You might also like
- Interpretation of Arterial Blood Gases (ABGs)Document6 pagesInterpretation of Arterial Blood Gases (ABGs)afalfitraNo ratings yet
- Teaching Argument WritingDocument8 pagesTeaching Argument WritingAmanda Garcia0% (1)
- Marketing Plan SampleDocument100 pagesMarketing Plan SampleCamille See100% (17)
- Mirzhakhanyan v. Setyan, Motion To Set Aside DafaultDocument8 pagesMirzhakhanyan v. Setyan, Motion To Set Aside DafaultElena VernyNo ratings yet
- Acid Base AnswersDocument4 pagesAcid Base Answersapi-232466940No ratings yet
- Fluid Electrolyte ImbalanceDocument46 pagesFluid Electrolyte ImbalanceAxsa Alex100% (1)
- DiaQueen SUPER LONG LIFE COOLANT PREMIUM PDFDocument5 pagesDiaQueen SUPER LONG LIFE COOLANT PREMIUM PDFJohannes VGNo ratings yet
- 3rd Annual Innovation Coast Conference Detailed ScheduleDocument40 pages3rd Annual Innovation Coast Conference Detailed ScheduleOrganic Nuts100% (1)
- Acid Base DisordersDocument5 pagesAcid Base DisordersMillenial VoiceNo ratings yet
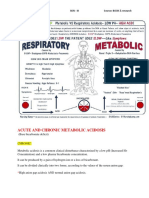
- Acute and Chronic Metabolic Acidosis: Amada, Kevin Moor N. BSN - Iii Source: BOOK & ResearchDocument10 pagesAcute and Chronic Metabolic Acidosis: Amada, Kevin Moor N. BSN - Iii Source: BOOK & ResearchKyle Ü D. CunanersNo ratings yet
- MedicineDocument30 pagesMedicineDr .Boobalan VengateshNo ratings yet
- RTA Type 1 TreatmentDocument4 pagesRTA Type 1 TreatmentJane RamosNo ratings yet
- Hepatopulmonary SyndromeDocument1 pageHepatopulmonary SyndromepraveenbhavniNo ratings yet
- De Morais, HA, Et Al, Fluid, Electrolyte, Acid Base Disorders, 2012, 302-315Document14 pagesDe Morais, HA, Et Al, Fluid, Electrolyte, Acid Base Disorders, 2012, 302-315Yanie Ummu ArsylaNo ratings yet
- TERBARU Dr. RUDY TERAPI OKSIGENDocument55 pagesTERBARU Dr. RUDY TERAPI OKSIGENDhytha NovitaNo ratings yet
- Jurding Hipertensi PulmonalDocument33 pagesJurding Hipertensi PulmonalRyu KangNo ratings yet
- Acid-Base Disorder in SurgeryDocument52 pagesAcid-Base Disorder in SurgeryFree ZingNo ratings yet
- PNUR 251 Homeostasis S 2022Document56 pagesPNUR 251 Homeostasis S 2022JennNo ratings yet
- Shock Five Point ZeroDocument78 pagesShock Five Point ZeroprashsubbuNo ratings yet
- Guidebook: Department of AnaesthesiaDocument9 pagesGuidebook: Department of Anaesthesiasmoore1234No ratings yet
- Respiratory Failure Workup: Approach ConsiderationsDocument8 pagesRespiratory Failure Workup: Approach Considerationsjeanie mae PangapalanNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument15 pagesDr. Ali's Uworld Notes For Step 2 CKBoogy WoogyNo ratings yet
- Tau Chempath - Acid Base Imbalance & Pahology of Resp FailureDocument31 pagesTau Chempath - Acid Base Imbalance & Pahology of Resp FailureChipego ChiyaamaNo ratings yet
- Interpretation of Arterial Blood Gases (Abgs) I David A. Kaufman, MD DDocument17 pagesInterpretation of Arterial Blood Gases (Abgs) I David A. Kaufman, MD DingridpuspitaNo ratings yet
- Veterinary Clinics: Respiratory Acidosis: A Quick ReferenceDocument4 pagesVeterinary Clinics: Respiratory Acidosis: A Quick ReferenceAndersonValentimOliveiradaSilvaNo ratings yet
- Acid - Base Imbalance and Its Impact On ElectrolytesDocument40 pagesAcid - Base Imbalance and Its Impact On ElectrolytesahmadNo ratings yet
- Blood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIDocument39 pagesBlood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIIQBAL HAKKIKINo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Book Review (Writing) : Indriyani (1740601042)Document8 pagesBook Review (Writing) : Indriyani (1740601042)Indri YaniNo ratings yet
- Pneumonia - Kyphoscoliosis - Morbid Obesity - Drug OverdoseDocument3 pagesPneumonia - Kyphoscoliosis - Morbid Obesity - Drug OverdoseJessica nonyeNo ratings yet
- Interpretation of Arterial Blood GasesDocument7 pagesInterpretation of Arterial Blood GasesGaby FernándezNo ratings yet
- Arterial Blood GasDocument65 pagesArterial Blood GasKar TwentyfiveNo ratings yet
- Chloremia (Hypochloremia) & Acute and Chronic Respiratory Alkalosis (Carbonic Acid Deficit)Document4 pagesChloremia (Hypochloremia) & Acute and Chronic Respiratory Alkalosis (Carbonic Acid Deficit)KQarlo Luis Pestaño Maniaol100% (1)
- Acute Pulmonary Edema: Purwoko Sugeng HDocument25 pagesAcute Pulmonary Edema: Purwoko Sugeng HBee DanielNo ratings yet
- High Yield ItemsDocument790 pagesHigh Yield ItemsErin HillNo ratings yet
- Acid Base: Heather Wacholz TCCCDocument33 pagesAcid Base: Heather Wacholz TCCCahmadNo ratings yet
- AJAB CAR Pulmonary HypertensionDocument51 pagesAJAB CAR Pulmonary HypertensionAjabsingh ChoudharyNo ratings yet
- Disturbances in AcidDocument11 pagesDisturbances in AcidShannen Alija M. LaoNo ratings yet
- ABG Interpretation 1Document59 pagesABG Interpretation 1Sura KwakNo ratings yet
- Fluid, Electrolytes, Acid Base BalanceDocument18 pagesFluid, Electrolytes, Acid Base Balanceashdmb217100% (5)
- BiochemistryDocument33 pagesBiochemistryamhhospital0No ratings yet
- Understanding Acid Base Balance.3Document3 pagesUnderstanding Acid Base Balance.3YuniParaditaDjunaidi100% (1)
- Medical Surgical Nursing TionkoDocument40 pagesMedical Surgical Nursing TionkojeshemaNo ratings yet
- Abg 2Document6 pagesAbg 2Maine AsuncionNo ratings yet
- ContDocument76 pagesContIola JaneNo ratings yet
- Arterial Blood Gas InterpretationsDocument7 pagesArterial Blood Gas InterpretationsErin TraversNo ratings yet
- 04 06 0413 PDFDocument10 pages04 06 0413 PDFeric lauwrenzNo ratings yet
- Alterations in Gas Exchange NEW SU 2023 STUDENTDocument83 pagesAlterations in Gas Exchange NEW SU 2023 STUDENTHaley HannNo ratings yet
- Arterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPDocument39 pagesArterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPGio Tamaño BalisiNo ratings yet
- Arterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPDocument39 pagesArterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPevbptrprnrmNo ratings yet
- Normal Anion GapDocument5 pagesNormal Anion Gapatribecalledquest20No ratings yet
- Fluid Electrolyte ImbalanceDocument46 pagesFluid Electrolyte ImbalanceAxsa AlexNo ratings yet
- Acid-Base Homeostasis: Dr. Abeer KhurshidDocument42 pagesAcid-Base Homeostasis: Dr. Abeer Khurshidسلة فواكة100% (2)
- Tuti Herawati, MN: Fakultas Ilmu Keperawatan Universitas Indonesia 2008Document40 pagesTuti Herawati, MN: Fakultas Ilmu Keperawatan Universitas Indonesia 2008SelvyaNo ratings yet
- Drug-Induced Lupus Pleuritis Mimicking Pleural Space LnfectionDocument2 pagesDrug-Induced Lupus Pleuritis Mimicking Pleural Space LnfectionAtmayadi GunawanNo ratings yet
- ABG Interpretation - ATSDocument5 pagesABG Interpretation - ATSHAMMYER ALROKHAMINo ratings yet
- Resp AlkalosisDocument4 pagesResp AlkalosisCas SanchezNo ratings yet
- Fluid Electrolye Acid Base Disorder EraldDocument21 pagesFluid Electrolye Acid Base Disorder EraldM. R. EmeraldNo ratings yet
- Acid Base Balance and DisordersDocument25 pagesAcid Base Balance and DisordersIsmail Vokshi100% (1)
- Hypo Xi ADocument22 pagesHypo Xi AIka RivaniNo ratings yet
- Alert Medical Series: USMLE Alert I, II, IIIFrom EverandAlert Medical Series: USMLE Alert I, II, IIIRating: 2 out of 5 stars2/5 (1)
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansFrom EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpNo ratings yet
- Dna Structure: A, B and Z Dna Helix Families Dnastructure: Sequence EffectsDocument11 pagesDna Structure: A, B and Z Dna Helix Families Dnastructure: Sequence EffectsAdriana MorenoNo ratings yet
- Assignment Chapter 9Document3 pagesAssignment Chapter 9Nur ArinahNo ratings yet
- Security Analysis (Mauboussin) SP2015Document12 pagesSecurity Analysis (Mauboussin) SP2015Glaiza OrtigueroNo ratings yet
- 2022-MRV South & Southeast Asia-Edit (High Res.)Document124 pages2022-MRV South & Southeast Asia-Edit (High Res.)tsaifulNo ratings yet
- FullStack LabDocument44 pagesFullStack LabRam DhighashNo ratings yet
- Wedding LutopanDocument2 pagesWedding LutopanCecelia ChoirNo ratings yet
- Project Report On Worker Turnover On KDS GarmentsDocument18 pagesProject Report On Worker Turnover On KDS GarmentsShelveyElmoDiasNo ratings yet
- 2014 - The Episteme Journal of Linguistics and Literature Vol 1 No 1 - 2-The Analysis of Language Style On The Campaign Speech ofDocument9 pages2014 - The Episteme Journal of Linguistics and Literature Vol 1 No 1 - 2-The Analysis of Language Style On The Campaign Speech ofwahyuningsi fahrahNo ratings yet
- FS 1 Episode 1 FinalDocument25 pagesFS 1 Episode 1 FinalJonny VirayNo ratings yet
- Bassoon Quartets and Quintets Sheet Music Collection DVDDocument3 pagesBassoon Quartets and Quintets Sheet Music Collection DVDdigitalsheetplusNo ratings yet
- Homework Slang WordDocument8 pagesHomework Slang Wordafetuieog100% (1)
- Y%S, XLD M Dka %SL Iudcjd Ckrcfha .Eiü M %H: The Gazette of The Democratic Socialist Republic of Sri LankaDocument13 pagesY%S, XLD M Dka %SL Iudcjd Ckrcfha .Eiü M %H: The Gazette of The Democratic Socialist Republic of Sri LankaYoonus MaheesNo ratings yet
- Megatech, Inc. Case Study 1: John Locke - SM 300 - Chapter 1 ActivityDocument2 pagesMegatech, Inc. Case Study 1: John Locke - SM 300 - Chapter 1 ActivityRené Ríos100% (1)
- Chapter 1 PhoneticsDocument9 pagesChapter 1 PhoneticsAthaya FirdaNo ratings yet
- P1-3 and P1-9 Sanga's PartDocument22 pagesP1-3 and P1-9 Sanga's PartAmir AmirrzzNo ratings yet
- GSM Mobile Based Speed Control of DC MotorDocument9 pagesGSM Mobile Based Speed Control of DC MotorRoshan Singh100% (1)
- Benefits of RuckingDocument1 pageBenefits of RuckingFerdous ShareefNo ratings yet
- Syntagmatic RelationsDocument11 pagesSyntagmatic RelationsSarwar AzizNo ratings yet
- "Mental Fitness For Traders" by Norman HalletDocument35 pages"Mental Fitness For Traders" by Norman Halletapi-26247058100% (2)
- Ezekiel, The Prophet of The ExileDocument10 pagesEzekiel, The Prophet of The ExileSung RemiNo ratings yet
- A Letter of Hazrat Abul Hasanat Abdullah Shah HYDERABADDocument12 pagesA Letter of Hazrat Abul Hasanat Abdullah Shah HYDERABADMohammed Abdul Hafeez, B.Com., Hyderabad, IndiaNo ratings yet
- Iceberg Model of CultureDocument4 pagesIceberg Model of CultureafiqahNo ratings yet
- Zoroastrian Is MDocument401 pagesZoroastrian Is Mkrataios100% (4)
- IITB Transportation PlanningDocument24 pagesIITB Transportation PlanningsohamNo ratings yet
- 16s - Wiring Diagram - Package Insert v16.1Document2 pages16s - Wiring Diagram - Package Insert v16.1Harold MontesNo ratings yet