You might also like
- Integration and Visualization of Gene Selection and Gene Regulatory Networks for Cancer GenomeFrom EverandIntegration and Visualization of Gene Selection and Gene Regulatory Networks for Cancer GenomeNo ratings yet
- Machine Learning Methods For Estimating Heterogeneous Causal EffectsDocument25 pagesMachine Learning Methods For Estimating Heterogeneous Causal EffectsLilia XaNo ratings yet
- Machine Learning Methods For Estimating HeterogeneDocument26 pagesMachine Learning Methods For Estimating HeterogeneRBNo ratings yet
- Nciph ERIC14Document5 pagesNciph ERIC14bejarhasanNo ratings yet
- Assessing Bias The Importance of Considering ConfoundingDocument4 pagesAssessing Bias The Importance of Considering ConfoundingAndrieli TodescatoNo ratings yet
- BiasDocument1 pageBiasAbdulqader DawoudNo ratings yet
- Quantitative Reasearch KINDS OF RESEARCHDocument1 pageQuantitative Reasearch KINDS OF RESEARCHEivie SonioNo ratings yet
- 1408 BiasDocument3 pages1408 Biaspeppino WuverNo ratings yet
- Chen 2007Document42 pagesChen 2007Jonathan MansillaNo ratings yet
- Kinds of Quantitative ResearchDocument5 pagesKinds of Quantitative ResearchArlene Lie FernandoNo ratings yet
- LESSON 1 - Nature of Inquiry and Research PDFDocument36 pagesLESSON 1 - Nature of Inquiry and Research PDFKent SalmorinNo ratings yet
- Handouts 1Document4 pagesHandouts 1Ken DumpNo ratings yet
- Bioe 211 - Epidemiologic StudiesDocument5 pagesBioe 211 - Epidemiologic Studiesbabalegaspi09No ratings yet
- Molin 4Document7 pagesMolin 4Yor - ChannelNo ratings yet
- Module 1 Prac 2 Month of SeptemberDocument22 pagesModule 1 Prac 2 Month of SeptemberLeah CalzadoNo ratings yet
- Word VisualDocument146 pagesWord VisualRenan MagpusaoNo ratings yet
- Unveiling The Hidden Connections Exploring Correlation AnalysisDocument8 pagesUnveiling The Hidden Connections Exploring Correlation Analysisk.i.n.g.ston.dra.ke.31No ratings yet
- Artículo Saccharomyces CerevisaeDocument9 pagesArtículo Saccharomyces CerevisaeJessi BoschNo ratings yet
- Multilevel Modeling of Individual and Group Level Mediated EffectsDocument31 pagesMultilevel Modeling of Individual and Group Level Mediated EffectsPhuoc NguyenNo ratings yet
- Biostatistics For CK Step 2 6.16.2019Document37 pagesBiostatistics For CK Step 2 6.16.2019karan kauraNo ratings yet
- Analysis of Cause Effect RelationshipDocument50 pagesAnalysis of Cause Effect RelationshipRida AwwalNo ratings yet
- Hennekens 0316356360 Pp287-323 Copyright ClearedDocument20 pagesHennekens 0316356360 Pp287-323 Copyright ClearedMareesol Chan-TiopiancoNo ratings yet
- Researchmethodslecture 2015Document25 pagesResearchmethodslecture 2015api-300762638No ratings yet
- 2018 Mansournia Case ControlDocument23 pages2018 Mansournia Case ControlmateusglehnNo ratings yet
- Expounding The Terms in ResearchDocument49 pagesExpounding The Terms in ResearchElon MuskNo ratings yet
- Multivariate Behavioral Research: To Cite This Article: Stanley A. Mulaik (1987) : A Brief History of The PhilosophicalDocument40 pagesMultivariate Behavioral Research: To Cite This Article: Stanley A. Mulaik (1987) : A Brief History of The PhilosophicalAcatalepsoNo ratings yet
- Nested Case Control StudyDocument6 pagesNested Case Control StudyFarah FarahNo ratings yet
- BIAS. Confounding and Effect ModificationDocument10 pagesBIAS. Confounding and Effect ModificationCSilva16No ratings yet
- Epid Klinik 6 ValiduitasDocument71 pagesEpid Klinik 6 ValiduitasHalim SyahrilNo ratings yet
- Association Causation - DR FarzanaDocument41 pagesAssociation Causation - DR Farzanahimanshu2010swNo ratings yet
- Solution Manual For Introduction To Epidemiology Distribution and Determinants of Disease 1st EditionDocument9 pagesSolution Manual For Introduction To Epidemiology Distribution and Determinants of Disease 1st EditionCrystalGalvantebi100% (39)
- Lesson5 ExpsyDocument6 pagesLesson5 ExpsygacilanaltheabspsyNo ratings yet
- Appraising The Evidence: What Is Selection Bias?: Case Control StudiesDocument2 pagesAppraising The Evidence: What Is Selection Bias?: Case Control Studiesruba azfr-aliNo ratings yet
- Kind Goal Variables and Experimental Manipulation Data Collection Technique Sample TitlesDocument6 pagesKind Goal Variables and Experimental Manipulation Data Collection Technique Sample TitlesChristine EvangelistaNo ratings yet
- Correlational Research PPT Group 2Document15 pagesCorrelational Research PPT Group 2Lisma Firda FarhaniNo ratings yet
- Twin StudiesDocument5 pagesTwin StudiesKeenisha KannanNo ratings yet
- Public Health FADocument22 pagesPublic Health FAsaurabhdhakedgNo ratings yet
- A Meta-Analytic Examination of Attrition in Virtual Reality Exposure TherapyDocument9 pagesA Meta-Analytic Examination of Attrition in Virtual Reality Exposure TherapyArteria PsicosocialNo ratings yet
- Study Guide in Lesson 1: The Characteristics, Strengths, Weaknesses, and Kinds of Quantitative ResearchDocument3 pagesStudy Guide in Lesson 1: The Characteristics, Strengths, Weaknesses, and Kinds of Quantitative ResearchMia GallegoNo ratings yet
- Non-Gaussian Methods For Causal Structure Learning: Shohei ShimizuDocument11 pagesNon-Gaussian Methods For Causal Structure Learning: Shohei ShimizuEmotyNo ratings yet
- Module For The Month of SEPTEMBER Practical Research Ii Grade 12 First Semester S.Y. 2021-2022Document20 pagesModule For The Month of SEPTEMBER Practical Research Ii Grade 12 First Semester S.Y. 2021-2022Cute NickvanNo ratings yet
- Chapter 9 Validity in Epidemiologic Studies Booklet - Final 9may2021Document7 pagesChapter 9 Validity in Epidemiologic Studies Booklet - Final 9may2021Genevieve Magpayo NangitNo ratings yet
- Evid Sint Decis Making 3Document23 pagesEvid Sint Decis Making 3Antonio López MolláNo ratings yet
- 02 - Quantitative Research - HANDOUTSDocument2 pages02 - Quantitative Research - HANDOUTSJOSEPH EARNEST TIEMPONo ratings yet
- Delgado-Rodriguez 2004 SesgosDocument7 pagesDelgado-Rodriguez 2004 SesgosGaby SchwindtNo ratings yet
- Quantitative Research MethodologiesDocument35 pagesQuantitative Research MethodologiesRomina Lucena FajardoNo ratings yet
- 408 MidDocument7 pages408 Midshishirar.12No ratings yet
- Final Exam Study Sheet Chapter 8-12Document2 pagesFinal Exam Study Sheet Chapter 8-12gulzira3amirovnaNo ratings yet
- Threats To Research Bias and Error Confounding and InteractionDocument8 pagesThreats To Research Bias and Error Confounding and Interactionnajdah_220754970No ratings yet
- Analysis of Variance (Anova) Aliasing Confounding Alpha RiskDocument8 pagesAnalysis of Variance (Anova) Aliasing Confounding Alpha RiskDennis ChenNo ratings yet
- Random and Systemeatic ErrorsDocument62 pagesRandom and Systemeatic Errorssamuel zelaelmNo ratings yet
- Biostatistics Study Cheat SheetDocument1 pageBiostatistics Study Cheat Sheetab100% (1)
- Evaluation of Scientific Publications - Part 11 - Data Analysis of Epidemiological Studies PDFDocument6 pagesEvaluation of Scientific Publications - Part 11 - Data Analysis of Epidemiological Studies PDFPhoNo ratings yet
- Lecture 29Document5 pagesLecture 29hrishabh_agrawalNo ratings yet
- Bias GlossaryDocument7 pagesBias GlossaryArielle Joize IlanoNo ratings yet
- Peer Effects AngristDocument11 pagesPeer Effects AngristShadab AzeemNo ratings yet
- Assessing Bias in Case-Control Studies: Comments, Opinions, and ReviewsDocument5 pagesAssessing Bias in Case-Control Studies: Comments, Opinions, and ReviewsAmelia MarisaNo ratings yet
- IDC 213 06 Workshop 3 Critical Appraisal On Studies About HarmDocument5 pagesIDC 213 06 Workshop 3 Critical Appraisal On Studies About HarmFort SalvadorNo ratings yet
- 11 AssociationDocument25 pages11 Associationrjt7jzd265No ratings yet
- IOER Descriptive and Inferential Gonzales NepthalieDocument39 pagesIOER Descriptive and Inferential Gonzales NepthalieMITZHE GAE MAMINONo ratings yet
- Riph Reviewer FinalsDocument5 pagesRiph Reviewer Finalsbabalegaspi09No ratings yet
- Bioe 211 - Outbreak InvestigationDocument4 pagesBioe 211 - Outbreak Investigationbabalegaspi09No ratings yet
- Bioe 211 - Epidemiologic StudiesDocument5 pagesBioe 211 - Epidemiologic Studiesbabalegaspi09No ratings yet
- Bioe 211 - Screening and Public Health SurveillanceDocument3 pagesBioe 211 - Screening and Public Health Surveillancebabalegaspi09No ratings yet
- Pdpa CraDocument3 pagesPdpa CraAdyrah RahmanNo ratings yet
- Fashion Design and Product DevelopmentDocument6 pagesFashion Design and Product DevelopmentYona Tasya AzizieNo ratings yet
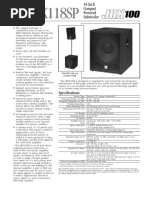
- JRX118SP SpecsheetDocument2 pagesJRX118SP SpecsheetLuisNo ratings yet
- Comparing Registers: MIPS vs. ARM AssemblyDocument12 pagesComparing Registers: MIPS vs. ARM Assemblyshruti chouhanNo ratings yet
- Student Teacher InterviewDocument3 pagesStudent Teacher InterviewLauren ColeNo ratings yet
- AirBossPSS100andEvoplusseriesscba Donning ProcedureDocument1 pageAirBossPSS100andEvoplusseriesscba Donning ProcedureMarco LondonNo ratings yet
- Painting and Weathering Unlocked PDFDocument91 pagesPainting and Weathering Unlocked PDFWrensEye100% (6)
- One Word SubstitutionDocument5 pagesOne Word SubstitutionPranaykant Singh PanwarNo ratings yet
- Intro To RMAN-10g-okDocument41 pagesIntro To RMAN-10g-okAnbao ChengNo ratings yet
- 027 03 Dec13 CseDocument647 pages027 03 Dec13 CseParth NagarNo ratings yet
- Assignment 1Document12 pagesAssignment 1Santosh SubramanyaNo ratings yet
- Cultural Competence Refers To An Ability To Interact Effectively With People of Different CulturesDocument5 pagesCultural Competence Refers To An Ability To Interact Effectively With People of Different CulturesKim EliotNo ratings yet
- FINAL THESIS DOC LastDocument114 pagesFINAL THESIS DOC LastMulat ShierawNo ratings yet
- CertificateofAnalysis 2019 11 9 879766Document2 pagesCertificateofAnalysis 2019 11 9 879766Trọng TínNo ratings yet
- De Cuong On Thi HK2 Tieng Anh 10Document5 pagesDe Cuong On Thi HK2 Tieng Anh 10hoangtouri2512No ratings yet
- English Is The Window To The World. MimieDocument2 pagesEnglish Is The Window To The World. MimieFARAH NADIANo ratings yet
- Complete-Crp SPC Shamli r01-1562323540Document291 pagesComplete-Crp SPC Shamli r01-1562323540p nandyNo ratings yet
- Swot Analysis of Revlon IncDocument5 pagesSwot Analysis of Revlon IncSubhana AsimNo ratings yet
- APAVE Tiger CP - UK - FINAL2Document1 pageAPAVE Tiger CP - UK - FINAL2AdrewhassTechnicaNo ratings yet
- 4363 112 Heat TransferDocument6 pages4363 112 Heat Transferyogesh_b_kNo ratings yet
- TSS Training Package Implementation Guidefinal 0Document18 pagesTSS Training Package Implementation Guidefinal 0hanabbecharaNo ratings yet
- Virtual Screening of Natural Products DatabaseDocument71 pagesVirtual Screening of Natural Products DatabaseBarbara Arevalo Ramos100% (1)
- CATEGORY - Green (III) Consent To EstablishDocument4 pagesCATEGORY - Green (III) Consent To EstablishROOPDIP MUKHOPADHYAYNo ratings yet
- Activity On The Layers of The Earth 1Document1 pageActivity On The Layers of The Earth 1Ian MarianoNo ratings yet
- Binary Arithmetic Operations: Prof. R.Ezhilarasie Assistant Professor School of Computing SASTRA Deemed To Be UniversityDocument26 pagesBinary Arithmetic Operations: Prof. R.Ezhilarasie Assistant Professor School of Computing SASTRA Deemed To Be UniversityEzhil RamanathanNo ratings yet
- Climate Transition Finance Handbook Related Questions: 9 December 2020Document4 pagesClimate Transition Finance Handbook Related Questions: 9 December 2020glenlcyNo ratings yet
- IB Biology Lab Report TemplateDocument6 pagesIB Biology Lab Report TemplatebigbuddhazNo ratings yet
- Marc ChagallDocument3 pagesMarc ChagallAnaNo ratings yet
- SSPC Monitoreo y Control de Condiciones AmbientalesDocument4 pagesSSPC Monitoreo y Control de Condiciones AmbientalesRony Ruiz100% (1)
- Pre-Test Chapter 19 Ed17Document8 pagesPre-Test Chapter 19 Ed17Sarah ZeidatNo ratings yet