You might also like
- 2020 05 25 20110239v1 FullDocument7 pages2020 05 25 20110239v1 FullArief LiemNo ratings yet
- Povidone-Iodine Use in Sinonasal and Oral CavitiesDocument8 pagesPovidone-Iodine Use in Sinonasal and Oral CavitiesTulio Reis HannasNo ratings yet
- SSRN Id3563092Document10 pagesSSRN Id356309211050027No ratings yet
- The Use of Povidone Iodine Nasal Spray and Mouthwash During The Current COVID-19 Pandemic May Reduce Cross Infection and Protect Healthcare WorkersDocument10 pagesThe Use of Povidone Iodine Nasal Spray and Mouthwash During The Current COVID-19 Pandemic May Reduce Cross Infection and Protect Healthcare WorkersDwi RetnoNo ratings yet
- Repurposing 0.5% Povidone Iodine Solution in Otorhinolaryngology Practice in Covid 19 PandemicDocument4 pagesRepurposing 0.5% Povidone Iodine Solution in Otorhinolaryngology Practice in Covid 19 PandemicNeel PatelNo ratings yet
- Betadine Ear/nose Drops and Mouth Gargle Reduces Covid-19 Hospitalizations by 84%, Mortality by 88%.Document5 pagesBetadine Ear/nose Drops and Mouth Gargle Reduces Covid-19 Hospitalizations by 84%, Mortality by 88%.Michael Smith100% (1)
- Sjournal Homepage: - : Manuscript HistoryDocument5 pagesSjournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- SSRN Id3563092 PDFDocument10 pagesSSRN Id3563092 PDFAmalia SholihahNo ratings yet
- Beneficial Effects of A Mouthwash Containing An Antiviral Phthalocyanine Derivative On The Length of Hospital Stay For COVID 19: Randomised TrialDocument10 pagesBeneficial Effects of A Mouthwash Containing An Antiviral Phthalocyanine Derivative On The Length of Hospital Stay For COVID 19: Randomised TrialtvinteNo ratings yet
- Journal Pre-Proof: HeliyonDocument23 pagesJournal Pre-Proof: HeliyonMohammed Shuaib AhmedNo ratings yet
- Povidone-Iodine Gargle/Mouthwash Against Respiratory and Oral Tract PathogensDocument11 pagesPovidone-Iodine Gargle/Mouthwash Against Respiratory and Oral Tract PathogensJonathan00711No ratings yet
- Molecular Oral Microbiology - 2023 - D Amico - Efficacy of Cetylpyridinium Chloride Mouthwash Against SARS CoV 2 ADocument10 pagesMolecular Oral Microbiology - 2023 - D Amico - Efficacy of Cetylpyridinium Chloride Mouthwash Against SARS CoV 2 Akatcharles.persoNo ratings yet
- Study of The Efficacy and Safety of Topical Ivermectin + Iota-Carrageenan in The Prophylaxis Against COVID-19 in Health PersonnelDocument6 pagesStudy of The Efficacy and Safety of Topical Ivermectin + Iota-Carrageenan in The Prophylaxis Against COVID-19 in Health PersonnelKaroline MarxNo ratings yet
- Pathogens: Differential Effects of Antiseptic Mouth Rinses On Sars-Cov-2 Infectivity in VitroDocument14 pagesPathogens: Differential Effects of Antiseptic Mouth Rinses On Sars-Cov-2 Infectivity in VitroVINKA ANJANI IRNANDANo ratings yet
- Tolerability and Usability of 0.5% PVP-I Gargles and Nasal Drops in 6692 Patients: Observational StudyDocument4 pagesTolerability and Usability of 0.5% PVP-I Gargles and Nasal Drops in 6692 Patients: Observational StudyNeel PatelNo ratings yet
- Efficacy of Povidone-Iodine Nasal and Oral Antiseptic Preparations Against Severe Acute Respiratory Syndrome-Coronavirus 2 (Sars-Cov-2)Document5 pagesEfficacy of Povidone-Iodine Nasal and Oral Antiseptic Preparations Against Severe Acute Respiratory Syndrome-Coronavirus 2 (Sars-Cov-2)GTNo ratings yet
- 0.5% Povidone Iodine Irrigation in Otorhinolaryngology Surgical Practice During COVID 19 T PandemicDocument2 pages0.5% Povidone Iodine Irrigation in Otorhinolaryngology Surgical Practice During COVID 19 T PandemicNeel PatelNo ratings yet
- Avhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Document6 pagesAvhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Phuong ThaoNo ratings yet
- Cetylpyridinium Chloride As A Tool Against COVID-19Document4 pagesCetylpyridinium Chloride As A Tool Against COVID-19Nicoll SQNo ratings yet
- Public Health: Letter To The EditorDocument2 pagesPublic Health: Letter To The EditorFebie DevinaNo ratings yet
- Jam 13361Document6 pagesJam 13361Melissa SchulthessNo ratings yet
- Lary 9999 0Document8 pagesLary 9999 0Niken KuncorowatiNo ratings yet
- Sodio OralDocument6 pagesSodio OralBoris QuelcaNo ratings yet
- Being A Dentist in The PandemicDocument2 pagesBeing A Dentist in The PandemicLarissa CostaNo ratings yet
- Journal of Periodontology - 2021 - Anand - A Case Control Study On The Association Between Periodontitis and CoronavirusDocument7 pagesJournal of Periodontology - 2021 - Anand - A Case Control Study On The Association Between Periodontitis and CoronavirusGabriela VillagomezNo ratings yet
- Jurnal PerodonsiaDocument7 pagesJurnal PerodonsiaLisa Noor SetyaningrumNo ratings yet
- 1 s2.0 S0895398819301096 MainDocument10 pages1 s2.0 S0895398819301096 MainGabriela VargasNo ratings yet
- Dental Practitioners' Knowledge, Attitude and Practices For Mouthwash Use Amidst The COVID-19 PandemicDocument14 pagesDental Practitioners' Knowledge, Attitude and Practices For Mouthwash Use Amidst The COVID-19 PandemicsovalaxNo ratings yet
- Articulo 1 MicroDocument5 pagesArticulo 1 MicroSusanaNo ratings yet
- Vacuum Aerosol 6Document7 pagesVacuum Aerosol 6khamilatusyNo ratings yet
- MainDocument7 pagesMainlps DiamondNo ratings yet
- Clorhexidin Efektif Menurunkan VAPDocument7 pagesClorhexidin Efektif Menurunkan VAPNovi LisnawatiNo ratings yet
- 10 1016@j Oraloncology 2020 104821Document4 pages10 1016@j Oraloncology 2020 104821khamilatusyNo ratings yet
- Emergency Management in A Dental Clinic During TheDocument8 pagesEmergency Management in A Dental Clinic During TheAriska AndriyaniNo ratings yet
- Disinfection Methods Against SARS-CoV-2Document35 pagesDisinfection Methods Against SARS-CoV-2GTNo ratings yet
- DownloadDocument4 pagesDownloadSkAliHassanNo ratings yet
- Acetic Acid Disinfection As A Potential Adjunctive Therapy For Non Severe COVID 19Document4 pagesAcetic Acid Disinfection As A Potential Adjunctive Therapy For Non Severe COVID 19Intan AyuNo ratings yet
- Wuhan UniversityDocument10 pagesWuhan UniversityPavithra balasubramaniNo ratings yet
- 1-2021 HJ, ANTONIO, GIULIO, MANUEL Healthcare-10-00063Document10 pages1-2021 HJ, ANTONIO, GIULIO, MANUEL Healthcare-10-00063Palomar Dental GroupNo ratings yet
- Disinfection Methods Against Sars-Cov-2: A Systematic ReviewDocument34 pagesDisinfection Methods Against Sars-Cov-2: A Systematic ReviewFlori TabacaruNo ratings yet
- Polymicrobial Ventilator-Associated Pneumonia: Fighting in Vitro Candida albicans-Antifungal-Antibacterial Combination TherapyDocument19 pagesPolymicrobial Ventilator-Associated Pneumonia: Fighting in Vitro Candida albicans-Antifungal-Antibacterial Combination TherapyFarhanNo ratings yet
- Vol09 2 84-88strDocument5 pagesVol09 2 84-88strJoe Sam AbrahamNo ratings yet
- Testori Tiziano (2020), COVID-19 and Oral Surgery: A Narrative Review of Preoperative Mouth RinsesDocument11 pagesTestori Tiziano (2020), COVID-19 and Oral Surgery: A Narrative Review of Preoperative Mouth RinsesPhuong ThaoNo ratings yet
- Andrade Et Al-2020-Journal of Health & Biological SciencesDocument9 pagesAndrade Et Al-2020-Journal of Health & Biological SciencesJuliaNo ratings yet
- Infectious DiseasesDocument7 pagesInfectious DiseasesIneke FaradilaNo ratings yet
- Jurnal BerbayarDocument13 pagesJurnal BerbayarLIZBETH FEMMIL SAPUTRINo ratings yet
- Lingual Bony ProminencesDocument9 pagesLingual Bony ProminencesAgustin BiagiNo ratings yet
- Diagnosis and Protection of COVID-19 in StomatologyDocument5 pagesDiagnosis and Protection of COVID-19 in StomatologyBOHR International Journal of Current research in Dentistry (BIJCRID)No ratings yet
- Nasal Irrigation Clo2Document4 pagesNasal Irrigation Clo2Candela VidalNo ratings yet
- Sauer Brei 2010Document6 pagesSauer Brei 2010Antimikrop MikrobiyolojiNo ratings yet
- Hypochlorous Acid COVID ReviewDocument6 pagesHypochlorous Acid COVID ReviewEnvirolyte Solutions InternationalNo ratings yet
- Is The Oral Cavity Relevant in Sars-Cov-2 Pandemic?Document6 pagesIs The Oral Cavity Relevant in Sars-Cov-2 Pandemic?cabarcaxNo ratings yet
- SB 210547-553Document7 pagesSB 210547-553paria motahariNo ratings yet
- Synergistic Effects of Anionic Surfactants On Coronavirus (Sars-Cov-2) Virucidal Efficiency of Sanitizing Fluids To Fight Covid-19Document8 pagesSynergistic Effects of Anionic Surfactants On Coronavirus (Sars-Cov-2) Virucidal Efficiency of Sanitizing Fluids To Fight Covid-19Alicia PerezNo ratings yet
- Virucidal Eficacia de Enjuagatorios Orales COMPLETO JOURNALDocument4 pagesVirucidal Eficacia de Enjuagatorios Orales COMPLETO JOURNALDallas Juan Tarco SumireNo ratings yet
- Ellepola Microbiology PublicationDocument8 pagesEllepola Microbiology Publicationarjuna.ellepolaNo ratings yet
- Antiviral Activity of Reagents in Mouth Rinses Against Sars-Cov-2Document9 pagesAntiviral Activity of Reagents in Mouth Rinses Against Sars-Cov-2angie catalina estupiñan mirandaNo ratings yet
- Effects of Preprocedural Mouth Rinse On Microbial.12Document7 pagesEffects of Preprocedural Mouth Rinse On Microbial.12samanvi badriNo ratings yet
- Environmental Mycology in Public Health: Fungi and Mycotoxins Risk Assessment and ManagementFrom EverandEnvironmental Mycology in Public Health: Fungi and Mycotoxins Risk Assessment and ManagementCarla ViegasRating: 5 out of 5 stars5/5 (6)
- Cardiovascular Exam: FACEM Part II Notes Eunicia TanDocument28 pagesCardiovascular Exam: FACEM Part II Notes Eunicia TanGolam SarwarNo ratings yet
- Midterm PrepDocument2 pagesMidterm PrepSAKHAWAT HOSSAIN KHAN MDNo ratings yet
- Aspects of The Topic ReadingsDocument4 pagesAspects of The Topic ReadingsBettNo ratings yet
- P.B. TELEFO, Ph.D. Senior Lecturer of Biochemistry University of Dschang, CameroonDocument59 pagesP.B. TELEFO, Ph.D. Senior Lecturer of Biochemistry University of Dschang, CameroonTabe AndersonNo ratings yet
- Communicable Disease Surveillance in Animal PopulationDocument15 pagesCommunicable Disease Surveillance in Animal Populationsamwel danielNo ratings yet
- Lumber PDFDocument13 pagesLumber PDFPrasann RoyNo ratings yet
- Methicillin-Resistant Staphylococcus Aureus (MRSA)Document14 pagesMethicillin-Resistant Staphylococcus Aureus (MRSA)GIST (Gujarat Institute of Science & Technology)100% (1)
- PATH All TA Reviews Answers and Notes11Document718 pagesPATH All TA Reviews Answers and Notes11Andleeb Imran100% (1)
- Feline PanleukopeniaDocument15 pagesFeline PanleukopeniaVetlife DvpNo ratings yet
- Seizure Disorders: Assessment and Diagnostic FindingsDocument3 pagesSeizure Disorders: Assessment and Diagnostic FindingsBlessed GarcianoNo ratings yet
- Piis0300957220301428 PDFDocument5 pagesPiis0300957220301428 PDFDabeet MoncayoNo ratings yet
- Microbiology of WaterDocument27 pagesMicrobiology of WaterRao Qaisar Shahzad100% (2)
- A Review Article of Oral Health and Diabetes Mellitus: Ankita AgarwalDocument2 pagesA Review Article of Oral Health and Diabetes Mellitus: Ankita Agarwalankita agarwalNo ratings yet
- Position Statements of The PSAAI On COVID19 Vaccines and Their Adverse Reactions August 5 2021 ClickableDocument25 pagesPosition Statements of The PSAAI On COVID19 Vaccines and Their Adverse Reactions August 5 2021 ClickableMonica LowinskiNo ratings yet
- Case Study On Children With Cardiac DisordersDocument3 pagesCase Study On Children With Cardiac DisordersAlyNo ratings yet
- Chen. M SR and Three Level MADocument17 pagesChen. M SR and Three Level MASreeja CherukuruNo ratings yet
- TriageDocument6 pagesTriageWindyNo ratings yet
- I. Health, Wellness and Illness: Self-Esteem Love and Belongingness Self-ActualizationDocument3 pagesI. Health, Wellness and Illness: Self-Esteem Love and Belongingness Self-ActualizationYmon TuallaNo ratings yet
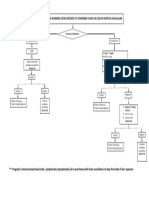
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- Final 22.06Document12 pagesFinal 22.06Anca NeaguNo ratings yet
- Asperger's Symptoms in Adults - Diagnosis, Treatment, and More - HOLLANDDocument11 pagesAsperger's Symptoms in Adults - Diagnosis, Treatment, and More - HOLLANDRoxan PacsayNo ratings yet
- Chapter 4 ParasitologyDocument35 pagesChapter 4 ParasitologyJuancho OsorioNo ratings yet
- September Recall ExportDocument1 pageSeptember Recall ExportMuhammad Abubakar100% (1)
- A Cardiomyopathy PPT NEWDocument62 pagesA Cardiomyopathy PPT NEWShetal Sharma100% (1)
- Certificates and FormatsDocument12 pagesCertificates and FormatsAnimesh PriyadarshiNo ratings yet
- Renal Tubulointerstitial DiseasesDocument13 pagesRenal Tubulointerstitial DiseasesDani DanyNo ratings yet
- Ankylosing SpondylitisDocument34 pagesAnkylosing SpondylitisLau100% (2)
- 20-21 - M - ENG - Part - 1 - PDFDocument34 pages20-21 - M - ENG - Part - 1 - PDFPulkit MittalNo ratings yet
- Jonelta Foundation School of Medicine: University of Perpetual Help System DaltaDocument5 pagesJonelta Foundation School of Medicine: University of Perpetual Help System DaltaMark Joshua CervantesNo ratings yet
- Guillain Barre Syndrome-PPT FinalDocument39 pagesGuillain Barre Syndrome-PPT Finalmeghana100% (1)