You might also like
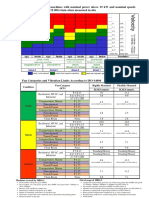
- Limit Table According To ISO (10816-3 and 14694)Document1 pageLimit Table According To ISO (10816-3 and 14694)Muhammad Haroon67% (3)
- Articulo Pedia en InglesDocument10 pagesArticulo Pedia en InglesMónica NatalyNo ratings yet
- UntitledDocument13 pagesUntitledscott janeNo ratings yet
- Food Safety Attitude and Associated Factors AmongDocument6 pagesFood Safety Attitude and Associated Factors AmongEmmanuelNo ratings yet
- GeographicallocationDocument6 pagesGeographicallocationسوسو توتوNo ratings yet
- Effect of Health Education Program For Mothers of Children With Enterobius Vermicularis at Assiut University Children HospitalDocument30 pagesEffect of Health Education Program For Mothers of Children With Enterobius Vermicularis at Assiut University Children HospitalancillaagraynNo ratings yet
- A Multilevel Analysis of Factors Associated With Childhood Diarrhea in EthiopiaDocument10 pagesA Multilevel Analysis of Factors Associated With Childhood Diarrhea in Ethiopianoventina7marbunNo ratings yet
- 3158-Article Text-10989-12848-10-20231026Document6 pages3158-Article Text-10989-12848-10-20231026nadiyah kamiliaNo ratings yet
- Asian Paci Fic Journal of Tropical BiomedicineDocument5 pagesAsian Paci Fic Journal of Tropical BiomedicineYosia KevinNo ratings yet
- BMC Public Health: Intestinal Parasites Prevalence and Related Factors in School Children, A Western City Sample-TurkeyDocument6 pagesBMC Public Health: Intestinal Parasites Prevalence and Related Factors in School Children, A Western City Sample-TurkeyVelazquez Rico Cinthya MontserrathNo ratings yet
- Maternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoDocument20 pagesMaternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoAnisa SafutriNo ratings yet
- 2020-RS-Epidemiology of Intestinal ParasiticDocument16 pages2020-RS-Epidemiology of Intestinal ParasiticmoramdNo ratings yet
- Prevalence of Premature Rupture of Membrane and Its Associated Factors Among Pregnant Women in Ethiopia: A Systematic Review and Meta-AnalysisDocument9 pagesPrevalence of Premature Rupture of Membrane and Its Associated Factors Among Pregnant Women in Ethiopia: A Systematic Review and Meta-AnalysisCitrast NursyahidahNo ratings yet
- PDFDocument10 pagesPDFDagnew YehualaNo ratings yet
- Worm InfestationDocument1 pageWorm InfestationMRS CHAKRAPANINo ratings yet
- Causal Relationship Between Environmental Enteric Dysfunction - 2022 - ScientifDocument8 pagesCausal Relationship Between Environmental Enteric Dysfunction - 2022 - ScientifCawee CawNo ratings yet
- Survival and Associated Factors of Mortality of Preterm Neonates Admitted To FHSHDocument8 pagesSurvival and Associated Factors of Mortality of Preterm Neonates Admitted To FHSHAyanawNo ratings yet
- Knowledge, Attitude and Practices of School Children On Prevention and Control of Superficial Fungal in Western KenyaDocument7 pagesKnowledge, Attitude and Practices of School Children On Prevention and Control of Superficial Fungal in Western KenyaPremier PublishersNo ratings yet
- RRTM 327129 Isolation of Escherichia Coli and Its Associated Risk FactorDocument8 pagesRRTM 327129 Isolation of Escherichia Coli and Its Associated Risk FactorAssefa AlemuNo ratings yet
- 1 s2.0 S2213398422000392 MainDocument9 pages1 s2.0 S2213398422000392 MainMoad RuzkiNo ratings yet
- 10 1177@1059840518785447Document11 pages10 1177@1059840518785447dindasaviraNo ratings yet
- 1 s2.0 S2666149722000202 MainDocument6 pages1 s2.0 S2666149722000202 MainALEXANDRE SOUSANo ratings yet
- Assessment of Hand Washing Practice andDocument6 pagesAssessment of Hand Washing Practice andAbdirahman Yusuf AliNo ratings yet
- Prevalence and Factors Associated With Intestinal Parasites Among Children of Age 6 To 59 Months In, Boricha District, South Ethiopia, in 2018Document7 pagesPrevalence and Factors Associated With Intestinal Parasites Among Children of Age 6 To 59 Months In, Boricha District, South Ethiopia, in 2018Mirtha AnggraeniNo ratings yet
- Married Women's Decision-Making Autonomy On Contraceptive Use and Its Associated Factors in Ethiopia: A Multilevel Analysis of 2016 Demographic and Health SurveyDocument14 pagesMarried Women's Decision-Making Autonomy On Contraceptive Use and Its Associated Factors in Ethiopia: A Multilevel Analysis of 2016 Demographic and Health SurveyKusse UrmaleNo ratings yet
- Diaper RashDocument9 pagesDiaper RashVincentius Michael WilliantoNo ratings yet
- Structured Assessment, Evaluation and MonitoringDocument7 pagesStructured Assessment, Evaluation and Monitoringrandy gallegoNo ratings yet
- Magnitude and Associated Factors of Respectful Maternity Care in Tirunesh Beijing Hospital, Addis Ababa, Ethiopia, 2021Document8 pagesMagnitude and Associated Factors of Respectful Maternity Care in Tirunesh Beijing Hospital, Addis Ababa, Ethiopia, 2021Amare MisganawNo ratings yet
- Preliminary Survey of Schoolbased Water Sanitation Hygiene in Public Schools Odeda Ogun State PDFDocument10 pagesPreliminary Survey of Schoolbased Water Sanitation Hygiene in Public Schools Odeda Ogun State PDFPelumiNo ratings yet
- The Relationship Between Mothers' Knowledge and Practice Level of Cough Etiquette and Their Children's Practice Level in South KoreaDocument10 pagesThe Relationship Between Mothers' Knowledge and Practice Level of Cough Etiquette and Their Children's Practice Level in South KoreaDicky CaritoNo ratings yet
- Tu 2022Document12 pagesTu 2022Elías Enrique MartínezNo ratings yet
- Water, Sanitation Dan Hygiene Analysis, and Individual Factors For Stunting Among Children Under Two Years in AmbonDocument5 pagesWater, Sanitation Dan Hygiene Analysis, and Individual Factors For Stunting Among Children Under Two Years in AmbonDaniya BisaraNo ratings yet
- Prevalence of Intestinal Helminthic Infections and Malnutrition Among Schoolchildren of The Zegie Peninsula, Northwestern EthiopiaDocument9 pagesPrevalence of Intestinal Helminthic Infections and Malnutrition Among Schoolchildren of The Zegie Peninsula, Northwestern EthiopiaFajar RokhmanitaNo ratings yet
- Association Between Environmental Factors and Incidence of Diarrhea Among Toddlers in The Working Area of Ambal I Health Center, Kebumen, Center of Java, IndonesiaDocument9 pagesAssociation Between Environmental Factors and Incidence of Diarrhea Among Toddlers in The Working Area of Ambal I Health Center, Kebumen, Center of Java, IndonesiaIJELS Research JournalNo ratings yet
- The Egyptian Journal of Medical Human Genetics: Alaa Youssef Ahmed, Amany Mohammed SayedDocument4 pagesThe Egyptian Journal of Medical Human Genetics: Alaa Youssef Ahmed, Amany Mohammed SayedJuanokNo ratings yet
- Scabies Among Children in EthiopiaDocument9 pagesScabies Among Children in EthiopiaIJPHSNo ratings yet
- Acute Malnutrition PDFDocument10 pagesAcute Malnutrition PDFDamesa MiesaNo ratings yet
- GJESM - Volume 10 - Issue 2 - Pages 589-604Document16 pagesGJESM - Volume 10 - Issue 2 - Pages 589-604Fikran Ahmad Ahmad Al-HadiNo ratings yet
- Predictors of StuntingDocument12 pagesPredictors of Stuntingrezky_tdNo ratings yet
- A School Based Cross Sectional Survey ofDocument5 pagesA School Based Cross Sectional Survey ofPaul JohnsonNo ratings yet
- 2021 - Maria - Predictors of Infection in Children With Systemic Lupus Erythematosus - A Single Center Study in IndonesiaDocument9 pages2021 - Maria - Predictors of Infection in Children With Systemic Lupus Erythematosus - A Single Center Study in IndonesiaLily ChandraNo ratings yet
- Artikel Afipah HumairaDocument11 pagesArtikel Afipah HumairaReski 04No ratings yet
- Assessment of Water, Sanitation and Nutrition Factors Associated With Diarrhea Among ChildrenDocument9 pagesAssessment of Water, Sanitation and Nutrition Factors Associated With Diarrhea Among ChildrenKIU PUBLICATION AND EXTENSIONNo ratings yet
- Pengaruh Asam Sitrat Pada Stres Oksidatif Yang Diinduksi Oleh LPS Peroksidasi LipidDocument5 pagesPengaruh Asam Sitrat Pada Stres Oksidatif Yang Diinduksi Oleh LPS Peroksidasi LipidnidaatsNo ratings yet
- Manuskrip Bahasa Inggris Hubungan Perilaku 3M Plus Terhadap Keberadaan Jentik Nyamuk Aedes Aegypti Di Kecamatan Medan Denai PDFDocument7 pagesManuskrip Bahasa Inggris Hubungan Perilaku 3M Plus Terhadap Keberadaan Jentik Nyamuk Aedes Aegypti Di Kecamatan Medan Denai PDFReza RestuNo ratings yet
- Original Research ArticleDocument5 pagesOriginal Research ArticleNouraNo ratings yet
- Pregnant Women in West GojjamDocument10 pagesPregnant Women in West Gojjambluish oceanNo ratings yet
- Template Jurnal Kesehatan PrimerDocument7 pagesTemplate Jurnal Kesehatan PrimerSyafrisar Meri AgritubellaNo ratings yet
- Effect of Health Teaching On Knowledge and Practice of Postnatal Mother Admitted in Selected Hospital Regarding Using Diaper in Children To Prevent Systemic Bacterial InfectionDocument7 pagesEffect of Health Teaching On Knowledge and Practice of Postnatal Mother Admitted in Selected Hospital Regarding Using Diaper in Children To Prevent Systemic Bacterial InfectionLovely SarangiNo ratings yet
- Soil Transmitted Helminths Prevalence, Perception and Determinants Among Primary School Children in Rural Enugu State, NigeriaDocument12 pagesSoil Transmitted Helminths Prevalence, Perception and Determinants Among Primary School Children in Rural Enugu State, Nigeriaelias aniwadaNo ratings yet
- Research Article Food and Personal Hygiene Perceptions and Practices Among Caregivers Whose Children Have Diarrhea: A Qualitative Study of Urban Mothers in Tangerang, IndonesiaDocument8 pagesResearch Article Food and Personal Hygiene Perceptions and Practices Among Caregivers Whose Children Have Diarrhea: A Qualitative Study of Urban Mothers in Tangerang, IndonesiaAndi UmmahNo ratings yet
- Artikel 4Document6 pagesArtikel 4Claudia BuheliNo ratings yet
- CrossmDocument14 pagesCrossmIra DwijayantiNo ratings yet
- Received: 17/4/19 Accepted: 13/6/19Document5 pagesReceived: 17/4/19 Accepted: 13/6/19UMYU Journal of Microbiology Research (UJMR)No ratings yet
- The Problem and Its Scope: Liceo de Cagayan University College of Medical Laboratory ScienceDocument53 pagesThe Problem and Its Scope: Liceo de Cagayan University College of Medical Laboratory SciencecyrelleNo ratings yet
- 6th International Conference On Tropical Medicine AbstractDocument1 page6th International Conference On Tropical Medicine AbstractMegbaruNo ratings yet
- The Problem and Its Scope: Liceo de Cagayan University College of Medical Laboratory ScienceDocument51 pagesThe Problem and Its Scope: Liceo de Cagayan University College of Medical Laboratory SciencecyrelleNo ratings yet
- Epidemiology and Determinants of Soil-Transmitted Helminthiases Among Selected Primary School Children in Tuguegarao City, Cagayan, Philippines: A Cross-Sectional StudyDocument4 pagesEpidemiology and Determinants of Soil-Transmitted Helminthiases Among Selected Primary School Children in Tuguegarao City, Cagayan, Philippines: A Cross-Sectional StudyIJEAB JournalNo ratings yet
- Research Article A Study of The Prevalence of Giardiasis in Children of The Kindergartens of Islam Abad Gharb City, IranDocument4 pagesResearch Article A Study of The Prevalence of Giardiasis in Children of The Kindergartens of Islam Abad Gharb City, IranFarmasiNo ratings yet
- Case ControlDocument13 pagesCase ControlririsNo ratings yet
- Acne: Current Concepts and ManagementFrom EverandAcne: Current Concepts and ManagementDae Hun SuhNo ratings yet
- Basic Safety Rules in Hindi - Chemistry - NatureDocument6 pagesBasic Safety Rules in Hindi - Chemistry - NatureNikesh Sati100% (1)
- AVP - Distillation Solved ProblemsDocument47 pagesAVP - Distillation Solved ProblemsUdop Charles100% (1)
- Biology 10th Edition Solomon Solutions ManualDocument5 pagesBiology 10th Edition Solomon Solutions Manualspawnerminutiaxae7n100% (35)
- CBT For Acne Comment IJD 2013Document2 pagesCBT For Acne Comment IJD 2013Ionelia PașaNo ratings yet
- Pak KurDocument6 pagesPak KurLoly SeptyanNo ratings yet
- Risk Benefit AnalysisDocument12 pagesRisk Benefit AnalysisAdinaMilitaruNo ratings yet
- Mandril MMGDocument2 pagesMandril MMGlilivaca28No ratings yet
- Mira ExcelDocument48 pagesMira ExcelColin KingNo ratings yet
- Cis 229e Fuji FrontierDocument10 pagesCis 229e Fuji FrontierMILAN709No ratings yet
- E345Document5 pagesE345Juan Enrique Garcia JimenezNo ratings yet
- Aip Cy 2021 WordDocument6 pagesAip Cy 2021 Wordignatius romero100% (2)
- Oxy IQ OxigenoDocument70 pagesOxy IQ OxigenoDavidNo ratings yet
- Aurora@deped Gov PHDocument7 pagesAurora@deped Gov PHGibbs Quizana BaldonadeNo ratings yet
- AttahiruDocument28 pagesAttahiruAdamu Umar100% (1)
- Per Capita Budget For Meal Provision of Patients2 PDFDocument30 pagesPer Capita Budget For Meal Provision of Patients2 PDFMara Benzon-BarrientosNo ratings yet
- Safe and Legal Abortion Is A Womans Human RightDocument8 pagesSafe and Legal Abortion Is A Womans Human Rightan nNo ratings yet
- Markowitz ModelDocument11 pagesMarkowitz ModelAmit GuptaNo ratings yet
- Consumer Protection Act For Medical Profession in IndiaDocument70 pagesConsumer Protection Act For Medical Profession in IndiaAsmi MohamedNo ratings yet
- Fastenal - Mechanical Properties of Inch FastenersDocument4 pagesFastenal - Mechanical Properties of Inch FastenersbclarkeoobNo ratings yet
- BMP - Other Welding ProcessesDocument76 pagesBMP - Other Welding Processessujay nayakNo ratings yet
- Corrosion Analysis of Mild Steel: Supervisor: DR Abdul Wadood Presented By: Saba Sohail (19) & Ahsan Abdul RaufDocument30 pagesCorrosion Analysis of Mild Steel: Supervisor: DR Abdul Wadood Presented By: Saba Sohail (19) & Ahsan Abdul RaufSaba SohailNo ratings yet
- Course Content (CPE 104) : Lesson 1Document4 pagesCourse Content (CPE 104) : Lesson 1eL LeahNo ratings yet
- Citrus Lemon Juice Manufacturing Unit DPR by IIFPTDocument35 pagesCitrus Lemon Juice Manufacturing Unit DPR by IIFPThamza chaabaniNo ratings yet
- Class 9 - Science - MCQDocument116 pagesClass 9 - Science - MCQs.karthick5583No ratings yet
- Site Appraisal Form: Ministry of Basic, Higher and Technical EducationDocument3 pagesSite Appraisal Form: Ministry of Basic, Higher and Technical EducationJohaima HaronNo ratings yet
- Republic Act No. 9262: Anti-Violence Against Women and Their Children ACT OF 2004Document35 pagesRepublic Act No. 9262: Anti-Violence Against Women and Their Children ACT OF 2004Lucky Alonzo100% (1)
- Solar Radiation, Heat Balance and Temperature Chapter 8 - Class 11 Geography NCERT - Class Notes - Samagra Book Series Batch (Hinglish)Document30 pagesSolar Radiation, Heat Balance and Temperature Chapter 8 - Class 11 Geography NCERT - Class Notes - Samagra Book Series Batch (Hinglish)avnish.k.verma.2014No ratings yet
- Statistics On Child Care (STENT)Document8 pagesStatistics On Child Care (STENT)Farmmy NiiNo ratings yet
- Accumulation in TDSDocument4 pagesAccumulation in TDSAnanthakumar ANo ratings yet