You might also like
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Blood Pressure Regulation HandoutDocument10 pagesBlood Pressure Regulation Handoutsac50900100% (2)
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- CVS 5Document6 pagesCVS 5MayankNo ratings yet
- Blood Pressure-For StudentsDocument79 pagesBlood Pressure-For StudentsAshok Kumar P100% (1)
- Cardio-Physiology Exam QuestionsDocument17 pagesCardio-Physiology Exam Questionsjimmy100% (1)
- 2300 - Module 5 - Basic Cardiovascular PathophysiologyDocument14 pages2300 - Module 5 - Basic Cardiovascular Pathophysiologymegan.abbinkNo ratings yet
- Cardiovasular SystemDocument26 pagesCardiovasular SystemPhai KoemhienNo ratings yet
- Blood Pressure AssignmentDocument19 pagesBlood Pressure AssignmentADITYAROOP PATHAKNo ratings yet
- Manajemen Disritmia Kardiak IntraoperatifDocument53 pagesManajemen Disritmia Kardiak IntraoperatifAbi FaizNo ratings yet
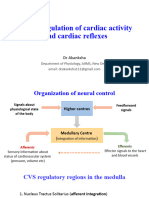
- Lecture 8 - Neural Regulation of Cardiac Activity and Cardiac ReflexesDocument35 pagesLecture 8 - Neural Regulation of Cardiac Activity and Cardiac ReflexesVishal BalamuruganNo ratings yet
- Approach To ShockDocument28 pagesApproach To ShockSyasya ZulkiffliNo ratings yet
- Lung InflammationDocument44 pagesLung InflammationOnSolomonNo ratings yet
- Diagnosis&Manajemen ShockDocument8 pagesDiagnosis&Manajemen ShockHJKIMNo ratings yet
- Nervous Regulation of The Circulation and Rapid Control of Arterial PressureDocument2 pagesNervous Regulation of The Circulation and Rapid Control of Arterial Pressuremcwnotes100% (2)
- Heart Rate Blood PressureDocument128 pagesHeart Rate Blood PressureShubhra ShettyNo ratings yet
- Circulation Seqs With Keys Edu Apnafort ComDocument10 pagesCirculation Seqs With Keys Edu Apnafort ComᎷᏒ ᏗᏒᎩᏗᏁ ᏦᏂᏗᏁNo ratings yet
- Drugs Acting in CVSDocument63 pagesDrugs Acting in CVSMeghan Norico Cristuta100% (1)
- 05 Cardiovascular System PhysiologyDocument34 pages05 Cardiovascular System PhysiologyKaye Alyssa EnriquezNo ratings yet
- MS Cardio Lecture EDITEDDDocument28 pagesMS Cardio Lecture EDITEDDsanchezanya34No ratings yet
- Cardiovascular Control: Marinette Rumusud-Jambaro, MD Diplomate in Internal MedicineDocument48 pagesCardiovascular Control: Marinette Rumusud-Jambaro, MD Diplomate in Internal MedicineVerlette Roselle Aguisanda LizardoNo ratings yet
- Goal of The Cardiovascular System: Deliver Blood To All Parts of The BodyDocument20 pagesGoal of The Cardiovascular System: Deliver Blood To All Parts of The BodyNestor BalboaNo ratings yet
- Blood Pressure PhysiologyDocument167 pagesBlood Pressure PhysiologyMeriam AntonyNo ratings yet
- Long & Short Term Regulation of BPDocument50 pagesLong & Short Term Regulation of BPntambik21No ratings yet
- Blood PressureDocument26 pagesBlood PressureEniola DaramolaNo ratings yet
- 8 BloodpressuremechanismDocument75 pages8 BloodpressuremechanismNithya SekarNo ratings yet
- Antiarrhythmic DrugsDocument15 pagesAntiarrhythmic DrugsjaimeNo ratings yet
- Cardiovascular SystemDocument8 pagesCardiovascular SystemDawnmurph Dharlene Wag-eNo ratings yet
- 25circulation Part 3Document15 pages25circulation Part 3Jaydave PatelNo ratings yet
- Physiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Document62 pagesPhysiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Akshay ChaudharyNo ratings yet
- Control of Blood Pressure: OutlineDocument26 pagesControl of Blood Pressure: OutlineNurul Avisa ArianiNo ratings yet
- Cardiovascular System TamreedDocument8 pagesCardiovascular System TamreedslmylwkaaNo ratings yet
- CV RegulatnDocument28 pagesCV RegulatnShahin KhanNo ratings yet
- BP503T Unit 1-3Document432 pagesBP503T Unit 1-3Solomon GyampohNo ratings yet
- Cardiovascular Regulatory MechanismDocument34 pagesCardiovascular Regulatory Mechanismhia natasyaNo ratings yet
- Cardiac Arrest Cardiac Massage Defibrillation: Pathophysiological BasisDocument42 pagesCardiac Arrest Cardiac Massage Defibrillation: Pathophysiological Basisronwest1990No ratings yet
- Short and Long Term Regulation and Determinants of BPDocument90 pagesShort and Long Term Regulation and Determinants of BPDan Tristam MicabaloNo ratings yet
- Arterial Pressure RegulationDocument50 pagesArterial Pressure RegulationareebNo ratings yet
- Cardiac Cycle NotesDocument20 pagesCardiac Cycle NotesKelly Yeow100% (3)
- Homeostasis Sistem Kardiovaskuler: Dr. Dr. H. Busjra M. Nur MSC Dept. Fisiologi Fkui / FKK UmjDocument22 pagesHomeostasis Sistem Kardiovaskuler: Dr. Dr. H. Busjra M. Nur MSC Dept. Fisiologi Fkui / FKK Umjtaufiqus stengahTKSNo ratings yet
- MODULE 20 HANDOUTS Cardiovascular SystemDocument4 pagesMODULE 20 HANDOUTS Cardiovascular SystemMichaela PoNo ratings yet
- Regulation of ECF VolumeDocument49 pagesRegulation of ECF VolumeGeorge LusanaNo ratings yet
- Autonomic Dysfunction and Hypotension: Christopher J. MathiasDocument28 pagesAutonomic Dysfunction and Hypotension: Christopher J. MathiaswaltercarvalhoNo ratings yet
- Physio Lab Rev 2Document48 pagesPhysio Lab Rev 2Kyle IcaroNo ratings yet
- Physiology Summary Chapter 20Document9 pagesPhysiology Summary Chapter 20gail01850% (2)
- Cardiac Output, Venous Return, and Their RegulationDocument50 pagesCardiac Output, Venous Return, and Their RegulationMohammed T. Abdul Razak100% (1)
- Heart Failure - 2022Document106 pagesHeart Failure - 2022Rana Khaled AwwadNo ratings yet
- JVP, Hs&coDocument29 pagesJVP, Hs&coVansh SinghNo ratings yet
- 2.2 Strcuture and Function of Cardiovascular SystemDocument74 pages2.2 Strcuture and Function of Cardiovascular SystemchaaarrNo ratings yet
- 1324autonomicdysfunc 180617164555Document83 pages1324autonomicdysfunc 180617164555Minaz PatelNo ratings yet
- Blood Pressure Regulation - SlidesDocument35 pagesBlood Pressure Regulation - Slidesمحمد السنجلاويNo ratings yet
- BloodpressureDocument47 pagesBloodpressureakinaasirNo ratings yet
- Heart QuizDocument1 pageHeart QuizNaNo ratings yet
- CASE 1 TG Heart Failure and Cardiogenic Shock 2014Document52 pagesCASE 1 TG Heart Failure and Cardiogenic Shock 2014biandaNo ratings yet
- Cardiovascular System: Dulay, Arjay SDocument21 pagesCardiovascular System: Dulay, Arjay SarjayNo ratings yet
- Cardio Vascular SystemDocument62 pagesCardio Vascular SystemMeera NandanNo ratings yet
- Physiology of The HeartDocument34 pagesPhysiology of The Heartalyssa_marie_keNo ratings yet
- The Circulation: Blood Pressure RegulationDocument42 pagesThe Circulation: Blood Pressure RegulationLouis JinNo ratings yet
- Lab08 Frog HeartDocument4 pagesLab08 Frog HeartAbie CaponponNo ratings yet
- Wa0004.Document31 pagesWa0004.Aisha samreenNo ratings yet
- ProSim8 Umeng0300 User ManualDocument112 pagesProSim8 Umeng0300 User ManualMarco QuirozNo ratings yet
- (Thesis) Neide Simões 2013 PDFDocument164 pages(Thesis) Neide Simões 2013 PDFDmitriyNo ratings yet
- Acute Critical Care Nursing HandoutDocument17 pagesAcute Critical Care Nursing HandoutJulie May100% (6)
- ADHFDocument81 pagesADHFAfni WahyuniNo ratings yet
- Ecocardiografia NeonatalDocument10 pagesEcocardiografia NeonatalRonald MHNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSherree Hayes100% (2)
- Principle of Aerobic ExercisesDocument46 pagesPrinciple of Aerobic Exercisesway to satlok100% (1)
- Coherencia HemodinamicaDocument9 pagesCoherencia HemodinamicaMaritza Alejandra Baeza EricesNo ratings yet
- Articulo Shock Neurogenic o 2016Document5 pagesArticulo Shock Neurogenic o 2016Christian MolinaNo ratings yet
- Unity User Manual PDFDocument226 pagesUnity User Manual PDFRizkiana SamarindNo ratings yet
- Recommendations For Standards of Monitoring During 2015Document10 pagesRecommendations For Standards of Monitoring During 2015Bondan PalestinNo ratings yet
- Medical Electronics 2 Marks With AnswersDocument17 pagesMedical Electronics 2 Marks With Answersyasmin niharaNo ratings yet
- Technological Assessment and Objective Evaluation of Minimally Invasive and Noninvasive Cardiac Output Monitoring SystemsDocument8 pagesTechnological Assessment and Objective Evaluation of Minimally Invasive and Noninvasive Cardiac Output Monitoring Systemsnvidia coreNo ratings yet
- Exercise HTP ArtDocument10 pagesExercise HTP ArtDiana CarstairsNo ratings yet
- Whole-Body Human Thermal Models: E. H. WisslerDocument50 pagesWhole-Body Human Thermal Models: E. H. WisslerArinjayKumarNo ratings yet
- HypertensionDocument2 pagesHypertensionRodel Yacas0% (1)
- 11 Care of The CV Surgery Patient EmilDocument2 pages11 Care of The CV Surgery Patient EmilameliajamirusNo ratings yet
- OXY-Cardio Care ManagementDocument114 pagesOXY-Cardio Care Managementlalaine22daleNo ratings yet
- Case Study Scenario # 1 Congestive Heart Failure (Mojica)Document10 pagesCase Study Scenario # 1 Congestive Heart Failure (Mojica)Noah Kent MojicaNo ratings yet
- Fluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CADocument9 pagesFluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CAerwanNo ratings yet
- Measurements To Guide Your Patient Care: EfficiaDocument16 pagesMeasurements To Guide Your Patient Care: EfficiaXinwen ChenNo ratings yet
- Perfusion and HemodynamicsDocument21 pagesPerfusion and HemodynamicsKrisianne Mae Lorenzo Francisco100% (1)
- Guidelines For Intensive Care Unit DesignDocument11 pagesGuidelines For Intensive Care Unit DesignasupicuNo ratings yet
- Bio Unit 4Document38 pagesBio Unit 4Mei NgNo ratings yet
- General Surgery MCQDocument249 pagesGeneral Surgery MCQShriyansh Chahar88% (8)
- Intraoperative Management of Shock in Adults - UpToDateDocument36 pagesIntraoperative Management of Shock in Adults - UpToDateYessica RivasNo ratings yet
- Hemodynamic MonitoringDocument28 pagesHemodynamic MonitoringKimberlie Dela Merced Tomas100% (1)
- 2003-Academic Emergency MedicineDocument154 pages2003-Academic Emergency MedicinealiceNo ratings yet
- Updated - Prioritization of ProblemsDocument1 pageUpdated - Prioritization of ProblemsKaycelyn JimenezNo ratings yet
- Moxy Running EbookDocument18 pagesMoxy Running EbookPippo PlutoNo ratings yet
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayFrom EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNo ratings yet
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionFrom EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionRating: 3.5 out of 5 stars3.5/5 (11)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (784)
- Music For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicFrom EverandMusic For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicRating: 5 out of 5 stars5/5 (1)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (96)
- Whole Body Barefoot: Transitioning Well to Minimal FootwearFrom EverandWhole Body Barefoot: Transitioning Well to Minimal FootwearRating: 4 out of 5 stars4/5 (16)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (111)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Weight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantFrom EverandWeight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantRating: 4.5 out of 5 stars4.5/5 (38)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.From EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Rating: 4.5 out of 5 stars4.5/5 (124)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesFrom EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo ratings yet
- Structural Integration and Energy Medicine: A Handbook of Advanced BodyworkFrom EverandStructural Integration and Energy Medicine: A Handbook of Advanced BodyworkRating: 4 out of 5 stars4/5 (1)
- The Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandThe Yamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (19)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceFrom EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceRating: 4.5 out of 5 stars4.5/5 (237)
- Fascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)From EverandFascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)Rating: 5 out of 5 stars5/5 (3)
- The Power of Now by Eckhart Tolle: Summary and AnalysisFrom EverandThe Power of Now by Eckhart Tolle: Summary and AnalysisRating: 4.5 out of 5 stars4.5/5 (12)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingFrom EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingRating: 4.5 out of 5 stars4.5/5 (132)
- Body by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekRating: 4 out of 5 stars4/5 (38)
- If You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsFrom EverandIf You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsRating: 4.5 out of 5 stars4.5/5 (7)
- Buteyko Breathing Course Manual: For use with the Advanced Buteyko CourseFrom EverandButeyko Breathing Course Manual: For use with the Advanced Buteyko CourseRating: 5 out of 5 stars5/5 (1)