You might also like
- Volume Replacement Therapy - Principles and Clinical UseFrom EverandVolume Replacement Therapy - Principles and Clinical UseNo ratings yet
- RRT: Citrate & Acid Base Balance: Carole Ichai, MD, PHD Medicosurgical IcuDocument17 pagesRRT: Citrate & Acid Base Balance: Carole Ichai, MD, PHD Medicosurgical IcuОльга РапицкаяNo ratings yet
- Proceso Oxo (Hidroformilación) : Andrea Dávila AlvarezDocument22 pagesProceso Oxo (Hidroformilación) : Andrea Dávila AlvarezkrmeliNo ratings yet
- Analisis Sintesis I: Sintesis Vitamin Dan Beberapa AntibiotikDocument12 pagesAnalisis Sintesis I: Sintesis Vitamin Dan Beberapa AntibiotikNovita Sari AritonangNo ratings yet
- MEKANISMEDocument2 pagesMEKANISMEEry NourikaNo ratings yet
- Diels-Alder Practice Problems With AnswersDocument2 pagesDiels-Alder Practice Problems With AnswersBoas Wayne100% (1)
- Doc-20170131-Wa0159 1 1Document9 pagesDoc-20170131-Wa0159 1 1rashidNo ratings yet
- Citric Acid Cycle: Step 1 Step 2 Step 8Document3 pagesCitric Acid Cycle: Step 1 Step 2 Step 8Ali Ali AliNo ratings yet
- Name Reactions Knoevenagel AnswerDocument1 pageName Reactions Knoevenagel AnswerShally GuptaNo ratings yet
- Chemistry Xam IdeaDocument9 pagesChemistry Xam Ideagowrimanohar1975No ratings yet
- Lec 5 Aldehyde Ketone Nucleophilic Addition PDFDocument78 pagesLec 5 Aldehyde Ketone Nucleophilic Addition PDFAssyakurNo ratings yet
- Mekanisme RX DibenzalasetonDocument2 pagesMekanisme RX DibenzalasetonWulan safitriNo ratings yet
- Synthesis of Salicylic Acid: Practical Lab. 3Document12 pagesSynthesis of Salicylic Acid: Practical Lab. 3Saba GheniNo ratings yet
- Synthesis of Aspirin and Wintegreen Spring 2006Document6 pagesSynthesis of Aspirin and Wintegreen Spring 2006apzzzzNo ratings yet
- Preparation of MaleimideDocument11 pagesPreparation of MaleimideDotsha Raheem100% (1)
- Organic Name Reactions: Nutshell Review & Preview ofDocument9 pagesOrganic Name Reactions: Nutshell Review & Preview ofSai YashwanthNo ratings yet
- Nanh (1 Equiv.) 2. CH - CH - I H, Lindlar Catalyst Mcpba CH Li Cubr TSCL Pyridine NacnDocument12 pagesNanh (1 Equiv.) 2. CH - CH - I H, Lindlar Catalyst Mcpba CH Li Cubr TSCL Pyridine NacnpNo ratings yet
- Tarea x3Document1 pageTarea x3Ulises DantánNo ratings yet
- Problem Set 4 - Key: 1. Suggest A Plausible Arrow-Pushing Mechanism For The Following Reactions. ADocument6 pagesProblem Set 4 - Key: 1. Suggest A Plausible Arrow-Pushing Mechanism For The Following Reactions. ATrần Nguyễn Quỳnh NhưNo ratings yet
- Moleculas 3Document3 pagesMoleculas 3Eloy Morales perezNo ratings yet
- IMP Last Minute Revision Formulae Organic ChemistryDocument99 pagesIMP Last Minute Revision Formulae Organic ChemistryMakeshsvm2611No ratings yet
- Dark Reaction Calvin Cycle C3, C4 and CAM Plants Photorespiration Factors Influencing PhotorespirationDocument44 pagesDark Reaction Calvin Cycle C3, C4 and CAM Plants Photorespiration Factors Influencing PhotorespirationprianthikaNo ratings yet
- Biodegradable Polymers: Chemistry, Degradation and ApplicationsDocument26 pagesBiodegradable Polymers: Chemistry, Degradation and ApplicationsAnand GuptaNo ratings yet
- ZaharideDocument7 pagesZaharideBriana IonescuNo ratings yet
- Biodegradable Materials 1Document26 pagesBiodegradable Materials 1Louie Shaolin LungaoNo ratings yet
- Question 5C (I) Reagents - Lewis Acid (Alcl3) - Acetyl Chloride (CH Cocl)Document9 pagesQuestion 5C (I) Reagents - Lewis Acid (Alcl3) - Acetyl Chloride (CH Cocl)KIBET SHADRACKNo ratings yet
- Esterfication MechanismDocument1 pageEsterfication MechanismrasikamuhandiramgeNo ratings yet
- Molecular Mechanisms of Enzyme Action: (WEEK 7)Document44 pagesMolecular Mechanisms of Enzyme Action: (WEEK 7)oczhinviaNo ratings yet
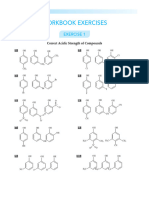
- Goc 1 Work Book 1Document12 pagesGoc 1 Work Book 1YuvarajNo ratings yet
- 4Document3 pages4vinhb2204329No ratings yet
- Advanced Biochemistry: The Krebs CycleDocument11 pagesAdvanced Biochemistry: The Krebs CycleMaritsa PerHerNo ratings yet
- 생체의학공학 04 BiomaterialsDocument124 pages생체의학공학 04 Biomaterials생따일괄기No ratings yet
- 1 GlikolisisDocument15 pages1 GlikolisisQonita FadiyahNo ratings yet
- Requirements For Structural Determination of A Carbohydrate A B CDocument20 pagesRequirements For Structural Determination of A Carbohydrate A B CMunir AhmadNo ratings yet
- Carboxylic Acid Derivatives: 1. The Correct Explanation For The Below Reaction IsDocument20 pagesCarboxylic Acid Derivatives: 1. The Correct Explanation For The Below Reaction Issree anugraphicsNo ratings yet
- Reaksi Aldehid Dan KetonDocument19 pagesReaksi Aldehid Dan KetonMega KurniaNo ratings yet
- Mecanismos de Sintesis de PolimerosDocument3 pagesMecanismos de Sintesis de PolimerosJesús Gildardo López BurgosNo ratings yet
- Monomers Oligomers Polymers MacromoleculesDocument6 pagesMonomers Oligomers Polymers MacromoleculesQuar Tul AinNo ratings yet
- Topic - Colloids SolutionDocument6 pagesTopic - Colloids SolutionMuhd AmirNo ratings yet
- Mechanisms 1-10: CHEM 725: Davey 1Document7 pagesMechanisms 1-10: CHEM 725: Davey 1Bradley DaveyNo ratings yet
- 1 An Observation - The Krebs CycleDocument33 pages1 An Observation - The Krebs CycleOmbrog JustinNo ratings yet
- Carboxylic Acid and Their DerivativesDocument5 pagesCarboxylic Acid and Their DerivativesShubham KumarNo ratings yet
- BI115 หลักชีววิทยา (Priciples of biology)Document315 pagesBI115 หลักชีววิทยา (Priciples of biology)สาธิต ปริ นทร์ทองNo ratings yet
- Mecanismo de Reaccion Cloretona o ClorobutanolDocument1 pageMecanismo de Reaccion Cloretona o ClorobutanolAndres MondragonNo ratings yet
- Glyc o SidesDocument22 pagesGlyc o Sidessiddra khalidNo ratings yet
- Alkene PreparationDocument1 pageAlkene Preparationtemp accNo ratings yet
- 4.5 Answers To ExercisesDocument4 pages4.5 Answers To Exercisesloly62006No ratings yet
- Biological Molecules - ProteinsDocument18 pagesBiological Molecules - ProteinsblackmoneygrabberNo ratings yet
- Heterocyclic ReactionsDocument2 pagesHeterocyclic Reactionsthat's niceNo ratings yet
- Amino Acids 21Document12 pagesAmino Acids 21Taha GHNo ratings yet
- Reductions PPT 29-08-2020Document12 pagesReductions PPT 29-08-2020jkc collegeNo ratings yet
- Ejercicios ElectroquimicaDocument6 pagesEjercicios ElectroquimicaEthel Elsa D ́ Arendelle Lan WanJi IPNNo ratings yet
- Esquema GlucolisisDocument2 pagesEsquema GlucolisisJulio César CastañedaNo ratings yet
- Kami Export - 6 Biological MoleculesDocument5 pagesKami Export - 6 Biological MoleculesNicholas Crowell100% (1)
- Quant Chem AnalDocument4 pagesQuant Chem AnalMisheelt TsolmonbaatarNo ratings yet
- MitDocument13 pagesMitKasi RuddrarajuNo ratings yet
- Advanced Organic Reactions 2000 - WarrenDocument174 pagesAdvanced Organic Reactions 2000 - Warrenshiv57100% (3)
- SelectivityDocument4 pagesSelectivitySamik BiswasNo ratings yet
- Solution Manual for The Elements of Polymer Science and EngineeringFrom EverandSolution Manual for The Elements of Polymer Science and EngineeringRating: 4 out of 5 stars4/5 (3)
- Twinmotion 2016 Edition Full CrackDocument3 pagesTwinmotion 2016 Edition Full CrackGivi Andriyanto0% (1)
- Dll-Eapp 12 Week 15Document5 pagesDll-Eapp 12 Week 15marivic franciscoNo ratings yet
- Design and Analysis Aircraft Nose and Nose Landing Gear PDFDocument8 pagesDesign and Analysis Aircraft Nose and Nose Landing Gear PDFTarik Hassan ElsonniNo ratings yet
- ACCSA Module 1 - 8 Practice Dimensions & Skillsets of Addiction CounsellingDocument148 pagesACCSA Module 1 - 8 Practice Dimensions & Skillsets of Addiction Counsellingskye42817No ratings yet
- QQQQ PDFDocument484 pagesQQQQ PDFSagor Saha100% (1)
- Chapter 2Document7 pagesChapter 2Edita O PanuncioNo ratings yet
- BOLBOK (1st)Document10 pagesBOLBOK (1st)Mj EndozoNo ratings yet
- Microtronics Technologies: GSM Based Vehicle Theft Detection SystemDocument3 pagesMicrotronics Technologies: GSM Based Vehicle Theft Detection Systemابراهيم الثوبريNo ratings yet
- Business Tax ReviewerDocument22 pagesBusiness Tax ReviewereysiNo ratings yet
- AX Performance Tools1Document21 pagesAX Performance Tools1Htun Lin AungNo ratings yet
- Leadership's Ramdom MCQsDocument48 pagesLeadership's Ramdom MCQsAhmed NoumanNo ratings yet
- Scheme and Syllabus of B.E. (Computer Science and Engineering) 3 TO8 Semester 2017-2018Document170 pagesScheme and Syllabus of B.E. (Computer Science and Engineering) 3 TO8 Semester 2017-2018pratik YadavNo ratings yet
- Somatic TherapiesDocument170 pagesSomatic TherapiesDelyn Gamutan Millan100% (2)
- Cutlist Cistern TankDocument10 pagesCutlist Cistern TankAilyn O. DungogNo ratings yet
- Online Banking TCsDocument52 pagesOnline Banking TCsmaverick_1901No ratings yet
- BCSP GuideDocument44 pagesBCSP GuideCarol Sarmiento DelgadoNo ratings yet
- Question Bank For MDocument22 pagesQuestion Bank For MchinnnababuNo ratings yet
- Psychology - Masters in Psychology Entrance Examination Book (Power Within Psychology, Amit Panwar) (Z-Library)Document414 pagesPsychology - Masters in Psychology Entrance Examination Book (Power Within Psychology, Amit Panwar) (Z-Library)Suraj100% (12)
- CN Mod1 Ppt-FinalDocument56 pagesCN Mod1 Ppt-FinalkkNo ratings yet
- Huawei Sne Mobile Phone User Guide - (Emui9.0.1 - 01, En-Uk, Normal)Document68 pagesHuawei Sne Mobile Phone User Guide - (Emui9.0.1 - 01, En-Uk, Normal)FarzadNo ratings yet
- MarpleDocument10 pagesMarpleC.Auguste DupinNo ratings yet
- Benjamin Gomez v. Enrico PalomarDocument11 pagesBenjamin Gomez v. Enrico PalomarUlyung DiamanteNo ratings yet
- Gamla Stan PDFDocument4 pagesGamla Stan PDFAlexandra FricosuNo ratings yet
- Reading 40 Introduction To Industry and Company AnalysisDocument23 pagesReading 40 Introduction To Industry and Company AnalysisNeerajNo ratings yet
- Bridge Operation Maintenance COWIDocument19 pagesBridge Operation Maintenance COWIAhmadKhattabNo ratings yet
- Chapter 11Document3 pagesChapter 11Kristine TiuNo ratings yet
- 2 - ARM Cotex-M3 - IntroductionDocument124 pages2 - ARM Cotex-M3 - IntroductionNghĩa VũNo ratings yet
- DBMS NotesDocument6 pagesDBMS Notesᴠɪᴄɪᴏᴜs ᴄᴜʀsᴇNo ratings yet
- PNAPDocument79 pagesPNAPYu chung yinNo ratings yet
- Coastal Boards Co Is A Merchandising Business The Account BalancesDocument1 pageCoastal Boards Co Is A Merchandising Business The Account BalancesFreelance WorkerNo ratings yet