Professional Documents
Culture Documents
Ann Clin Biochem-2009-Guy-468-76
Uploaded by
keyssiOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Ann Clin Biochem-2009-Guy-468-76
Uploaded by
keyssiCopyright:
Available Formats
Original Article
Protein and albumin-to-creatinine ratios in random urines
accurately predict 24 h protein and albumin loss
in patients with kidney disease
Mark Guy1, Joanna K Borzomato1,5, Ronald G Newall2, Philip A Kalra3 and Christopher P Price4
1
Department of Clinical Biochemistry, Salford Royal NHS Foundation Trust, Hope Hospital, Salford; 2Highover Park, Amersham, Bucks;
3
Department of Renal Medicine, Salford Royal NHS Foundation Trust, Salford; 4Department of Clinical Biochemistry, University of Oxford,
Oxford, UK; 5Present address: Department of Clinical Biochemistry, Royal Albert Edward Infirmary, Wigan, UK
Corresponding author: Mark Guy. Email: mark.guy@srft.nhs.uk
Abstract
Background: Random urine protein-to-creatinine (PCR) and albumin-to-creatinine (ACR) ratios have been proposed as
alternatives to 24 h urine measurements to simplify sample collection and overcome errors. The aim of this study was to
examine the ability of PCR and ACR to predict urinary 24 h protein and albumin loss, respectively, in patients with kidney
disease, and determine the most appropriate time of collection.
Methods: Eighty-three patients were recruited from a renal outpatient clinic. In a 24 h period, each collected an early-morning
urine (EMU), second and third voids, and the remaining urine passed that day. PCR and ACR were determined in random
urines and compared with the 24 h loss of protein and albumin, respectively.
Results: For all patients, median (range) 24 h urine protein and albumin losses were 220 (30– 15600) and 60 (,8 –10,557) mg,
respectively. Ratios derived from each of three random urines correlated well with 24 h protein or albumin loss (Spearman’s
rs . 0.87, P , 0.0001). Receiver operator characteristic (ROC) curve analysis showed PCR accurately predicted both an
abnormal 24 h urine protein !150 mg/24 h (areas under curves [AUC] 0.90–0.92) and significant proteinuria above 300 mg/
24 h (AUC between 0.97 and 1.00). ACR accurately predicted both an abnormal 24 h urine albumin !30 mg/24 h (AUC 0.98 to
0.99) and frank albuminuria at !300 mg/24 h or !700 mg/24 h (AUC between 0.99 and 1.00). EMU and random urines
performed equally well in predicting proteinuria and albuminuria from PCR and ACR, respectively.
Conclusions: By careful choice of cut-offs, both PCR and ACR can be used in patients with kidney disease to rule in or
rule out abnormal 24 h losses of protein and albumin. EMU and, importantly, random samples can be used as surrogates for
24 h urine collections.
Ann Clin Biochem 2009; 46: 468– 476. DOI: 10.1258/acb.2009.009001
Introduction urine collection, the variability of results obtained by this
The identification and quantitation of proteinuria is of impor- method make this view questionable. Quoted reference
tance in the initial diagnosis and subsequent follow-up and ranges for 24 h protein loss vary, but most would regard a
monitoring of renal disease.1,2 Proteinuria is also recognized protein loss of more than 150 mg/24 h as abnormal with sig-
as an independent risk factor for cardiovascular disease and nificant proteinuria being greater than 300 mg/24 h.13
as a predictor of end organ damage.3 – 5 More specifically, Urine albumin measurements have been used as a more sen-
urine albumin measurement now has an established role in sitive measure and early marker for nephropathy6 and there is
the early identification and monitoring of diabetic nephropa- now much support advocating the use of urine albumin
thy6 and, relatively recently, has been identified as an indi- measurement rather than total protein14,15 because detection
cator of cardiovascular risk in renal, hypertensive and other of ‘low-level’ albuminuria, important in the therapeutic
patients.7,8 Thus, urine protein or albumin measurements approach to a patient, may be masked by tests that measure
now form a central part of the classification and guidelines total protein. Urine albumin losses in the normal individual
for chronic kidney disease (CKD).9 – 12 are usually ,30 mg/24 h (and often below 10 mg/24 h),
There is no ‘gold standard’ for identifying proteinuria with 30–300 mg/24 h being within the ‘microalbuminuric’
and, although it has been generally accepted that the best range.16,17 Urinary losses above 300 mg/24 h would be
measure of protein or albumin loss is that based on a 24 h regarded as frank albuminuria (clinically overt proteinuria).
Annals of Clinical Biochemistry 2009; 46: 468 –476
Downloaded from acb.sagepub.com by guest on April 24, 2016
Guy et al. PCR and ACR in patients with kidney disease 469
................................................................................................................................................
Twenty-four hour urine collections, however, can be cum- immunoturbidimetry.35 The lower limits of detection for
bersome to perform and prone to errors in collection.18 For urine protein and albumin assays were 20 and 8 mg/L,
this reason, the use of protein or albumin-to-creatinine ratios respectively. Between-day coefficients of variation for the
(PCR or ACR) in random urine samples has been pro- urine protein assay were 2.2% and 4.3% at concentrations
posed.19 ACRs have been evaluated extensively in patients of 161 and 550 mg/L, respectively. For the urine albumin
with diabetes20 – 22 and several studies have examined the assay, they were 2.0% and 2.6% at concentrations of
utility of PCRs in predicting proteinuria, primarily in hyper- 26.7 and 97.5 mg/L, respectively and for urine creatinine
tensive pregnancy23,24 and paediatric settings.25,26 There they were 1.7% and 1.8% at concentrations of 12.7 and
have been relatively few studies in renal disease27 – 30 and 5.7 mmol/L, respectively. For the purposes of this study,
there is little data at present which shows the ability of random urines with undetectable protein or albumin con-
ACR to predict proteinuria in non-diabetic patients. Most centrations were, respectively, designated as having a PCR
studies have demonstrated a good relationship between cal- of 5 mg/mmol and ACR of 0.5 mg/mmol. The 24 h urines
culated ratios and 24 h protein loss and some have quoted with undetectable albumin were designated an albumin
predictive values for identifying significant proteinuria. loss of 5 mg/24 h.
Few, however, have indicated the confidence with which Statistical analyses on the data were performed using
creatinine ratios can rule in or rule out proteinuria. One sys- Analyse-it for Excel (Analyse-it Software Ltd, Leeds, UK).
tematic review of studies using random urine PCR con- Spearman’s rank correlation was used to compare urine
cluded that they provided evidence to rule out significant PCR and ACR with 24 h protein and albumin loss, respect-
proteinuria as defined by a 24 h measurement.13 ively. The ability of urine PCR and ACR at various cut-offs
The aim of this study was to assess the ability of PCR and to predict abnormal 24 h protein or albumin loss was deter-
ACR from random urine samples to rule in or rule out pro- mined from receiver operator characteristic (ROC) curve
teinuria or albuminuria in patients with kidney disease analysis and by calculation of sensitivities, specificities, pre-
attending a nephrology clinic. In addition, by collecting dictive values and likelihood ratios (LRs). A negative likeli-
urine at different points during the day, the most appropri- hood ratio (LR[2], false-positive rate/true negative rate) of
ate random urine sample, if any, could be determined. ,0.1 and positive likelihood ratio (LR[þ], true positive rate/
false-negative rate) greater than 10 were taken to indicate
good test performance.36 Areas under ROC curves were
Patients compared using the method of DeLong et al. 37
A total of 117 outpatients with various stages of CKD and
requiring 24 h urine total protein measurement as part of
their clinical investigation or management were enrolled Results
in the study between September and December 2005. Patient characteristics
Patients were consecutive and recruited from one consult-
Of the 117 patients who consented to be involved in the
ant’s (PAK) nephrology clinic. Other parts of the study
study, 86 (73.5%) returned urine samples. Two urine
have been reported elsewhere.31,32 The study was approved
collections of ,500 mL in volume and one having a 24 h
by Greater Manchester Local Ethics Committees with signed
urine creatinine output ,3.0 mmol were rejected on the
written consent being obtained from each patient.
assumption that they might not have been complete 24 h
collections. The main contributory causes of CKD in the
remaining 83 patients were diabetic nephropathy (n ¼ 17),
Methods hypertensive damage (n ¼ 13), renovascular (n ¼ 18),
Each patient was asked to collect urine in the 24 h period glomerulonephritis/glomerulosclerosis (n ¼ 16) (including
immediately prior to their nephrology clinic appointment IgA nephropathy [n ¼ 6]), tubulointerstitial damage (n ¼
as follows. After discarding the first sample of the day, 5) and amyloidosis (n ¼ 1). Causes in 10 patients were not
urine was collected in four separate containers: (i) second certain or under investigation.
void; (ii) third void; (iii) remaining urine passed that day; There were 25 patients with diabetes mellitus and 53 had
and (iv) early-morning urine (EMU) passed the following documented hypertension (10 of these patients were subop-
day. Urine was collected into containers without preserva- timally controlled). One patient had stage 1 CKD, with
tive and stored at 48C prior to analysis, which was usually 11 (13%), 35 (42%), 27 (33%) and 9 (11%) patients having
within 24– 48 h of receipt. stages 2, 3, 4 and 5, respectively. Seventy-two percent
Urine protein, albumin and creatinine were measured on were men and the median age for all patients was 67
each of samples (i), (ii) and (iv) and PCR and ACRs (both years. For all patients, median (range) 24 h urinary protein
mg/mmol) calculated. All four aliquots were then pooled, loss was 220 (30– 15,600) mg/24 h and median (range)
the volume measured, and protein and albumin measure- 24 h albumin loss was 60 (,8– 10557) mg/24 h (Table 1).
ments repeated to give the 24 h outputs of each.
All assays were performed on the Roche Integra 800
(Roche Diagnostics Ltd, Burgess Hill, UK) using reagent Protein:creatinine ratio versus 24 h urine protein
kits and calibrators supplied by the manufacturer. Urine There was a very good correlation between 24 h urine protein
protein was measured using pyrogallol red,33 urine creati- loss and PCR in second and third voids and EMUs
nine by a kinetic Jaffe method34 and urine albumin by (Figures 1a–c), and these correlations were very similar for
Downloaded from acb.sagepub.com by guest on April 24, 2016
470 Annals of Clinical Biochemistry Volume 46 November 2009
................................................................................................................................................
(a) 10,000
albuminuria
Prevalence
Table 1 Patient characteristics and median (range) age, 24 h urine volumes and outputs of protein, albumin and creatinine. Prevalence data refers to patients with 24 h urinary loss of protein
1000
65.1
70.0
52.2
(%)
PCR (mg/mmol)
100
Prevalence
proteinuria 10
65.1
70.0
52.2
(%)
1
10 100 1000 10,000 100,000
60 (,8–10557)
66 (,8–10557)
Urine Albumin
40 (,8–1531)
Urine total protein (mg/24 h)
mg/24 h
(b) 10,000
1000
220 (30 – 15600)
220 (50 – 15600)
PCR (mg/mmol)
195 (30 – 1650)
Urine Protein
100
mg/24 h
10
1.57 (0.70 –2.9)
1.43 (0.96 –2.9)
Urine volume
1.60 (0.7 – 2.7)
1
10 100 1000 10,000 100,000
L/24 h
Urine total protein (mg/24 h)
(c) 10,000
7.7 (3.5 – 16.4)
8.5 (4.4 – 16.4)
6.6 (3.5 –9.6)
mmol/24 h
creatinine
1000
PCR (mg/mmol)
Urine
100
10
67 (28 –86)
67 (28 –86)
67 (33 –80)
Age (y)
1
10 100 1000 10,000 100,000
Urine total protein (mg/24 h)
5
9
4
5
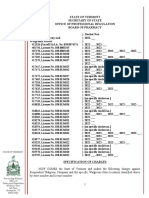
Figure 1 Protein-to-creatinine ratio measured in random urines compared
with 24 h urine protein loss. (a) ¼ Second void, (b) ¼ third void, (c) ¼ early-
morning urine. Spearman rank correlation coefficients were (a) 0.90, (b)
27
19
8
4
0.91, (c) 0.87; P , 0.0001 for all
each of the three urine aliquots. ROC curve analysis showed
35
28
7
3
with CKD stage
PCR to be a good predictor of both abnormal urine protein
No. of patients
!150 mg/24 h or albumin !30 mg/24 h
loss !150 mg/24 h and clinically significant urine protein
11
9
2
loss above 300 mg/24 h (Table 2). There were no significant
2
differences between areas under curves (AUC) generated
from each of the three urine aliquots (P . 0.05 for all
CKD, chronic kidney disease
1
1
0
1
cases), suggesting they were equally good at predicting pro-
teinuria. The ability of PCR to predict or exclude significant
83
60
23
n
24 h protein loss of !500 mg was assessed for each aliquot
at various PCR cut-offs (Table 3). For each PCR cut-off, calcu-
lated LRs and predictive values were similar between each of
All patients
Females
the three urine aliquots. At cut-offs of 70 mg/mmol and
Males
below, PCR showed good ability in ruling out significant
proteinuria denoted by negative likelihood ratios (LR2) of
Downloaded from acb.sagepub.com by guest on April 24, 2016
Guy et al. PCR and ACR in patients with kidney disease 471
................................................................................................................................................
Table 2 Areas under curves (AUC) generated from receiver operator (Figures 2a –c) and again correlations were very similar for
characteristic analysis showing the ability of protein-to-creatinine each of the three urine aliquots. ROC curve analysis
ratios (PCRs) from random urines to predict 24 h urine protein loss
!150, !300, !500 or 1000 mg/24 h
showed that ACR in each random urine adequately
predicted a 24 h albumin loss of !30, !300 and !700 mg
Urine total protein
(Table 5). EMU, and second and third voids were equally
loss (mg/24 h) Urine aliquot AUC 95% CI AUC
good at predicting albuminuria, as there was no significant
!150 Second void 0.91 0.85 –0.97 difference between AUCs generated from each of the three
Third void 0.92 0.87 –0.98
EMU 0.90 0.84 –0.97
urine aliquots (P . 0.05 for all cases). Using an ACR
!300 Second void 0.97 0.94 –1.00 cut-off of 30 mg/mmol, all three urine aliquots showed a
Third void 0.98 0.96 –1.00 similar good performance in being able to rule in or rule
EMU 0.97 0.93 –1.00 out significant albuminuria (!300 mg/day), denoted by
!500 Second void 1.00 0.99 –1.00
LRþ .10 and LR2 ,0.1, respectively (Table 6). All three
Third void 0.99 0.97 –1.00
EMU 0.99 0.98 –1.00 urine aliquots showed similar ability in predicting albumi-
!1000 Second void 0.99 0.97 –1.00 nuria for 24 h outputs of 300 and 700 mg. ACR cut-offs
Third void 0.99 0.97 –1.00 that gave optimum sensitivities and specificities for predict-
EMU 0.98 0.96 –1.00 ing albuminuria at these levels are shown in Table 7.
AUC, areas under curves; CI, confidence interval
(EMU, early-morning urine)
Total protein versus albumin
approximately 0.1 or below. The ability to rule in significant Figure 3 shows the relationship between albumin and total
proteinuria, denoted by positive likelihood ratios (LRþ) of protein in 24 h urines (n ¼ 83). At significant urinary total
approximately 10 or above, was seen at PCR cut-offs above protein losses (.1000 mg/24 h), there was a good corre-
50 mg/mmol. All three urine aliquots also showed similar lation (Spearman’s r ¼ 0.87, P , 0.0001) between the two
ability in predicting proteinuria for other 24 h outputs of with albumin contributing to the majority of the total
150, 300 and 1000 mg. PCR cut-offs that gave optimum protein present (median 89%, 95% range 67– 104%). With
sensitivities and specificities for predicting proteinuria at urinary losses .1000 mg/24 h, the Cusum linearity test
these levels are shown in Table 4. showed a linear relationship between the two (P . 0.1).
At lower urinary protein losses (,1000 mg/24 h), albumin
as a percentage of total protein was much more variable
Albumin:creatinine ratio versus 24 h urine albumin (Spearman’s r ¼ 0.71, P , 0.0001, median 27%, 95% range
For each patient, ACR from second and third voids and 2 –92%) and the linear relationship between the two was
EMUs correlated extremely well with 24 h albumin loss lost (Cusum linearity test, P , 0.01).
Table 3 Likelihood ratios (LRs) and predictive values for each urine aliquot in predicting a 24 h urine protein loss of !500 mg/24 h
PCR
cut-off Sensitivity Specificity
(mg/mmol) Urine (%) (%) PV1 PV2 LR1 LR2
10 (a) 100 6 0.36 1.00 1.1 0.0
(b) 100 9 0.37 1.00 1.1 0.0
(c) 100 7 0.37 1.00 1.1 0.0
15 (a) 100 19 0.40 1.00 1.2 0.0
(b) 100 22 0.41 1.00 1.3 0.0
(c) 100 35 0.45 1.00 1.5 0.0
20 (a) 100 30 0.43 1.00 1.4 0.0
(b) 100 41 0.48 1.00 1.7 0.0
(c) 100 54 0.54 1.00 2.2 0.0
30 (a) 100 56 0.55 1.00 2.3 0.0
(b) 100 69 0.63 1.00 3.2 0.0
(c) 100 76 0.69 1.00 4.2 0.0
50 (a) 100 87 0.81 1.00 7.7 0.0
(b) 93 85 0.77 0.96 6.3 0.1
(c) 100 87 0.81 1.00 7.7 0.0
70 (a) 100 96 0.94 1.00 27.0 0.0
(b) 90 98 0.96 0.95 48.4 0.1
(c) 83 100 1.00 0.93 high 0.1
100 (a) 69 100 1.00 0.86 high 0.3
(b) 70 100 1.00 0.86 high 0.3
(c) 69 100 1.00 0.86 high 0.3
200 (a) 38 100 1.00 0.75 high 0.6
(b) 38 100 1.00 0.75 high 0.6
(c) 28 100 1.00 0.72 high 0.7
PCR, protein-to-creatinine ratio
(a) ¼ second void, (b) ¼ third void, (c) ¼ early-morning urine. PVþ, PV2 ¼ positive, negative predictive values. LRþ, LR2 ¼ positive, negative LRs
Downloaded from acb.sagepub.com by guest on April 24, 2016
472 Annals of Clinical Biochemistry Volume 46 November 2009
................................................................................................................................................
Table 4 Optimum PCR cut-offs for predicting 24 h urine protein Table 5 AUCs generated from ROC analysis showing the ability of
losses of 150, 300, 500 and 1000 mg ACRs from random urines to predict 24 h urine albumin losses !30,
!300 and !700 mg/24 h
Total
protein PCR Sensitivity Specificity Urine albumin
mg/24 h Urine cut-off (%) (%) LR1 LR2 loss (mg/24 h) Urine aliquot AUC 95% CI AUC
150 (a) 31 84 86 5.9 0.2 !30 Second void 0.98 0.96 –1.00
(b) 27 84 86 5.9 0.2 Third void 0.99 0.98 –1.00
(c) 23 78 79 3.7 0.3 EMU 0.98 0.96 –1.00
300 (a) 47 91 92 11.0 0.1 !300 Second void 1.00 0.99 –1.00
(b) 45 91 92 11.0 0.1 Third void 1.00 1.00 –1.00
(c) 50 94 94 15.0 0.1 EMU 1.00 1.00 –1.00
500 (a) 72 97 96 26.1 0.0 !700 Second void 1.00 1.00 –1.00
(b) 57 93 93 16.8 0.1 Third void 0.99 0.97 –1.00
(c) 60 93 94 16.8 0.1 EMU 1.00 0.99 –1.00
1000 (a) 123 93 93 12.8 0.1
(b) 115 93 93 12.8 0.1 AUC, areas under curves; CI, confidence interval; ACR,
(c) 105 93 93 12.8 0.1 albumin-to-creatinine ratio
(EMU, early-morning urine)
PCR, protein-to-creatinine ratio; LRþ, positive likelihood ratio; LR2,
negative likelihood ratio
(a) ¼ second void, (b) ¼ third void, (c) ¼ early-morning urine. LRþ, LR2 ¼ Twenty-nine out of 83 patients had evidence of clinically
positive, negative likelihood ratios significant proteinuria with urine protein !500 mg/24 h. Six
(a) 10,000
of these samples had 24 h urinary albumin losses ,300 mg
(range ,8– 196 mg). There were no patients with urine
1000
albumin !300 mg/24 h and urine protein , 500 mg/24 h.
Similarly 15 patients had evidence of heavy proteinuria
ACR (mg/mmol)
100 with urine protein !1000 mg/24 h with only one having
urine albumin levels lower than 700 mg/24 h (684 mg/
10 24 h). Three patients had urine albumin .700 mg/24 h
and urine protein lower than 1000 mg/24 h (values
1 between 740 and 780 mg/24 h). Table 8 shows optimum
sensitivities and specificities for random urine ACR in pre-
0 dicting 24 h protein outputs of 150, 300, 500 and 1000 mg.
1 10 100 1000 10,000 100,000
Urine albumin (mg/24 h)
(b) 10,000 Discussion
1000 Collection of 24 h urine samples is cumbersome and prone
to errors, hence analyte measurement in random urine is
ACR (mg/mmol)
100 often proposed with correction for variation in urine flow
rate by expressing results as a ratio to creatinine concen-
10
tration. It was not possible to formally assess completeness
1
of collection of 24 h samples, particularly as there is little
published data for patients with CKD. Although samples
0 were from a well-motivated group of patients who regularly
1 10 100 1000 10,000 100,000 made 24 h urine collections, a pragmatic approach was
Urine albumin (mg/24 h) adopted to reject samples that had either unusually low
(c) 10,000
urine volume or creatinine outputs, on the premise that
they may not have been a complete 24 h collection. As a
1000 result, only 71% of patients enrolled in this study returned
or provided viable samples highlighting the inconvenience
ACR (mg/mmol)
100 and errors associated with 24 h urine collection.
Several studies have assessed the benefits of using
10 random urine PCR as a surrogate for 24 h protein measure-
ment, but relatively few of these have involved patients with
1 kidney disease, or have examined the ability of PCRs or
ACRs to rule in or rule out abnormal protein loss. Most
0 studies have shown good correlations between PCR and
1 10 100 1000 10,000 100,000 24 h protein loss and have demonstrated adequate sensi-
Urine albumin (mg/24 h) tivities and specificities when PCR was used to predict
24 h proteinuria. However, cut-offs used to define abnormal
Figure 2 Albumin-to-creatinine ratio measured in random urines compared
PCR or abnormal protein loss have varied widely. Thus,
with 24 h urine albumin loss. (a) ¼ Second void, (b) ¼ third void, (c) ¼ early-
morning urine. Spearman rank correlation coefficients were (a) 0.97, (b) Gai et al. 27 in predicting a 24 h urine protein loss .150 mg
0.96, (c) 0.97; P , 0.0001 for all from a PCR ! 11.3 mg/mmol, obtained sensitivities and
Downloaded from acb.sagepub.com by guest on April 24, 2016
Guy et al. PCR and ACR in patients with kidney disease 473
................................................................................................................................................
Table 6 LRs and predictive values for each urine aliquot in predicting a 24 h urine albumin loss of !300 mg/day
ACR cut-off
(mg/mmol) Urine Sensitivity (%) Specificity (%) PV1 PV2 LR1 LR2
10 (a) 100 72 0.58 1.00 3.5 0.0
(b) 100 68 0.55 1.00 3.2 0.0
(c) 100 78 0.64 1.00 4.6 0.0
15 (a) 100 85 0.72 1.00 6.7 0.0
(b) 100 83 0.70 1.00 6.0 0.0
(c) 100 90 0.79 1.00 10.0 0.0
20 (a) 100 92 0.82 1.00 12.0 0.0
(b) 100 87 0.74 1.00 7.5 0.0
(c) 100 93 0.85 1.00 15.0 0.0
30 (a) 100 93 0.85 1.00 15.0 0.0
(b) 100 93 0.85 1.00 15.0 0.0
(c) 100 97 0.92 1.00 30.0 0.0
50 (a) 96 98 0.96 0.98 57.4 0.1
(b) 91 98 0.96 0.97 54.8 0.1
(c) 92 100 1.00 0.97 High 0.1
70 (a) 87 98 0.95 0.95 52.2 0.2
(b) 91 98 0.96 0.97 54.8 0.1
(c) 78 100 1.00 0.92 High 0.2
100 (a) 78 100 1.00 0.92 High 0.2
(b) 74 100 1.00 0.91 High 0.3
(c) 57 100 1.00 0.86 High 0.4
200 (a) 39 100 1.00 0.79 High 0.6
(b) 44 100 1.00 0.82 High 0.6
(c) 30 100 1.00 0.79 High 0.7
ACR, albumin-to-creatinine ratio; LR, likelihood ratio;
(a) ¼ second void, (b) ¼ third void, (c) ¼ early-morning urine. PVþ, PV2 ¼ positive, negative predictive values. LRþ, LR2 ¼ positive, negative LRs
Table 7 Optimum ACR cut-offs for predicting 24 h urine albumin 100,000
outputs of 30, 300, and 700 mg
Urine ACR
albumin cut- Sensitivity Specificity 10,000
mg/24 h Urine off (%) (%) LR1 LR2
Albumin (mg/24 h)
30 (a) 6 93 93 13.4 0.1
1000
(b) 6 96 97 27.9 0.0
(c) 4 96 97 27.9 0.0
300 (a) 50 96 98 57.4 0.0
(b) 43 96 98 57.4 0.0 100
(c) 40 100 100 high 0.0
700 (a) 109 94 99 62.1 0.1
(b) 80 88 92 11.7 0.1 10
(c) 65 94 97 31.0 0.1
ACR, albumin-to-creatinine ratio 1
(a) ¼ second void, (b) ¼ third void, (c) ¼ early-morning urine. LRþ, 1 10 100 1000 10,000 100,000
LR2 ¼ positive, negative likelihood ratios
Protein (mg/24 h)
Figure 3 Relationship between albumin and total protein in 24 h urines
(n ¼ 83). Samples with undetectable albumin levels have been assigned a
specificities of 91% and 75%, respectively. Similarly Lane 24 h value of 5 mg
et al.,30 using thresholds of between 300 mg/L and 3.0 g/L
to define abnormal 24 h proteinuria, obtained sensitivities
between 85% and 93% and specificities between 80% and to be a good predictor of 24 h urine protein loss (Table 2).
91% at varying PCR cut-offs. Importantly, there was no statistical difference between
Many studies have used a 24 h protein output of greater areas under the curves generated from EMU, second or
than 300 mg to indicate clinically significant proteinuria.13 third voids suggesting any would be equally effective as a
Recent guidelines have used higher levels of 500 mg/24 h substitute for the 24 h urine. In addition, the data show
and 1 g/24 h (roughly equivalent to PCR of 50 and that, by using an appropriate cut-off, PCR can be a reliable
100 mg/mmol, respectively) to denote significant proteinuria tool for ruling in or ruling out abnormal 24 h protein loss.
and to define levels at which treatment should be insti- For example, at PCR greater than 50 mg/mmol, there is
tuted.9,12,38 In this study, we have demonstrated good corre- strong evidence to be able to rule in significant proteinuria
lation between 24 h urine protein loss and PCR in second and of 500 mg/24 h or more, demonstrated by LRþ greater
third voids and EMUs (Figures 1a–c). Furthermore, ROC than 10. Likewise at PCR below 50 mg/mmol, there is
curve analysis at multiple 24 h protein cut-offs showed PCR strong evidence to be able to rule out significant 24 h
Downloaded from acb.sagepub.com by guest on April 24, 2016
474 Annals of Clinical Biochemistry Volume 46 November 2009
................................................................................................................................................
Table 8 Optimum albumin-to-creatinine ratio cut-offs for predicting Recent guidelines have recommended the use of urine
24 h urine protein outputs of 150, 300, 500, 1000 mg albumin measurement in preference to total protein.9,10,12
Total ACR Some also quote approximate equivalence points for urine
protein cut- Sensitivity Specificity protein and albumin. For example, the National Institute
mg/24 h Urine off (%) (%) LR1 LR2
for Health and Clinical Excellence12 quote ACRs of 30 and
150 (a) 6 72 72 2.6 0.4 70 mg/mmol to be roughly approximate to 24 h protein
(b) 7 72 76 3.0 0.4 outputs of 500 mg and 1 g, respectively. The Scottish
(c) 5 79 80 4.0 0.3
300 (a) 12 86 84 5.9 0.2
Intercollegiate Guidelines Network38 quote an ACR of
(b) 11 80 83 4.8 0.2 30 mg/mmol being equivalent to protein loss of 450 mg/
(c) 9 83 83 5.0 0.2 24 h. Thresholds for diagnosis and treatment of clinically
500 (a) 15 86 87 6.7 0.2 significant proteinuria have therefore been suggested at
(b) 17 86 87 6.7 0.2
ACR levels of 30 and 70 mg/mmol (approximately equival-
(c) 12 86 87 6.7 0.2
1000 (a) 109 93 96 21.2 0.1 ent to 24 h albumin outputs of 300 and 700 mg).9,10,12 Our
(b) 93 93 96 21.2 0.1 data suggest that either urine albumin or urine total
(c) 64 87 93 11.8 0.1 protein measurements would be equally good in assessing
or monitoring significant proteinuria, particularly for
ACR, albumin-to-creatinine ratio
(a) ¼ second void, (b) ¼ third void, (c) ¼ early - morning urine. LRþ, protein outputs greater than 1 g/24 h. Below 1 g/24 h, the
LR2 ¼ positive, negative likelihood ratios situation is less clear as the correlation between albumin
and total protein is more variable. This is highlighted by
the data in Table 8. Optimum ACR cut-offs for predicting
protein loss, as demonstrated by LR2 ,0.1 (Table 3). 24 h protein outputs at levels ,1 g/24 h are much lower
Similarly random urine PCR may be used effectively to than might be expected. Furthermore, six out of 29 patients
rule in or rule out other levels of proteinuria (Table 4). with significant proteinuria .500 mg/24 h had albumin
ACR now has an established role in the diagnosis outputs lower than the 300 mg/24 h threshold. If these
and monitoring of diabetic nephropathy.20 There are an data can be extrapolated to other patient populations, indi-
increasing number of studies using ACR in patients with viduals would have been potentially misclassified using
hypertension8,39 – 41 but there are few studies in other, non- guidelines based solely on ACR. This is in contrast to
diabetic groups. Most studies, however, have shown that Collier et al.,49 who found few discordant ACR and PCR
random urine ACR correlates well with 24 h albuminuria results in a study of 117 patients.
and demonstrate adequate sensitivity and specificity in pre- ACR measurements, however, have distinct advantages
dicting 24 h albuminuria.42 – 45 This study in renal outpati- due to the superior analytical sensitivity of assays. This is
ents has also shown good agreement between ACR and especially true for detecting early nephropathy in diabetics
24 h albumin loss (Figure 2) and ACR from each of the and possibly other high-risk groups, for example, patients
first, second and third voids predict 24 h albumin output with hypertension or cardiovascular disease.
equally well (Table 5). An ACR cut-off of 30 mg/mmol accu- This study has been limited by its relatively small size and
rately rules in or out significant albuminuria !300 mg/24 h, being restricted to one centre using hospital patients with
as denoted by LRþ .10 or LR2 ,0.1, respectively kidney disease. Owing to the small sample size, there
(Table 6). Lower cut-offs of between 4 and 6 mg/mmol were insufficient results to delineate the data by gender or
could be used to rule in or rule out albumin loss in the renal pathology. In diabetic patients, it has been demon-
‘microalbuminuric’ range, which is perhaps of greater strated that gender-specific cut-off values improve the diag-
importance in screening for renal disease (Table 7). nostic performance of ACR.21,50 Use of such cut-offs may
Most guidelines state that EMU is the preferred sample enhance the performance of ACR in patients with kidney
for ACR and PCR measurements, but this study has not disease. Further work needs to be undertaken to provide
found any advantage in using EMU over random such data and to establish whether our data can be extrapo-
samples. Reports in the literature are conflicting with lated to other patient groups.
some advocating EMU20,46 and others random urine In summary this study has shown that, in patients with
samples.18,47 There are benefits to both patients and clini- kidney disease, both random urine PCR and ACR accurately
cians if random ‘spot’ urines can be relied upon to accu- predict proteinuria and albuminuria, respectively. By
rately rule in or rule out proteinuria and provide an careful choice of cut-offs these ratios can be used to rule in
accurate quantitative measurement of proteinuria. or rule out abnormal 24 protein or albumin loss. If either
Albumin as a percentage of total protein is highly variable ACR or PCR is to be used as a first-line screening test for evi-
at lower levels of proteinuria (Figure 3) due to factors dence of renal disease, then the ratios could clearly be valu-
including a variable contribution from the tubular Tamm able as a rule-out test but early detection of proteinuria in
Horsfall glycoprotein, glomerular-filtered low molecular selected groups of patients may be best achieved using
weight proteins and, in some patients, paraproteins. As ACR. If the tests are to be used for monitoring the level of
urinary total protein levels approach and exceed 1 g/24 h, proteinuria or albuminuria in established renal disease,
the relative contribution from albumin increases and the they can then be used as surrogates for 24 h measurements.
ratio between albumin and total protein becomes relatively The finding that random urine aliquots are equally as accu-
constant. These findings are in agreement with other rate as EMU simplifies sample collection for both patients
published reports.14,48,49 and health-care workers.
Downloaded from acb.sagepub.com by guest on April 24, 2016
Guy et al. PCR and ACR in patients with kidney disease 475
................................................................................................................................................
DECLARATIONS 20 Marshall SM. Screening for microalbuminuria: which measurement?
Diabet Med 1991;8:706 –11
Competing interests: RN and CP were consultants to Bayer 21 Houlihan CA, Tsalamandris C, Akdeniz A, Jerums G. Albumin to
Corp., now Siemens., Healthcare Diagnostics Ltd, at the creatinine ratio: a screening test with limitations. Am J Kidney Dis
time this project was initiated. 2002;39:1183 – 9
22 Claudi T, Cooper JG. Comparison of urinary albumin excretion rate in
Funding: The study was supported by a grant from Siemens overnight urine and albumin creatinine ratio in spot urine in diabetic
Healthcare Diagnostics Ltd, USA. patients in general practice. Scan J Prim Health Care 2001;19:247 – 8
Ethical approval: The study was approved by Greater 23 Leanos-Miranda A, Marquez-Acost J, Romero-Arauz F, et al.
Manchester Local Ethics Committees (03/TG/063). Protein:creatinine ratio in random urine samples is a reliable marker of
Guarantor: MG. increased 24-hour protein excretion in hospitalized women with
hypertensive disorders of pregnancy. Clin Chem 2007;53:1623 – 8
Contributorship: All authors contributed to the study and 24 Gonsales Valerio E, Lopes Ramos JG, Martins-Costa SH, Muller AL.
to the writing of the paper. Variation in the urinary protein/creatinine ratio at four different
Acknowledgements: None. periods of the day in hypertensive women. Hypertens Pregnancy
2005;24:213 –21
25 Morgenstern BZ, Butani L, Wollan P, Wilson DM, Larson TS. Validity
of protein –osmolality versus protein-creatinine ratios in the estimation
REFERENCES of quantitative proteinuria from random samples of urine in children.
Am J Kidney Dis 2003;41:760 – 6
1 Remuzzi G, Bertani T. Pathophysiology of progressive nephropathies. 26 Nagasako H, Kiyoshi Y, Ohkawa T, et al. Estimation of 24-hour urine
N Engl J Med 1998;329:1448 – 56 protein quantity by the morning-urine protein –creatinine ratio. Clin Exp
2 Remuzzi G, Ruggenenti P, Benigni A. Understanding the nature of renal Nephrol 2007;11:142 –6
disease progression. Kidney Int 1997;51:2 –15 27 Gai M, Motta D, Giunti S, et al. Comparison between 24-h proteinuria,
3 Walls J. Relationship between proteinuria and progressive renal disease. urinary protein/creatinine ratio and dipstick test in patients with
Am J Kidney Dis 2001;37(Suppl. 2):S13–6 nephropathy: patterns of proteinuria in dipstick-negative patients.
4 Ruggenenti P, Perna A, Mosconi L, Pisoni R, Remuzzi G. Urinary protein Scand J Clin Lab Invest 2006;66:299 –307
excretion rate is the best predictor of ESRF in non-diabetic proteinuric 28 Morales JV, Weber R, Wagner MB, Barros EJG. Is morning urinary
chronic nephropathies. Kidney Int 1998;53:1209 –16 protein/creatinine ratio a reliable estimator of 24-hour proteinuria in
5 Segura J, Campo C, Ruilope LM. Proteinuria: an underappreciated risk patients with glomerulonephritis and different levels of renal function?
factor in cardiovascular disease. Curr Cardiol Rep 2002;4:458 –62 J Nephrol 2004;17:666– 72
6 Mogensen CE. Microabuminuria predicts clinical proteinuria and early 29 Ruggenenti P, Gaspari F, Perna A, Remuzzi G. Cross sectional
mortality in maturity-onset diabetes. N Engl J Med 1984;310:356 – 60 longitudinal study of spot morning urine protein:creatinine ratio, 24
7 Hillege HL, Fidler V, Diercks GF, et al. Prevention of Renal and Vascular hour urine protein excretion rate, glomerular filtration rate, and end
End Stage Disease (PREVEND) Study Group. Urine albumin excretion stage renal failure in chronic renal disease in patients without diabetes.
predicts cardiovascular and non cardiovascular mortality in the general BMJ 1998;316:504 – 9
population. Circulation 2002;106:777 – 82 30 Lane C, Brown M, Dunsmuir W, Kelly J, Mangos G. Can spot urine
8 Mariani M. Microalbuminuria, an integrated marker of cardiovascular protein/creatinine replace 24 h urine protein in usual clinical
risk in essential hypertension. J Hum Hypertens 2002;16:79 –89 nephrology? Nephrology 2006;11:245 –9
9 Levey AS, Coresh J, Balk E, et al. National Kidney Foundation. National 31 Guy M, Newall R, Borzomato J, Kalra P, Price C. Use of a first-line urine
Kidney Foundation practice guidelines for chronic kidney disease: protein-to-creatinine strip test on random urines to rule out proteinuria
evaluation, classification, and stratification. Ann Intern Med 2003;139: in patients with chronic kidney disease. Nephrol Dial Transplant 2009;
137– 47 24:1189 – 93
10 Levey AS, Eckardt KU, Tsukamoto Y, et al. Definition and classification 32 Guy M, Newall R, Borzomato J, Kalra P, Price C. Diagnostic accuracy of
of chronic kidney disease: a position statement from Kidney Disease: the urinary albumin: creatinine ratio determined by the CLINITEK
Improving Global Outcomes (KDIGO). Kidney Int 2005;67:2089 –100 Microalbumin and DCA 2000þ for the rule-out of albuminuria in
11 Joint Speciality Committee for Renal Disease. Royal College of chronic kidney disease. Clin Chim Acta 2009;399:54 – 8
Physicians of London and the Renal Association. Available at: http:// 33 Watanabe N, Kamei S, Ohkubo A, et al. Urine protein measured with a
www.renal.org/guidelines/print/CKDfinalMar07.pdf pyrogallol red-molybdate complex, manually and in a Hitachi 726
12 National Institute for Health and Clinical Excellence. Chronic Kidney autoanalyser. Clin Chem 1986;32:1551 –4
Disease: Early Identification and Management of Chronic Kidney Disease in 34 Bartels H, Böhmer M. Microdetermination of creatinine. Clin Chim Acta
Adults in Primary and Secondary Care. September 2008, Clinical guideline 1971;32:81 –5
73. Available at: www.nice.org.uk/Guidance/CG73 35 Gerbaut L. Immunoturbidimetry of albumin in serum, CSF and urine
13 Price CP, Newall RG, Boyd JC. Use of protein:creatinine ratio with a unique calibration curve. Clin Chem 1987;32:1260 –1
measurements on random urine samples for prediction of significant 36 Boyd JC. Statistical analysis and presentation of data. In: Price CP,
proteinuria: a systematic review. Clin Chem 2005;51:1577 –86 Christenson RH, eds. Evidence-based Laboratory Medicine, 2nd edn.
14 Newman DJ, Thakkar H, Medcalf EA, Gray R, Price CP. Use of urine Washington: AACC Press, 2007:113 –40
albumin measurement as a replacement for total protein. Clin Nephrol 37 DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas
1995;43:104 –9 under two or more correlated receiver operating characteristic curves:
15 Ballantyne FC, Gibbons J, O’Reilly D StJ. Urine albumin should replace a nonparametric approach. Biometrics 1988;44:837 – 45
total protein for the assessment of glomerular proteinuria. Ann Clin 38 Scottish Intercollegiate Guidelines Network. Diagnosis and Management of
Biochem 1993;30:101 –3 Chronic Kidney Disease. June 2008. Guideline No. 103. Available at: http://
16 National Service Framework for Diabetes. Department of Health, UK. www.sign.ac.uk/pdf/sign103.pdf
Available at: http://www.dh.gov.uk/en/Publicationsandstatistics/ 39 Segura J, Ruilope LM, Rodicio JL. Microalbuminuria. Clin Exp Hypertens
Publications/PublicationsPolicyAndGuidance/Browsable/DH_4917725 2004;26:701 –7
17 American Diabetes Association. Standards of medical care in diabetes 40 Viberti G. Regression of albuminuria: latest evidence for a new approach.
2007. Diabetes Care 2007;30(Suppl 1):S4 –S41 J Hypertens 2003;21(Suppl. 3):S24– 8
18 Shaw AB, Risdon P, Lewis-Jackson J. Protein creatinine index and 41 Luque M, de Rivas B, Alvarez B, Garcia G, Fernandez C, Martell N.
Albustix in assessment of proteinuria. BMJ 1983;287:929 –32 Influence of target organ lesion detection (assessment of
19 Newman DJ, Pugia MJ, Lott JA, Wallace JF, Hiar AM. Urinary protein microalbuminuria and echocardiogram) in cardiovascular risk
and albumin excretion corrected by creatinine and specific gravity. stratification and treatment of untreated hypertensive patients. J Hum
Clin Chim Acta 2000;294:139 –55 Hypertens 2006;20:187 –92
Downloaded from acb.sagepub.com by guest on April 24, 2016
476 Annals of Clinical Biochemistry Volume 46 November 2009
................................................................................................................................................
42 Jensen JS, Clausen P, Borch-Johnsen K, Jensen G, Feldt-Rasmussen B. 47 Schwab SJ, Dunn FL, Feinglos MN. Screening for microalbuminuria.
Detecting microalbuminuria by urinary albumin/creatinine ratio. A comparison of single sample methods of collection and techniques
Nephrol Dial Transplant 1997;12(Suppl. 2):6 –9 of albumin analysis. Diabetes Care 1992;15:1582 –4
43 Jafar TH, Cahturvedi N, Hatcher J, Levey AS. Use of albumin creatinine 48 Atkins RC, Briganti EM, Zimmet PZ, Chadban SJ. Association between
ratio and urine albumin concentration as a screening test for albuminuria albuminuria and proteinuria in the general population: the AusDiab
in an Indo-Asian population. Nephrol Dial Transplant 2007;22:2194 –200 study. Nephrol Dial Transplant 2003;18:2170 –4
44 Nisell H, Trygg M, Bäck R. Urine albumin/creatinine ratio for the 49 Collier G, Greenan MC, Brady JJ, Murray B, Cunningham SK. A study of
assessment of albuminuria in pregnancy hypertension. Acta Obstet the relationship between albuminuria, proteinuria and urinary reagent
Gynecol Scand 2006;85:1327 –30 strips. Ann Clin Biochem 2009;46:247 –9
45 Risberg A, Larsson A, Olsson K, Lyrenäs S, Sjöquist M. relationship 50 Connell SJ, Hollis S, Tieszen KL, McMurray JR, Dornan TL. Gender
between urinary albumin and albumin/creatinine ratio during normal and the clinical usefulness of the albumin:creatinine ratio. Diabet Med
pregnancy and pre-eclampsia. Scand J Clin Lab Invest 2004;64:17– 23 1994;11:32 –6
46 Xin G, Wang M, Jiao LL, Xu GB, Wang HY. Protein-to-creatinine ratio
in spot urine samples as a predictor of quantitation of proteinuria.
Clin Chim Acta 2004;350:35– 9 (Accepted 22 June 2009)
Downloaded from acb.sagepub.com by guest on April 24, 2016
You might also like
- Walgreens Specification of ChargesDocument40 pagesWalgreens Specification of ChargesMichael Cusanelli100% (2)
- Fluid TherapyDocument10 pagesFluid Therapytaner_soysurenNo ratings yet
- HIGH RISK PREGNANCY COMPLICATIONSDocument12 pagesHIGH RISK PREGNANCY COMPLICATIONSggrrk7100% (2)
- Kaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysisDocument9 pagesKaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysispudjoNo ratings yet
- Proteinuria BasicMechanismsPathophys PDFDocument147 pagesProteinuria BasicMechanismsPathophys PDFLedira Dara IsmiNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Antimicrobial Susceptibility Testing PDFDocument19 pagesAntimicrobial Susceptibility Testing PDFdatitoxNo ratings yet
- Newsletter10-1 SebiaDocument4 pagesNewsletter10-1 SebiaNidiam2100% (1)
- Drug StudyDocument13 pagesDrug StudyJaessa Feliciano50% (2)
- Exam - ORDocument4 pagesExam - ORJoel B. SeradNo ratings yet
- 2 Tietz 2012 Kidney Function TestsDocument39 pages2 Tietz 2012 Kidney Function TestsIvana BajunovicNo ratings yet
- Judith Blaine (Eds.) - Proteinuria - Basic Mechanisms, Pathophysiology and Clinical Relevance-Springer International Publishing (2016)Document147 pagesJudith Blaine (Eds.) - Proteinuria - Basic Mechanisms, Pathophysiology and Clinical Relevance-Springer International Publishing (2016)Rubén Casas BenítezNo ratings yet
- United States PharmacopeiaDocument4 pagesUnited States Pharmacopeiagabriel Rosell0% (1)
- Dermoscopy ChallengeDocument2 pagesDermoscopy ChallengegongutzNo ratings yet
- Kl355, KTD (Optha) : Allopathy Post Graduate Doct RsDocument54 pagesKl355, KTD (Optha) : Allopathy Post Graduate Doct RsKirti Raj0% (1)
- 06 Oa Comparison of Spot PDFDocument5 pages06 Oa Comparison of Spot PDFrositaputriagustiniNo ratings yet
- Methven TPCR RDocument6 pagesMethven TPCR RMARIA VICTORIA VELARDE ALIAGANo ratings yet
- Uapcr DiagnosticDocument8 pagesUapcr DiagnosticYA MAAPNo ratings yet
- Primary Care Approach To ProteinuriaDocument6 pagesPrimary Care Approach To Proteinuriadanny17phNo ratings yet
- Random Spot Urine Protein To Creatinine Ratio Is A Reliable Measure of Proteinuria in Lupus Nephritis in KoreansDocument5 pagesRandom Spot Urine Protein To Creatinine Ratio Is A Reliable Measure of Proteinuria in Lupus Nephritis in KoreansRajagopalNo ratings yet
- 10 0000@www Jrheum Org@32@5@828Document5 pages10 0000@www Jrheum Org@32@5@828Yasser AlghrafyNo ratings yet
- Urine Sediment Exam Provides More Diagnostic Information in AKI-1Document4 pagesUrine Sediment Exam Provides More Diagnostic Information in AKI-1Ingrid González EfronNo ratings yet
- Sindrom NefrotikDocument7 pagesSindrom NefrotikDania SaraswatiNo ratings yet
- Clinical Approach To Advanced Renal Function Tes Ting in Dogs and CA TsDocument16 pagesClinical Approach To Advanced Renal Function Tes Ting in Dogs and CA Tsl.fernandagonzalez97No ratings yet
- Guía Lab. 2 BC1Document8 pagesGuía Lab. 2 BC1Cristiana Auxiliadora Fonseca MayorgaNo ratings yet
- Korelasi Kadar Kreatinin Serum Dengan Hasil Tes Albumin Urine Pada Pasien Dengan Penyakit Ginjal Di Rsud Dr. Soegiri LamonganDocument8 pagesKorelasi Kadar Kreatinin Serum Dengan Hasil Tes Albumin Urine Pada Pasien Dengan Penyakit Ginjal Di Rsud Dr. Soegiri LamonganBahrur RoziNo ratings yet
- Urine 24 H ArticleDocument8 pagesUrine 24 H ArticleYousra NanoNo ratings yet
- Jurnal AsyiqueDocument10 pagesJurnal AsyiquepahrirrezaNo ratings yet
- Diagnostic Utility of Protein To Creatinine RatioDocument21 pagesDiagnostic Utility of Protein To Creatinine RatioDinda YenviartiNo ratings yet
- Original Articles_ Comparison of Urinary Albumin-Creatinine Ratio and Albumin Excretion Rate in the Diabetes Control and Complications Trial_Epidemiology of Diabetes Interventions and Complications StudyDocument16 pagesOriginal Articles_ Comparison of Urinary Albumin-Creatinine Ratio and Albumin Excretion Rate in the Diabetes Control and Complications Trial_Epidemiology of Diabetes Interventions and Complications StudyM Dwi SuprayogiNo ratings yet
- CKD Progression and Mortality with Sodium and Potassium ExcretionDocument20 pagesCKD Progression and Mortality with Sodium and Potassium ExcretionAndrie GunawanNo ratings yet
- HematuriaDocument9 pagesHematuriaTel Avid YaredNo ratings yet
- Screening Tool For Proteinuria in Lupus NephritisDocument7 pagesScreening Tool For Proteinuria in Lupus NephritisM Dwi SuprayogiNo ratings yet
- Original Article Assessment of Proteinuria by Using Protein: Creatinine Index in Random Urine SampleDocument4 pagesOriginal Article Assessment of Proteinuria by Using Protein: Creatinine Index in Random Urine SampleTanveerNo ratings yet
- Assessment of The Value of Serum Cholinesterase As A Liver Function Test For Cirrhotic PatientsDocument4 pagesAssessment of The Value of Serum Cholinesterase As A Liver Function Test For Cirrhotic PatientsdrferiNo ratings yet
- Bahan CKD Jurnal ProposalDocument6 pagesBahan CKD Jurnal ProposalArjunaPamungkasNo ratings yet
- JR2 RizaDocument3 pagesJR2 RizaCitra DewiNo ratings yet
- Urologi Jurnal InternasionalDocument9 pagesUrologi Jurnal InternasionalMyisha UfairaNo ratings yet
- Spot Urinary Albumin Creatinine Ratio As A PredictDocument7 pagesSpot Urinary Albumin Creatinine Ratio As A PredictFatimahNo ratings yet
- 5 - Clinical 1Document21 pages5 - Clinical 1levan guluaNo ratings yet
- Changes in Urine Volume and Serum Albumin in Incident Hemodialysis PatientsDocument12 pagesChanges in Urine Volume and Serum Albumin in Incident Hemodialysis Patientsmelda lestari haidirNo ratings yet
- Comprehensive Urinomic Identification of Protein Alternatives To Creatinine Normalization For Diagnostic Assessment of Lupus NephrDocument8 pagesComprehensive Urinomic Identification of Protein Alternatives To Creatinine Normalization For Diagnostic Assessment of Lupus NephrAlberto Carlos Espinosa GaravitoNo ratings yet
- Accuracy of 12-Hour Urine Collection in The Diagnosis of Pre-EclampsiaDocument6 pagesAccuracy of 12-Hour Urine Collection in The Diagnosis of Pre-EclampsiaJeanne d'Arc DyanchanaNo ratings yet
- PIIS0012369216315057Document5 pagesPIIS0012369216315057kk p;No ratings yet
- Sharawey2011 PDFDocument7 pagesSharawey2011 PDFIkram DibNo ratings yet
- Heers Pink StudyDocument6 pagesHeers Pink StudyluchititaNo ratings yet
- Tauk 2015Document7 pagesTauk 2015Andres Vásquez ChNo ratings yet
- Acute Kidney InjuryDocument10 pagesAcute Kidney InjuryFransiskus A Danu KrisbiantoroNo ratings yet
- El Examen de Sedimento de Orina Proporciona Más Información Diagnóstica en AKI Que Biomarcadores. 2022Document3 pagesEl Examen de Sedimento de Orina Proporciona Más Información Diagnóstica en AKI Que Biomarcadores. 2022Edwin Fabian Paz UrbanoNo ratings yet
- Useful TestsDocument3 pagesUseful TestsLiamNo ratings yet
- Proteinuria Pada Anak AnakDocument7 pagesProteinuria Pada Anak Anaklathifa nabilaNo ratings yet
- CC CC C C C!"#C $!$%: C$!$C c!"7 ":"!CDocument45 pagesCC CC C C C!"#C $!$%: C$!$C c!"7 ":"!CMukhtar JamacNo ratings yet
- Predicting Microalbuminuria Using Urine Protein-Creatinine RatioDocument6 pagesPredicting Microalbuminuria Using Urine Protein-Creatinine RatiosoniNo ratings yet
- Bilirrubina en Liq OrgánicoDocument6 pagesBilirrubina en Liq OrgánicoCindy Yunuen LeónNo ratings yet
- Validation of A Glucose Meter at An Intensive Care UnitDocument7 pagesValidation of A Glucose Meter at An Intensive Care UnitRodas GetachewNo ratings yet
- Jvim 29 028Document7 pagesJvim 29 028Marilyn Patricia Abello GarciaNo ratings yet
- Simplified Algorithm For Evaluation of Proteinuria in Clinical Practice: How Should A Clinician Approach?Document5 pagesSimplified Algorithm For Evaluation of Proteinuria in Clinical Practice: How Should A Clinician Approach?Danny JacobusNo ratings yet
- Week 6 Facilitator Copy Week 06 Renal Failure PDFDocument7 pagesWeek 6 Facilitator Copy Week 06 Renal Failure PDFoxyc0n999No ratings yet
- Hematuria em AdultosDocument10 pagesHematuria em AdultosalexandrecpcNo ratings yet
- Assesmentof Fibro Q Test, AAR & APRI Indices As Markers of Fibrosis in Chronic Liver DiseaseDocument5 pagesAssesmentof Fibro Q Test, AAR & APRI Indices As Markers of Fibrosis in Chronic Liver Diseaseferdinan goutamaNo ratings yet
- Sedimento RBC DismorficCellDocument7 pagesSedimento RBC DismorficCellecko RomanNo ratings yet
- Haemostatic Abnormalities in Patients With Cirrhosis and Their Relation With Severity of Liver Dysfunction As Assessed by Child Pugh ScoreDocument6 pagesHaemostatic Abnormalities in Patients With Cirrhosis and Their Relation With Severity of Liver Dysfunction As Assessed by Child Pugh ScoreWahyu PerdakaNo ratings yet
- Circadian Rhythms of Diuresis, Proteinuria and Natriuresis in Children With Chronic Glomerular DiseaseDocument9 pagesCircadian Rhythms of Diuresis, Proteinuria and Natriuresis in Children With Chronic Glomerular DiseaseAulia Arief RhdNo ratings yet
- Com Per 2005Document7 pagesCom Per 2005Rina ErlinaNo ratings yet
- 1-s2.0-S0039914020310092-mainDocument20 pages1-s2.0-S0039914020310092-mainBen DresimNo ratings yet
- Intervalo de Referencia Urine 24 Hours 2015 CaucasicoDocument13 pagesIntervalo de Referencia Urine 24 Hours 2015 CaucasicoGregorio De Las CasasNo ratings yet
- KidneyDocument1 pageKidneySujith KuttanNo ratings yet
- Urinalysis Interpretation and Clinical CorrelationsDocument21 pagesUrinalysis Interpretation and Clinical CorrelationsFercho MedNo ratings yet
- Index 2018 The-BreastDocument34 pagesIndex 2018 The-BreastkeyssiNo ratings yet
- Acute Abdominal Pain in Older Patients PDFDocument8 pagesAcute Abdominal Pain in Older Patients PDFleesaNo ratings yet
- Guia Ingles Ginebra Violacion SexualDocument154 pagesGuia Ingles Ginebra Violacion SexualkeyssiNo ratings yet
- Articulo Himen Complaciente IranDocument4 pagesArticulo Himen Complaciente IrankeyssiNo ratings yet
- Articulo Himen Complaciente IranDocument4 pagesArticulo Himen Complaciente IrankeyssiNo ratings yet
- Boala Binswanger PDFDocument12 pagesBoala Binswanger PDFDrHellenNo ratings yet
- History of TriageDocument12 pagesHistory of Triageyuni purwatiNo ratings yet
- Download Kaplan USMLE STEP 1 Notes and High Yield Medical Study MaterialsDocument9 pagesDownload Kaplan USMLE STEP 1 Notes and High Yield Medical Study MaterialsdtilaniNo ratings yet
- Rheumatic FeverDocument3 pagesRheumatic FeverKennette LimNo ratings yet
- Materi DR. Dr. Ery Olivianto, Sp.A (K)Document39 pagesMateri DR. Dr. Ery Olivianto, Sp.A (K)utamiprakosoNo ratings yet
- Share SPM Problems With AnswerDocument54 pagesShare SPM Problems With AnswersanthoshNo ratings yet
- Capstone Case F 4Document6 pagesCapstone Case F 4Ameer HamzaNo ratings yet
- PRC Form - orDocument5 pagesPRC Form - orJeaneline Pagasian EnonNo ratings yet
- Health System Building Blocks and Organ.2Document4 pagesHealth System Building Blocks and Organ.2Advait RajagopalNo ratings yet
- TheSun 2009-11-02 Page01 Painkiller Abuse AlertDocument1 pageTheSun 2009-11-02 Page01 Painkiller Abuse AlertImpulsive collectorNo ratings yet
- ART Rules March, 2022-1 PDFDocument96 pagesART Rules March, 2022-1 PDFsasankNo ratings yet
- LAB - 017 Injections - Subcutaneous (SC) Injection in Mice and RatsDocument6 pagesLAB - 017 Injections - Subcutaneous (SC) Injection in Mice and RatsGlorious LibertyNo ratings yet
- Procedure Checklist Chapter 23: Using A Volume-Control Administration Set (E.g., Buretrol, Volutrol, Soluset)Document2 pagesProcedure Checklist Chapter 23: Using A Volume-Control Administration Set (E.g., Buretrol, Volutrol, Soluset)jthsNo ratings yet
- Zincum ArsenicosumDocument8 pagesZincum ArsenicosumKamalNo ratings yet
- Rosenhan - Contextual Nature of Psychiatric DiagnosisDocument13 pagesRosenhan - Contextual Nature of Psychiatric Diagnosisvoidr66100% (2)
- 35Document174 pages35sggdgdNo ratings yet
- PENANG MEDICAL COLLEGE Critical Appraisal TherapyDocument3 pagesPENANG MEDICAL COLLEGE Critical Appraisal TherapyRebecca WongNo ratings yet
- Epidemic and Pandemic Differences Additional InformationDocument4 pagesEpidemic and Pandemic Differences Additional InformationPsyZeroNo ratings yet
- I. General Primary Health Care Facility Design Information: Research RequirementsDocument24 pagesI. General Primary Health Care Facility Design Information: Research RequirementsJoyce LapuzNo ratings yet
- Zirconnia Knife Edge PDFDocument6 pagesZirconnia Knife Edge PDFMuaiyed Buzayan AkremyNo ratings yet
- Psychogenic Pain and Aggression: The Syndrome of The Solitary HunterDocument11 pagesPsychogenic Pain and Aggression: The Syndrome of The Solitary HunterHikmat SatriaNo ratings yet