You might also like
- Acute Biologic Crisis & Disaster NursingDocument80 pagesAcute Biologic Crisis & Disaster NursingprinceBel21No ratings yet
- Disease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDocument57 pagesDisease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDeby Tri Widia LestariNo ratings yet
- Drugs Drugs Drugs STUDY GUIDEDocument13 pagesDrugs Drugs Drugs STUDY GUIDEAlexander Chamessian100% (1)
- Odynophagia Is Painful SwallowingDocument21 pagesOdynophagia Is Painful SwallowingVien CaagbayNo ratings yet
- NCP: Chronic Renal FailureDocument14 pagesNCP: Chronic Renal FailureJavie77% (13)
- Central DI in DogDocument70 pagesCentral DI in DogvetpathforumNo ratings yet
- Mnemonics For NursesDocument29 pagesMnemonics For Nursesashdmb217100% (2)
- Abg Concept: PH: 7.35-7.45 Paco2: 35-45 MMHG Hco3: 22-26 Meq/L Pao2: 80-100 MMHG Sao2: 95-100% Base Excess/ Deficit-2 - + 2Document7 pagesAbg Concept: PH: 7.35-7.45 Paco2: 35-45 MMHG Hco3: 22-26 Meq/L Pao2: 80-100 MMHG Sao2: 95-100% Base Excess/ Deficit-2 - + 2katherine dayagNo ratings yet
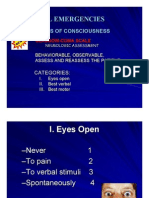
- Medical EmergenciesDocument81 pagesMedical EmergenciesKreshnik HAJDARINo ratings yet
- Pediatric NursingDocument14 pagesPediatric NursingJoanne PaulineNo ratings yet
- Clinical Methods General Exam 1Document57 pagesClinical Methods General Exam 1theonlinegeekhubNo ratings yet
- Common Histories and Red Flags Presentation Noninteractive VersionDocument21 pagesCommon Histories and Red Flags Presentation Noninteractive VersionesmarNo ratings yet
- General Medicine Diagnostic Points PDFDocument14 pagesGeneral Medicine Diagnostic Points PDF1031 Muhammad zaryabNo ratings yet
- Final ExamDocument8 pagesFinal ExamTaylor BurgessNo ratings yet
- Approach To Unconscious PatientDocument23 pagesApproach To Unconscious Patienttantw880% (1)
- Medical Nursing Notes on Stress Response and Endocrine DisordersDocument37 pagesMedical Nursing Notes on Stress Response and Endocrine Disordersincognito100% (11)
- Neurocardio NursingDocument101 pagesNeurocardio NursingMatt Lao DionelaNo ratings yet
- Mark Billy L. Perpetua, Man RN: Fluids, Electrolytes andDocument96 pagesMark Billy L. Perpetua, Man RN: Fluids, Electrolytes andMaica LectanaNo ratings yet
- Mnemonics For NursesDocument52 pagesMnemonics For Nursessweetpearl27100% (3)
- PropranololDocument2 pagesPropranololChristine Pialan SalimbagatNo ratings yet
- Case Presentation: Bernamieh O. Calam-Pastor, MDDocument51 pagesCase Presentation: Bernamieh O. Calam-Pastor, MDBernamai CalamNo ratings yet
- Heart Failure Symptoms and Physical FindingsDocument11 pagesHeart Failure Symptoms and Physical FindingsRubie Ann TillorNo ratings yet
- Exam 4 MedsurgDocument9 pagesExam 4 MedsurgTori RolandNo ratings yet
- Fe 2Document26 pagesFe 2api-3697326No ratings yet
- Syndrome of Inappropriate AdhDocument5 pagesSyndrome of Inappropriate AdhCarloRafaelNo ratings yet
- Pharmacology Guide for Safe Medication AdministrationDocument151 pagesPharmacology Guide for Safe Medication Administrationkyuss2100% (4)
- Fluids and Renal DisorderDocument139 pagesFluids and Renal DisorderLhara MañoNo ratings yet
- HyfrhDocument34 pagesHyfrhmebibegNo ratings yet
- Pedia - Intensive PhaseDocument2 pagesPedia - Intensive Phasepasabay270No ratings yet
- Fluids and Electrolytes, Acid-Base ImbalancesDocument15 pagesFluids and Electrolytes, Acid-Base ImbalancesJherome FernandoNo ratings yet
- DR Sonam's High Yield Notes For ST 2 & 5 2nd EditionDocument251 pagesDR Sonam's High Yield Notes For ST 2 & 5 2nd EditionMuhammad Fahad100% (1)
- Congenital Heart DefectsDocument3 pagesCongenital Heart DefectsAileen CaguladaNo ratings yet
- Theresa To PrintDocument6 pagesTheresa To PrintmtarriolaNo ratings yet
- Addison'sDocument4 pagesAddison'sKoRnflakesNo ratings yet
- Cardiac MedicationsDocument8 pagesCardiac Medicationsangeline totaram100% (2)
- MedSurg QuestionsDocument34 pagesMedSurg Questionssasha051969100% (1)
- Diana's Renal DiseasesDocument9 pagesDiana's Renal DiseasesdhyltonNo ratings yet
- Nursing Care Plan Renal FailureDocument11 pagesNursing Care Plan Renal Failurenosevad88850% (2)
- Medical MnemonicsDocument10 pagesMedical Mnemonicskenners99% (115)
- BCC - EndocrineDocument5 pagesBCC - EndocrineJhon meelerNo ratings yet
- Wk8 - Electrolyte Imbalances & Acid-Base ImbalancesDocument65 pagesWk8 - Electrolyte Imbalances & Acid-Base ImbalancesPotato PceeNo ratings yet
- Adrenal Glands: Adrenal Cortex Adrenal MedullaDocument66 pagesAdrenal Glands: Adrenal Cortex Adrenal MedullaRinto NugrohoNo ratings yet
- Endocrine 160110083024Document65 pagesEndocrine 160110083024Ryan CracknellNo ratings yet
- 2.3 HYPOCALCEMIA and HYPERCALCEMIADocument7 pages2.3 HYPOCALCEMIA and HYPERCALCEMIABooz Waief CaluzaNo ratings yet
- MS ReviewerDocument158 pagesMS ReviewerDexan Juridico100% (2)
- DKA To CRFDocument4 pagesDKA To CRFMark Anthony YabresNo ratings yet
- Pembahasan To Online 3Document201 pagesPembahasan To Online 3Fate DreamworkNo ratings yet
- Nursing Care Plan For LEUKEMIASDocument12 pagesNursing Care Plan For LEUKEMIASMaverick LimNo ratings yet
- Endocrinology Notes for Medical StudentsFrom EverandEndocrinology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (1)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Wonders of Homeopathy : 80 Homeo Remedies for your Health Problems : Healing with Homeopathy: Healing with HomeopathyFrom EverandWonders of Homeopathy : 80 Homeo Remedies for your Health Problems : Healing with Homeopathy: Healing with HomeopathyNo ratings yet
- CLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSFrom EverandCLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSNo ratings yet
- Internal Medicine: Over 200 Case StudiesFrom EverandInternal Medicine: Over 200 Case StudiesRating: 4.5 out of 5 stars4.5/5 (17)
- Clinical Signs in Humans and Animals Associated with Minerals, Trace Elements and Rare Earth ElementsFrom EverandClinical Signs in Humans and Animals Associated with Minerals, Trace Elements and Rare Earth ElementsNo ratings yet
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Taller de Calor EstDocument2 pagesTaller de Calor EstDiegoMuñozNo ratings yet
- Four Course Meal Plan and BudgetDocument5 pagesFour Course Meal Plan and BudgetPemphoNo ratings yet
- Steel Code Check Theory EnuDocument341 pagesSteel Code Check Theory Enupopaciprian27No ratings yet
- Introduction to measurement uncertainty components and calculationsDocument33 pagesIntroduction to measurement uncertainty components and calculationsLOUKILkarimNo ratings yet
- Postdoctoral Research Associate in Functional Organic MaterialsDocument6 pagesPostdoctoral Research Associate in Functional Organic MaterialsTheo GazisNo ratings yet
- Spring 2009 Midterm Opkst Mth601Document10 pagesSpring 2009 Midterm Opkst Mth601Khurram NadeemNo ratings yet
- Aghora and Tantra: Using Hawan To Appease Indra and YamaDocument3 pagesAghora and Tantra: Using Hawan To Appease Indra and YamaMahesh BadgujarNo ratings yet
- Briarborn - Nature's ProtectorsDocument6 pagesBriarborn - Nature's Protectorsa1057soulNo ratings yet
- Internship Report FACTDocument16 pagesInternship Report FACTBennetHailinkNo ratings yet
- 986.33 Mesofilos Aerobios-PetrifilmDocument1 page986.33 Mesofilos Aerobios-PetrifilmBleidy NieblesNo ratings yet
- Sentron: Reliable - From ExperienceDocument16 pagesSentron: Reliable - From ExperiencehaydarNo ratings yet
- Technical Specification For Sorghum GrainsDocument6 pagesTechnical Specification For Sorghum GrainsMohd SaifulNo ratings yet
- Chain Surveying InstrumentsDocument5 pagesChain Surveying InstrumentsSachin RanaNo ratings yet
- Yutra 3Document31 pagesYutra 3ကိုနေဝင်းNo ratings yet
- #5class-8 (Cordova) Chapter-6 SCIENCE Coal and PetroleumDocument2 pages#5class-8 (Cordova) Chapter-6 SCIENCE Coal and PetroleumVivek PatidarNo ratings yet
- Edward Jumper: Willow & Lark 2017 Designed UsingDocument9 pagesEdward Jumper: Willow & Lark 2017 Designed UsingMiraNo ratings yet
- 201 CH 8 Roadmap AnswersDocument2 pages201 CH 8 Roadmap AnswersdraggedfromthemoonNo ratings yet
- Determination of Melting Point of An Organic CompoundDocument4 pagesDetermination of Melting Point of An Organic CompoundyteyetyeNo ratings yet
- Agilent DSO5014A Oscilloscope Tutorial: EE105 Lab ExperimentsDocument6 pagesAgilent DSO5014A Oscilloscope Tutorial: EE105 Lab ExperimentshendraprimaNo ratings yet
- Price List Lang Technovation 02072019Document5 pagesPrice List Lang Technovation 02072019api-541004165No ratings yet
- Roland RD-800 Manuale Stage PianoDocument64 pagesRoland RD-800 Manuale Stage PianoAlberto FicheraNo ratings yet
- The Guitar in The Middle Ages and RenaisDocument4 pagesThe Guitar in The Middle Ages and RenaisТаня АфанасьеваNo ratings yet
- 23 Section I GW Glasses Window System and MirrorsDocument58 pages23 Section I GW Glasses Window System and Mirrorsamir8100No ratings yet
- Replacing ATA5567/T5557/ TK5551 With ATA5577 Application NoteDocument5 pagesReplacing ATA5567/T5557/ TK5551 With ATA5577 Application NoteM0n3No ratings yet
- Co Existence of Low and High Heat Flow Anomalies On The South Balearic Margin and Algerian Oceanic BasinsDocument19 pagesCo Existence of Low and High Heat Flow Anomalies On The South Balearic Margin and Algerian Oceanic BasinsmariaNo ratings yet
- Class Guide - Soldier Wheelman PDFDocument105 pagesClass Guide - Soldier Wheelman PDFRalph VasquezNo ratings yet
- Island of The Blue Dolphins: Before You Read The ChaptersDocument12 pagesIsland of The Blue Dolphins: Before You Read The ChaptersCostea CibanuNo ratings yet
- Gigabyte Z590 Gaming-XDocument52 pagesGigabyte Z590 Gaming-XjanchixnsNo ratings yet
- KA350 Pilot Checklist PN-73 PDFDocument142 pagesKA350 Pilot Checklist PN-73 PDFCarlos Anderez100% (13)
- MAYTAG MDE28PNCGW0 TechSheet-W10589718-RevADocument8 pagesMAYTAG MDE28PNCGW0 TechSheet-W10589718-RevAAngel MartinezNo ratings yet