazil Differences by Regionbcjbc7wxxpNo ratings yet
- Art:10.1186/1475 2891 12 69Document11 pagesArt:10.1186/1475 2891 12 69Ocha24 TupamahuNo ratings yet
- COVID 19 Recession Young Adult Food Insecurity, RDocument9 pagesCOVID 19 Recession Young Adult Food Insecurity, Rmohd zakirNo ratings yet
- Desigualdad Socioeconómica y Salud en MéxicoDocument12 pagesDesigualdad Socioeconómica y Salud en MéxicoAmisadai LugoNo ratings yet
- Low Latino Immunization Rates E-Portfolio 3Document7 pagesLow Latino Immunization Rates E-Portfolio 3api-300678072No ratings yet
- Años de Vida Perdidos Por Muerte Prematura (AVPP) en Adultos Del Gran Santiago ¿Hemos Ganado Con Equidad?Document8 pagesAños de Vida Perdidos Por Muerte Prematura (AVPP) en Adultos Del Gran Santiago ¿Hemos Ganado Con Equidad?Nay OviedoNo ratings yet
- Equidad de Genero en El AccesoDocument18 pagesEquidad de Genero en El AccesoAlejandra BeecheNo ratings yet
- Mental Disorders in Megacities: Findings From The Sa o Paulo Megacity Mental Health Survey, BrazilDocument11 pagesMental Disorders in Megacities: Findings From The Sa o Paulo Megacity Mental Health Survey, BrazilrafafenixsNo ratings yet
- Chapter 7 Human Population and EnvironmentDocument16 pagesChapter 7 Human Population and Environmentjieeniola1No ratings yet
- 10.1007@s12094 019 02107 WDocument6 pages10.1007@s12094 019 02107 WUzi SuruziNo ratings yet
- Asthma in The AmericasDocument11 pagesAsthma in The Americasthamires.assis.medNo ratings yet
- Population Dynamics & Processes: Birth, or Fertility, RatesDocument9 pagesPopulation Dynamics & Processes: Birth, or Fertility, RatesSamantha Ann T. TirthdasNo ratings yet
- Journal Pone 0275333Document15 pagesJournal Pone 0275333Nagilane ParenteNo ratings yet
- Knowledge, Attitudes and Practices On HIV/AIDS and Prevalence of HIV in The General Population of Sucre, BoliviaDocument13 pagesKnowledge, Attitudes and Practices On HIV/AIDS and Prevalence of HIV in The General Population of Sucre, BoliviaRima AnggreniNo ratings yet
- Unit 1 Dynamics of PopulationDocument29 pagesUnit 1 Dynamics of PopulationEngr. Karam AwanNo ratings yet
- Alleged Illtreatment of A Pauper at Lambeth Workhouse 1868Document1 pageAlleged Illtreatment of A Pauper at Lambeth Workhouse 1868groot marvelNo ratings yet
- Honeyman 2010Document45 pagesHoneyman 2010groot marvelNo ratings yet
- Off-Label Drugs (Gonzalez, 2008)Document33 pagesOff-Label Drugs (Gonzalez, 2008)Irfan AlviNo ratings yet
- Wilke 1997Document14 pagesWilke 1997groot marvelNo ratings yet
- Wilke 1997Document14 pagesWilke 1997groot marvelNo ratings yet
- Panter 2000Document8 pagesPanter 2000groot marvelNo ratings yet
- MahaDocument244 pagesMahagroot marvelNo ratings yet
- NSE Annual Report 2022-23-0 - 0Document436 pagesNSE Annual Report 2022-23-0 - 0groot marvelNo ratings yet
- Vaughn, Eve - ObsessedDocument229 pagesVaughn, Eve - Obsessedgroot marvelNo ratings yet
- Luther-Burbank - How-plants-Are-train (Volume 2) GRAFTING and BUDDING. (Volume 2)Document460 pagesLuther-Burbank - How-plants-Are-train (Volume 2) GRAFTING and BUDDING. (Volume 2)groot marvelNo ratings yet
- HTN Keith RN Mike Kelly Case Study AnswersDocument13 pagesHTN Keith RN Mike Kelly Case Study AnswersabbieNo ratings yet
- Kami Export - Circulatory System Study Questions WorksheetDocument2 pagesKami Export - Circulatory System Study Questions WorksheetEshrat TushyNo ratings yet
- GMT Assessment Adult CPR Skills DescriptionDocument2 pagesGMT Assessment Adult CPR Skills DescriptionpfeNo ratings yet
- Guideline: Physical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureDocument30 pagesGuideline: Physical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureNindy Yantika MciNo ratings yet
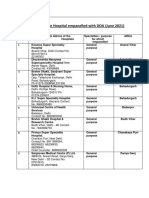
- List of The Hospital Empanelled With DDA (June 2021)Document24 pagesList of The Hospital Empanelled With DDA (June 2021)ygkrchNo ratings yet
- TEE Surgical Decision Making - June2020 PDFDocument43 pagesTEE Surgical Decision Making - June2020 PDFalina100% (1)
- Case PresentationDocument16 pagesCase PresentationAnuja NairNo ratings yet
- Ujang RDocument20 pagesUjang Rrode sihombingNo ratings yet
- First Grading VIDocument82 pagesFirst Grading VIIvy Villanueva Divino100% (1)
- MRD Carotid StentDocument5 pagesMRD Carotid StentKhushboo WarhadeNo ratings yet
- Atwood Management of Acute Coronary Syndrome 2022Document14 pagesAtwood Management of Acute Coronary Syndrome 2022goten ramirezNo ratings yet
- Basic ECG InterpretationDocument62 pagesBasic ECG Interpretationmohannadalkwiese3No ratings yet
- Biology 11 - Cardiovascular System True/False Intro Activity (With Answers)Document2 pagesBiology 11 - Cardiovascular System True/False Intro Activity (With Answers)ascd_msvuNo ratings yet
- Iso 5910 2018Document15 pagesIso 5910 2018Vũ QuangNo ratings yet
- PNS MethoxamineDocument1 pagePNS MethoxamineKim RuizNo ratings yet
- Hypertension GuidelinesDocument33 pagesHypertension GuidelinesErlinda NRANo ratings yet
- Physio Initial Assessment Form: Glasgow Coma ScaleDocument1 pagePhysio Initial Assessment Form: Glasgow Coma Scalechetha kundiNo ratings yet
- Management Acute StrokeDocument108 pagesManagement Acute StrokeratuhamimNo ratings yet
- 06 - HSE Alert Emergency Response - Electrical IncidentDocument2 pages06 - HSE Alert Emergency Response - Electrical Incidentmohammad_shahzad_iiuiNo ratings yet
- SBARDocument1 pageSBARCindy Deeann StarkeyNo ratings yet
- 5 ECG Changes of Hyperkalemia You Need To Know: 1. Tall 'Tented' T WavesDocument4 pages5 ECG Changes of Hyperkalemia You Need To Know: 1. Tall 'Tented' T Wavesricky hutagalungNo ratings yet
- CSA-AKI PatophysiologyDocument15 pagesCSA-AKI PatophysiologyOğuz KayıkçıNo ratings yet
- Atrioventricular Spetal Defect Avsd Partial EditDocument2 pagesAtrioventricular Spetal Defect Avsd Partial EditFelicia Shan SugataNo ratings yet
- Assignment Module 6Document2 pagesAssignment Module 6CARL JAMESNo ratings yet
- On CPRDocument32 pagesOn CPRPiyush Dutta100% (1)
- Diastolic Heart Failure Diagnosis and Therapy.12Document7 pagesDiastolic Heart Failure Diagnosis and Therapy.12enriquegarciagalianaNo ratings yet
- Excessive Weight Lifting PDFDocument6 pagesExcessive Weight Lifting PDFDownTheTheRabbitHole108No ratings yet
- Rheumatic Heart DiseaseDocument7 pagesRheumatic Heart DiseaseRoel John Atamosa CasilacNo ratings yet
- Diabetes, The Metabolic Syndrome, and Ischemic Stroke: Epidemiology and Possible MechanismsDocument10 pagesDiabetes, The Metabolic Syndrome, and Ischemic Stroke: Epidemiology and Possible MechanismsFelia AlyciaNo ratings yet
- Principles in Writing A ParagraphDocument6 pagesPrinciples in Writing A Paragraphjannah playlistsNo ratings yet