You might also like
- CPG On Chronic CoughDocument93 pagesCPG On Chronic Coughgail100% (2)
- Practice Writing Effective SentencesDocument5 pagesPractice Writing Effective SentencesHaekal FarabyNo ratings yet
- Deep Neck Space Infections in Children: Has Anything Changed?Document6 pagesDeep Neck Space Infections in Children: Has Anything Changed?Muhammad Dody HermawanNo ratings yet
- A Guide To The Management of Acute Rhinosinusitis in Primary CareDocument4 pagesA Guide To The Management of Acute Rhinosinusitis in Primary CarecubillahhNo ratings yet
- Acute and Chronic Rhinosinusitis in Adults PSO-HNS 2016Document12 pagesAcute and Chronic Rhinosinusitis in Adults PSO-HNS 2016Angela TakedaNo ratings yet
- Article 2.2Document9 pagesArticle 2.2jessika yanceNo ratings yet
- Medical Management Strategies in Acute and Chronic RhinosinusitisDocument6 pagesMedical Management Strategies in Acute and Chronic RhinosinusitisIhdinal MuktiNo ratings yet
- Rheumatic Fever and Rheumatic Heart Disease: PediatricsDocument8 pagesRheumatic Fever and Rheumatic Heart Disease: PediatricsRea Dominique CabanillaNo ratings yet
- Management of Nasal Polyposis: C. Bachert, T. RobillardDocument10 pagesManagement of Nasal Polyposis: C. Bachert, T. RobillardAnonymous il1cFm6No ratings yet
- ARTÍCULO GlaucomaDocument9 pagesARTÍCULO GlaucomalissalfonsiaNo ratings yet
- Inhaled Corticosteroids and Voice Problems. What Is New - PDFDocument7 pagesInhaled Corticosteroids and Voice Problems. What Is New - PDFDaniel Celestino DiazNo ratings yet
- Correspondence: Smell and Taste Dysfunction in Patients With COVID-19Document1 pageCorrespondence: Smell and Taste Dysfunction in Patients With COVID-19Dhyo Asy-shidiq HasNo ratings yet
- Intranasal Diprospan Injection For Chronic Rhinosinusitis Treatmenttwo Case Reports 2472 016X 1000109 PDFDocument5 pagesIntranasal Diprospan Injection For Chronic Rhinosinusitis Treatmenttwo Case Reports 2472 016X 1000109 PDFDiandraRezkyMaharaniNo ratings yet
- Recurrent Respiratory Papillomatosis: Case ReportDocument6 pagesRecurrent Respiratory Papillomatosis: Case ReportPradhana FwNo ratings yet
- 571 FullDocument2 pages571 FullJauhari JoNo ratings yet
- Cough: Neurophysiology, Methods of Research, Pharmacological Therapy and PhonoaudiologyDocument10 pagesCough: Neurophysiology, Methods of Research, Pharmacological Therapy and Phonoaudiologynadya shifaNo ratings yet
- Sore Throat: Navigating The Differential DiagnosisDocument7 pagesSore Throat: Navigating The Differential DiagnosisCaity YoungNo ratings yet
- Effects of COVID-19 LockdownDocument6 pagesEffects of COVID-19 LockdownMuhammad GilangNo ratings yet
- Disfunções Tratamentos OncológicosDocument7 pagesDisfunções Tratamentos Oncológicosbarbaraduarte0803No ratings yet
- Acute Isolated Sphenoid Sinusitis in Children - 2021 - International Journal ofDocument8 pagesAcute Isolated Sphenoid Sinusitis in Children - 2021 - International Journal ofHung Son TaNo ratings yet
- Sol Hipert en SibilanciasDocument9 pagesSol Hipert en Sibilanciasedith sandovalNo ratings yet
- 9009 44225 1 PB PDFDocument5 pages9009 44225 1 PB PDFwandajunitasNo ratings yet
- Clinicopathological Study of Change of Voice: ST THDocument10 pagesClinicopathological Study of Change of Voice: ST THAshokNo ratings yet
- Serous Otitis Media Clinical and Therapeutic ConsiDocument5 pagesSerous Otitis Media Clinical and Therapeutic Consiheidi leeNo ratings yet
- Retropharyngeal AbscessDocument3 pagesRetropharyngeal AbscessDwi Utari PratiwiNo ratings yet
- A Child With Complicated Diphtheria in This Vaccine Era: A Case ReportDocument2 pagesA Child With Complicated Diphtheria in This Vaccine Era: A Case Reportummu yayaNo ratings yet
- 1 IiomainDocument6 pages1 IiomainyandaputriNo ratings yet
- E20161309 FullDocument12 pagesE20161309 Fullwajarsi pratamiNo ratings yet
- Down Syndrome: Otolaryngological Effects of Rapid Maxillary ExpansionDocument7 pagesDown Syndrome: Otolaryngological Effects of Rapid Maxillary ExpansionDavid AndradeNo ratings yet
- Jurnal 3Document6 pagesJurnal 3Dheana IsmaniarNo ratings yet
- JMD 3 2 32 2Document7 pagesJMD 3 2 32 2JEREMIE FAYE UMALINo ratings yet
- Osa OrthopaedicsDocument13 pagesOsa OrthopaedicsJustin KimberlakeNo ratings yet
- Hospitalisations Due To Respiratory Syncytial Virus Infection inDocument8 pagesHospitalisations Due To Respiratory Syncytial Virus Infection innelcitojuniorNo ratings yet
- Hypoxemia in Children With Pneumonia and Its Clinical PredictorsDocument6 pagesHypoxemia in Children With Pneumonia and Its Clinical Predictorsamalia chairunnisaNo ratings yet
- Menière's DiseaseDocument21 pagesMenière's DiseaseFelipeAsenjoÁlvarezNo ratings yet
- Uia30 Anaesthesia For Paediatric Ear Nose and Throat SurgeryDocument6 pagesUia30 Anaesthesia For Paediatric Ear Nose and Throat SurgeryAshokNo ratings yet
- Fluticasone Propionate Aqueous Nasal Spray in The Treatment of Nasal PolyposisDocument7 pagesFluticasone Propionate Aqueous Nasal Spray in The Treatment of Nasal PolyposisAnonymous 5K38SwLNo ratings yet
- Voice Therapy in MTD CasesDocument5 pagesVoice Therapy in MTD Casesmerry christyNo ratings yet
- Herpes Zoster Oticus in A 12 Year Old Child and Review of Literature - A CaseDocument5 pagesHerpes Zoster Oticus in A 12 Year Old Child and Review of Literature - A CaseClodeyaRizolaNo ratings yet
- Pi Is 1875957213001903Document5 pagesPi Is 1875957213001903eppy syafriNo ratings yet
- Original Articles Efficacy and Safety of Mometasone Furoate Nasal Spray in Nasal PolyposisDocument7 pagesOriginal Articles Efficacy and Safety of Mometasone Furoate Nasal Spray in Nasal PolyposisCheah Chong ShengNo ratings yet
- 1 s2.0 S030095722200538X MainDocument1 page1 s2.0 S030095722200538X MainDana MateiNo ratings yet
- Adenoid Hypertrophy FixDocument7 pagesAdenoid Hypertrophy FixWidi Yuli HariantoNo ratings yet
- Stroboscopy For Benign Laryngeal Pathology in Evidence Based Health CareDocument5 pagesStroboscopy For Benign Laryngeal Pathology in Evidence Based Health CareDoina RusuNo ratings yet
- IJORL Volume 26 Issue 4 Pages 245-249Document5 pagesIJORL Volume 26 Issue 4 Pages 245-249adrianussetNo ratings yet
- Ana 29 492Document6 pagesAna 29 492AdilZyaniNo ratings yet
- Assessment of Intranasal Steroid Effect in Management of Adenoid Hypertrophy in Children Between 2-11 Years OldDocument7 pagesAssessment of Intranasal Steroid Effect in Management of Adenoid Hypertrophy in Children Between 2-11 Years OldSabrina JonesNo ratings yet
- Case Study - Macarambon, FDDocument5 pagesCase Study - Macarambon, FDUmar MacarambonNo ratings yet
- Laryngeal TuberculosisDocument5 pagesLaryngeal TuberculosisastralmaniaNo ratings yet
- Pediatric Laryngopharyngeal Reflux, Perceptual, Acoustic, and Laryngeal T FindingsDocument5 pagesPediatric Laryngopharyngeal Reflux, Perceptual, Acoustic, and Laryngeal T Findingsarif sudianto100% (1)
- PAPER (ENG) - The Presentation and Management of Laryngeal Cleft - A 10 Years ExperienceDocument7 pagesPAPER (ENG) - The Presentation and Management of Laryngeal Cleft - A 10 Years ExperienceAldo Hip NaranjoNo ratings yet
- Cherian Et Al, 2012Document5 pagesCherian Et Al, 2012julianasanjayaNo ratings yet
- 3121-9289-1-SM MutiaDocument9 pages3121-9289-1-SM MutiaTrhey Ahmilza DamaitaNo ratings yet
- Disfuncion de Cuedas VocalesDocument6 pagesDisfuncion de Cuedas VocalesJan SaldañaNo ratings yet
- 1 s2.0 S180886941530745X MainDocument5 pages1 s2.0 S180886941530745X MainChinciaNo ratings yet
- Snijders 2007Document6 pagesSnijders 2007carlaNo ratings yet
- Chronic Rhinosinusitis AbsDocument1 pageChronic Rhinosinusitis AbszainabNo ratings yet
- Acute Primary Herpetic Gingivostomatitis: Ravi Prakash Sasankoti Mohan, Sankalp Verma, Udita Singh, Neha AgarwalDocument3 pagesAcute Primary Herpetic Gingivostomatitis: Ravi Prakash Sasankoti Mohan, Sankalp Verma, Udita Singh, Neha AgarwalBrili AnenoNo ratings yet
- Allergic Nasal PolypsDocument6 pagesAllergic Nasal PolypsMirza Khizar HameedNo ratings yet
- NVBNDocument7 pagesNVBNAnonymous 5K38SwLNo ratings yet
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaFrom EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaNo ratings yet
- J-20 Stealth Fighter Design Balances Speed and Agility - Defense Content From Aviation WeekDocument9 pagesJ-20 Stealth Fighter Design Balances Speed and Agility - Defense Content From Aviation WeekMahesNo ratings yet
- Mono and DicotDocument3 pagesMono and Dicotlady chaseNo ratings yet
- Appendix 2-4.ep31422 - g-16Document15 pagesAppendix 2-4.ep31422 - g-16bsnegi111No ratings yet
- Unit P1, P1.1: The Transfer of Energy by Heating ProcessesDocument9 pagesUnit P1, P1.1: The Transfer of Energy by Heating ProcessesTemilola OwolabiNo ratings yet
- Lighting Movements-The Fox On The FairwayDocument1 pageLighting Movements-The Fox On The FairwayabneypaigeNo ratings yet
- ACE Inhibitors Vs ARBsDocument3 pagesACE Inhibitors Vs ARBsKo Phyo WaiNo ratings yet
- BotanyDocument11 pagesBotanyGirish GuptaNo ratings yet
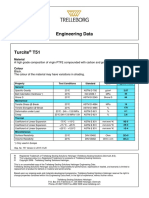
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Class XL (The Portrait of A Lady)Document7 pagesClass XL (The Portrait of A Lady)tmoNo ratings yet
- Animal 1414Document6 pagesAnimal 1414trialink minsanNo ratings yet
- Graha YuddhaDocument10 pagesGraha YuddhaHeather WilliamsNo ratings yet
- TrerwtsdsDocument167 pagesTrerwtsdsvinicius gomes duarteNo ratings yet
- Embryo AssignmentDocument2 pagesEmbryo AssignmentA.j. MasagcaNo ratings yet
- How To Write A Research Paper With Parenthetical DocumentationDocument5 pagesHow To Write A Research Paper With Parenthetical Documentationc9spy2qzNo ratings yet
- BITEBUDZ COMPANY EME Kemerut 1Document31 pagesBITEBUDZ COMPANY EME Kemerut 1Mark LightNo ratings yet
- Riparian Flora of Kaliwa River Watershed in The Sierra Madre Mountain Range, PhilippinesDocument12 pagesRiparian Flora of Kaliwa River Watershed in The Sierra Madre Mountain Range, PhilippinesMichael Angelo ValdezNo ratings yet
- Research PaperDocument2 pagesResearch PaperCyril FragataNo ratings yet
- Recognizing and Classifying Daily Human Activities: Group-22Document23 pagesRecognizing and Classifying Daily Human Activities: Group-22Divyam GuptaNo ratings yet
- Indigenous Resources ActivitiesDocument17 pagesIndigenous Resources Activitiesscribbler49971100% (1)
- KIN LONG Shower Screen CatalogueDocument58 pagesKIN LONG Shower Screen CatalogueFaiz ZentNo ratings yet
- CardiomyopathyDocument1 pageCardiomyopathyTrisha VergaraNo ratings yet
- Catchment CharacterisationDocument48 pagesCatchment CharacterisationSherlock BaileyNo ratings yet
- The National TerritoryDocument39 pagesThe National TerritoryRan RanNo ratings yet
- 413 1684 1 PB PDFDocument5 pages413 1684 1 PB PDFMhd RidwanNo ratings yet
- JBL Constant Beamwidth Technology - CBT Series Passive Controlled-Coverage ColumnsDocument12 pagesJBL Constant Beamwidth Technology - CBT Series Passive Controlled-Coverage ColumnsTom HampleNo ratings yet
- Ecs C42iix Rev C Vit m2400 1Document36 pagesEcs C42iix Rev C Vit m2400 1Victor Pic100% (1)
- Reglas Digitales Mitutoyo Scale Units Linear ScalesDocument31 pagesReglas Digitales Mitutoyo Scale Units Linear ScalesAngelmambrinNo ratings yet
- AnorexiaDocument1 pageAnorexiaCHIEF DOCTOR MUTHUNo ratings yet