You might also like
- CHN WR1Document31 pagesCHN WR1IlawNo ratings yet
- Global Health Issues PPDocument91 pagesGlobal Health Issues PPRitaNo ratings yet
- Community Health Nursing 1 Public Health Nursing in The PhilippinesDocument16 pagesCommunity Health Nursing 1 Public Health Nursing in The PhilippinesFlourence ZafranNo ratings yet
- Community Health Nursing OverviewDocument7 pagesCommunity Health Nursing OverviewKatie HolmesNo ratings yet
- NCM 113 Final Module 8 LectureDocument8 pagesNCM 113 Final Module 8 LectureAngel Khrisna BacasmotNo ratings yet
- CHN211 Week 1 WORD - Overview of Public Health Nursing in The PhilippinesDocument19 pagesCHN211 Week 1 WORD - Overview of Public Health Nursing in The PhilippinesVenansius GanggusNo ratings yet
- Community Health Nursing ReviewerDocument28 pagesCommunity Health Nursing ReviewerJenie Munar RosarioNo ratings yet
- CHN 1 Topic 1. A Handout in Overview of Public Health Nursing in The Phils.Document11 pagesCHN 1 Topic 1. A Handout in Overview of Public Health Nursing in The Phils.DANIAH ASARI. SAWADJAANNo ratings yet
- Community Health Nursing I Meeting AgendaDocument57 pagesCommunity Health Nursing I Meeting Agendasecret laNo ratings yet
- At The End of The Lesson, The Students Will:: Overview of Public Health Nursing in The Philippines Learning OutcomesDocument18 pagesAt The End of The Lesson, The Students Will:: Overview of Public Health Nursing in The Philippines Learning OutcomesPABLO, JACKSON P.100% (1)
- CHN 1 FullDocument88 pagesCHN 1 FullKristine Joy CamusNo ratings yet
- MidtermDocument60 pagesMidterm3D - AURELIO, Lyca Mae M.0% (1)
- Day 1aDocument67 pagesDay 1aMinette BucioNo ratings yet
- Global Health Challenges ClassDocument29 pagesGlobal Health Challenges ClassLenard GpNo ratings yet
- Western Mindanao State University Public Health Nursing Handout Overview Philippines IssuesDocument16 pagesWestern Mindanao State University Public Health Nursing Handout Overview Philippines IssuesRoshin TejeroNo ratings yet
- Health Problems in IndiaDocument25 pagesHealth Problems in Indiashubham rathod100% (1)
- Global Health Issues, Challenges and Trends The Importance of Global HealthDocument10 pagesGlobal Health Issues, Challenges and Trends The Importance of Global HealthIan James P. BranganNo ratings yet
- Bangladesh National Conservation StrategyDocument22 pagesBangladesh National Conservation StrategySaeed ShawonNo ratings yet
- Global Health Care Challenges and TrendsDocument13 pagesGlobal Health Care Challenges and TrendsNADISH MANZOORNo ratings yet
- What Is Global Health and Why Is It ImportantDocument7 pagesWhat Is Global Health and Why Is It ImportantSanty ManuelNo ratings yet
- Global Health Issues-2019Document8 pagesGlobal Health Issues-2019vishwanathNo ratings yet
- GlobalHealthBriefingBook FINAL Web PDFDocument66 pagesGlobalHealthBriefingBook FINAL Web PDFAyoade opeyemiNo ratings yet
- Global and National Health Situation Global Health Situation and Trends 1955-2025 PopulationDocument5 pagesGlobal and National Health Situation Global Health Situation and Trends 1955-2025 PopulationFatima Rewafa AminullaNo ratings yet
- Overview of Public Health 1Document65 pagesOverview of Public Health 1Ellyza EvangelistaNo ratings yet
- Sustainable development goals: Goal 3; Good health and well-beingDocument5 pagesSustainable development goals: Goal 3; Good health and well-beingMuhammad Haseeb HassanNo ratings yet
- Group 10 Global HealthDocument12 pagesGroup 10 Global HealthPearl Alex CandoNo ratings yet
- What Is Public HealthDocument13 pagesWhat Is Public HealthHpg HsuNo ratings yet
- CHN 1 Module 1Document9 pagesCHN 1 Module 1kcamillebautistaNo ratings yet
- Critical Period of Adolescence and Importance of Investment in Youth HealthDocument3 pagesCritical Period of Adolescence and Importance of Investment in Youth HealthMUWANGUZI ALEXANDERNo ratings yet
- Health Grade 10 Quarter 3 ReviewerDocument8 pagesHealth Grade 10 Quarter 3 ReviewerAntonNo ratings yet
- Global Health Priorities and ProgramsDocument22 pagesGlobal Health Priorities and ProgramsNalu ChangNo ratings yet
- Public Health Theme: Introduction To Public Health: DR Elizabeth OrtonDocument38 pagesPublic Health Theme: Introduction To Public Health: DR Elizabeth OrtonSidiq AboobakerNo ratings yet
- Clinical Nutrition Education of Doctors and MedicalDocument6 pagesClinical Nutrition Education of Doctors and Medicalpure 97jkNo ratings yet
- Future of Health Psych: Ageing, Gender, SystemsDocument15 pagesFuture of Health Psych: Ageing, Gender, SystemsnoorNo ratings yet
- Community Health Nursing NCM 104 2nd WeekDocument10 pagesCommunity Health Nursing NCM 104 2nd WeekGlyza EbradaNo ratings yet
- Global Health and Nursing Group 2Document16 pagesGlobal Health and Nursing Group 2Kathleen Camile CenaNo ratings yet
- Health Care in Developing Countries: Challenges and OpportunitiesDocument40 pagesHealth Care in Developing Countries: Challenges and OpportunitiesMainak MukherjeeNo ratings yet
- Community Health Nursing LectureDocument62 pagesCommunity Health Nursing LectureJoana Grace CortezNo ratings yet
- 14367SDG3format-rev MD ODDocument10 pages14367SDG3format-rev MD ODmert05No ratings yet
- 3 Global health lesson 1Document21 pages3 Global health lesson 1Solomon Fallah Foa SandyNo ratings yet
- Community Health Nursing LectureDocument35 pagesCommunity Health Nursing LectureMaxeneDhaleNo ratings yet
- Health and DevelopmentDocument20 pagesHealth and DevelopmentZinhle MthembuNo ratings yet
- Food Safety W07Document7 pagesFood Safety W07MelanieNo ratings yet
- Double Burden of Disease ReportDocument48 pagesDouble Burden of Disease ReportAlmasNo ratings yet
- CHN Modules No 3 4 PDFDocument262 pagesCHN Modules No 3 4 PDFMichael OblegoNo ratings yet
- 1234 Global health lesson 1 (1) -Document27 pages1234 Global health lesson 1 (1) -Solomon Fallah Foa SandyNo ratings yet
- Hunt JurnalDocument29 pagesHunt JurnalLily NGNo ratings yet
- World Health OrganizationDocument4 pagesWorld Health OrganizationLoreth Aurea OjastroNo ratings yet
- Strengthening The Quality Agenda in Health Care in Low-And Middle-Income Countries: Questions To ConsiderDocument5 pagesStrengthening The Quality Agenda in Health Care in Low-And Middle-Income Countries: Questions To ConsiderJose RamirezNo ratings yet
- Overview of Public Health Nursing in The Philippines: Learning ObjectivesDocument15 pagesOverview of Public Health Nursing in The Philippines: Learning ObjectivesRainy DaysNo ratings yet
- Contribution of Community Health Workers in The PRDocument31 pagesContribution of Community Health Workers in The PRVia Eliadora TogatoropNo ratings yet
- IBDP Geography complete summaryDocument8 pagesIBDP Geography complete summaryMeliNo ratings yet
- Ii. Problems and Development Strategies: Problems of The Third World CountriesDocument21 pagesIi. Problems and Development Strategies: Problems of The Third World CountriesMicsjadeCastilloNo ratings yet
- CHN Lecture - The Health Care Delivery SystemDocument38 pagesCHN Lecture - The Health Care Delivery SystemKatrina EstoconingNo ratings yet
- GLOBALDocument10 pagesGLOBALTiffany AdriasNo ratings yet
- Global Health Then and NowDocument4 pagesGlobal Health Then and NownameNo ratings yet
- The Philippine Health Agenda 2016 To 2022Document11 pagesThe Philippine Health Agenda 2016 To 2022Sheryl Alapad100% (3)
- 2nd Script For ScriptwritingDocument9 pages2nd Script For ScriptwritingFawzan Fahad MDNo ratings yet
- Philippine Nutrition Plan Targets Reducing Stunting, WastingDocument7 pagesPhilippine Nutrition Plan Targets Reducing Stunting, WastingJerreca DasasNo ratings yet
- Barangay Council Organization ChartDocument1 pageBarangay Council Organization ChartJerreca DasasNo ratings yet
- Control of Microbial GrowthDocument4 pagesControl of Microbial GrowthJerreca DasasNo ratings yet
- Adult Mouth Assessment FormDocument1 pageAdult Mouth Assessment FormJerreca DasasNo ratings yet
- 0.3 Chapter 3 - The FamilyDocument4 pages0.3 Chapter 3 - The FamilyJerreca DasasNo ratings yet
- 0.2 Chapter 2 - The Health Care Delivery SystemDocument20 pages0.2 Chapter 2 - The Health Care Delivery SystemJerreca DasasNo ratings yet
- S + LV + CDocument1 pageS + LV + CJerreca DasasNo ratings yet
- 12 Tenses of Verbs Explained in DetailDocument31 pages12 Tenses of Verbs Explained in DetailJerreca DasasNo ratings yet
- BSN1 F - Eng100 Group2Document31 pagesBSN1 F - Eng100 Group2Jerreca DasasNo ratings yet
- ExamplesDocument1 pageExamplesJerreca DasasNo ratings yet
- 12 Tenses of The VerbDocument3 pages12 Tenses of The VerbJerreca DasasNo ratings yet
- 3.5 PHARMA ANTI MYCOBACTERIAL AGENTSpdfDocument18 pages3.5 PHARMA ANTI MYCOBACTERIAL AGENTSpdfJanet SantosNo ratings yet
- Pedia Prof - OamilDocument147 pagesPedia Prof - OamilOne Click Online ShopNo ratings yet
- Med-Surg Exam #2 Study GuideDocument33 pagesMed-Surg Exam #2 Study GuideCaitlyn BilbaoNo ratings yet
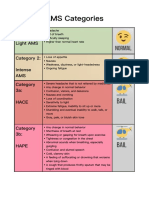
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- Book Reviews SampleDocument14 pagesBook Reviews SampleJohn Rey JumauayNo ratings yet
- African Traditional Medicine's Contributions to Nigeria's HealthcareDocument12 pagesAfrican Traditional Medicine's Contributions to Nigeria's HealthcareAliNo ratings yet
- Head Circumference For Age ChartDocument1 pageHead Circumference For Age ChartKaran TripathiNo ratings yet
- A008 MicroVue C4d EnglishDocument15 pagesA008 MicroVue C4d EnglishAlisNo ratings yet
- Early-Onset Sepsis in Newborns 2023Document9 pagesEarly-Onset Sepsis in Newborns 2023Charlie CharcapeNo ratings yet
- Tumor Inhibitors in PlantDocument14 pagesTumor Inhibitors in PlantTayf AlrawINo ratings yet
- MCQ Exam Questions (Faculty Pediatrics 2019-2020) .: Choleretics and Cholekinetics / HolenzimDocument20 pagesMCQ Exam Questions (Faculty Pediatrics 2019-2020) .: Choleretics and Cholekinetics / HolenzimKumar AdityaNo ratings yet
- Corn Pest Surveillance Pre-Inception MeetingDocument41 pagesCorn Pest Surveillance Pre-Inception MeetingMarcJunardJoverNo ratings yet
- Chapter 3 - The Polygraph TechniqueDocument16 pagesChapter 3 - The Polygraph Techniqueキャロル アンNo ratings yet
- Ecc Class 68 Pediatric (Newborn) Part - 4Document44 pagesEcc Class 68 Pediatric (Newborn) Part - 4Dinabandhu BaradNo ratings yet
- TB Management Final1Document23 pagesTB Management Final1Aanchal JainNo ratings yet
- Cell Injury, Cell Death, and Adaptations: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocument27 pagesCell Injury, Cell Death, and Adaptations: Dr. I Made Naris Pujawan, M.Biomed, SP - PAlindaNo ratings yet
- CBCR Joint Pain Student VersionDocument4 pagesCBCR Joint Pain Student VersionNika GianashviliNo ratings yet
- Biliran Province State University: ISO 9001:2015 CERTIFIED School of Nursing and Health SciencesDocument9 pagesBiliran Province State University: ISO 9001:2015 CERTIFIED School of Nursing and Health SciencesMaia Saivi OmegaNo ratings yet
- Magsaysay Memorial College of Zambales, IncDocument4 pagesMagsaysay Memorial College of Zambales, IncJoanne CuestaNo ratings yet
- Medical-Surgical Nursing Exam 20: NLE Style (100 Items) : Answers & RationaleDocument15 pagesMedical-Surgical Nursing Exam 20: NLE Style (100 Items) : Answers & RationaleHasan A AsFourNo ratings yet
- ACEs FlyerDocument2 pagesACEs Flyermahima sajanNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Epistaksis Pada Polip Nasal: September 2022Document10 pagesEpistaksis Pada Polip Nasal: September 2022FitrianiNo ratings yet
- Chapter 29: Perinatal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument2 pagesChapter 29: Perinatal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Chanca Piedra - Various Properties (Potential) PDFDocument17 pagesChanca Piedra - Various Properties (Potential) PDFSurya WijayaNo ratings yet
- Joseph Murphy Book ReviewsDocument54 pagesJoseph Murphy Book ReviewsDr. Peter Fritz Walter100% (4)
- GCSE History Britain: Health and The People, C1000-Present DayDocument30 pagesGCSE History Britain: Health and The People, C1000-Present DayAniqah ShujaatNo ratings yet
- Rufus Giwa Polytechnic OwoDocument7 pagesRufus Giwa Polytechnic OwoOLATIGBE NASIFNo ratings yet
- Final Oxygen Therapy and Monitoring Devices FM CommentedDocument56 pagesFinal Oxygen Therapy and Monitoring Devices FM CommentedDesalegnNo ratings yet
- Detection of Cardiac Disorder Using MATLAB BasedDocument4 pagesDetection of Cardiac Disorder Using MATLAB BasedSeira LoyardNo ratings yet