You might also like
- MethotrexateDocument2 pagesMethotrexateIvanne Hisoler83% (6)
- Methotrexate Drug StudyDocument1 pageMethotrexate Drug StudyAlexa Lexington Rae Zagado0% (1)
- Drug Study 1.1Document2 pagesDrug Study 1.1Arianne Nicole PinuelaNo ratings yet
- HydrocortisoneDocument2 pagesHydrocortisoneIvanne Hisoler100% (15)
- DR Anna Mira Lubis - Diagnostic Approach of ThrombocytopeniaDocument36 pagesDR Anna Mira Lubis - Diagnostic Approach of Thrombocytopeniayosua simarmataNo ratings yet
- Drugs For Cancer Patients: Mona Shrestha MN (Adult Nursing)Document77 pagesDrugs For Cancer Patients: Mona Shrestha MN (Adult Nursing)sushma shresthaNo ratings yet
- Drug Mechanism Clincal Use Side Effects Antifungal: Amphote Ricin BDocument30 pagesDrug Mechanism Clincal Use Side Effects Antifungal: Amphote Ricin BCess Lagera Ybanez0% (1)
- 0304 ConsultantoncallDocument4 pages0304 Consultantoncallnessimmounir1173No ratings yet
- Laboratory ReviewDocument3 pagesLaboratory ReviewSHARON GABRIELNo ratings yet
- Antihelmintic Drugs Humayunz CollectionDocument2 pagesAntihelmintic Drugs Humayunz CollectionTatenda BrunoNo ratings yet
- Intravascular Extravascular: Fe Storage Tibc SerumDocument2 pagesIntravascular Extravascular: Fe Storage Tibc Serumazhar hussinNo ratings yet
- Mnemonics Step 1Document4 pagesMnemonics Step 1Raji NaamaniNo ratings yet
- Anticancer Drugs: Pharm 3620 Human Pharmacology and Therapeutic PrinciplesDocument24 pagesAnticancer Drugs: Pharm 3620 Human Pharmacology and Therapeutic Principleszj5bnxbymzNo ratings yet
- Neoplasia (Mosby)Document5 pagesNeoplasia (Mosby)jmmacar19No ratings yet
- AntiprotozoalDocument2 pagesAntiprotozoalxelo_27No ratings yet
- Lung CaDocument1 pageLung CaAqila MumtazNo ratings yet
- Table: Selected Antibacterial Antibiotics Antibiotics THAT . Mechanism of Action Names of Drugs Notes and ProblemsDocument4 pagesTable: Selected Antibacterial Antibiotics Antibiotics THAT . Mechanism of Action Names of Drugs Notes and ProblemsTJNo ratings yet
- Anticancer Drugs: Alkylating AgentsDocument3 pagesAnticancer Drugs: Alkylating AgentsElijah Chiumya100% (1)
- Enzymes in Clinical Chemistry MLTDocument4 pagesEnzymes in Clinical Chemistry MLTwailjsNo ratings yet
- Hema Immuno.2Document8 pagesHema Immuno.2Marcel TabucolNo ratings yet
- Granules Speciality PDFDocument2 pagesGranules Speciality PDFMadhavi VutukuruNo ratings yet
- Hematologic MalignanciesDocument5 pagesHematologic MalignanciesPrisbert W. AlejoNo ratings yet
- Pharm Chemo Drugs SauldDocument6 pagesPharm Chemo Drugs Sauldneal100% (1)
- Sulfamethaxazole, Salbu + IpraDocument5 pagesSulfamethaxazole, Salbu + IpraGwyn RosalesNo ratings yet
- Bone Marrow FailureDocument2 pagesBone Marrow FailureGerardLum100% (1)
- Microcytic Type Aeitology Clinical Features Investigations ManagementDocument7 pagesMicrocytic Type Aeitology Clinical Features Investigations ManagementJason AnthonyNo ratings yet
- Cancer Chemotherapy 2Document8 pagesCancer Chemotherapy 2vrst7fhbq5No ratings yet
- Recombinant Human Erythropoietin Stimulates Erythropoiesis Via Division and Differentiation of Progenitor Cells in Bone MarrowDocument2 pagesRecombinant Human Erythropoietin Stimulates Erythropoiesis Via Division and Differentiation of Progenitor Cells in Bone MarrowGwyn RosalesNo ratings yet
- HydrocortisoneDocument4 pagesHydrocortisoneiammaiaNo ratings yet
- Anticancer Drugs: Pharm 3620 Human Pharmacology and Therapeutic PrinciplesDocument29 pagesAnticancer Drugs: Pharm 3620 Human Pharmacology and Therapeutic Principleszj5bnxbymzNo ratings yet
- Viii. PathophysiologyDocument2 pagesViii. Pathophysiologymacedon145377No ratings yet
- Red Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenDocument3 pagesRed Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenMaryam FadahNo ratings yet
- Ebr Hy CluesDocument16 pagesEbr Hy CluesStaporn KasemsripitakNo ratings yet
- Neuro Psych - Antiepileptic Drug ChartDocument5 pagesNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- Storage DisordersDocument1 pageStorage DisordersDian Putri NingsihNo ratings yet
- Parasitology Table 1Document5 pagesParasitology Table 1William BufNo ratings yet
- HydrocortisoneDocument3 pagesHydrocortisoneunkown userNo ratings yet
- Opioids & MSK TreatmentDocument6 pagesOpioids & MSK TreatmentNashrah HusnaNo ratings yet
- Hematology I ArconadoDocument37 pagesHematology I ArconadoReizel GaasNo ratings yet
- Metastatic Carcinoma of Prostate: AlkalineDocument2 pagesMetastatic Carcinoma of Prostate: AlkalineDjdjjd SiisusNo ratings yet
- Blood FunctionsDocument3 pagesBlood FunctionshelloaNo ratings yet
- Dopamine HCLDocument1 pageDopamine HCLIvanne Hisoler100% (3)
- Malarial RXDocument2 pagesMalarial RXalrainsNo ratings yet
- HEMOSTASISDocument12 pagesHEMOSTASISRyan PedregosaNo ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- Hematology SummaryDocument9 pagesHematology SummaryJovielle Hayden100% (1)
- Section XIX - Lysosomal Storage Diseases: Disease Deficient Enzyme Accumulated Substrate Findings InheritanceDocument2 pagesSection XIX - Lysosomal Storage Diseases: Disease Deficient Enzyme Accumulated Substrate Findings InheritanceKatharine NervaNo ratings yet
- Before: Source: Source: Source: Source: Source: Source: Source: Karch, Amy: 2009 Lippincott's Nursing Drug Guide, P. 407Document2 pagesBefore: Source: Source: Source: Source: Source: Source: Source: Karch, Amy: 2009 Lippincott's Nursing Drug Guide, P. 407SoniaMarieBalanayNo ratings yet
- Drugs Used For Blood Coagulation Disorders - KatzungDocument3 pagesDrugs Used For Blood Coagulation Disorders - Katzungsarguss14100% (6)
- Glomerulonephritis MindmapDocument1 pageGlomerulonephritis MindmapAlia AnasNo ratings yet
- MED (App17) - Approach To AnaemiaDocument5 pagesMED (App17) - Approach To AnaemiaFlora XuNo ratings yet
- Year Ii Pharmacology Drugs ListDocument21 pagesYear Ii Pharmacology Drugs ListsaifuddinNo ratings yet
- Laboratory Values: ElectrolytesDocument5 pagesLaboratory Values: ElectrolytesLauren Agatha ManipolNo ratings yet
- Neoplasia: Monoclonal Unregulated, and IrreversibleDocument10 pagesNeoplasia: Monoclonal Unregulated, and Irreversiblehippypsyduck mdNo ratings yet
- Antiparasitic & Antifungal DrugsDocument30 pagesAntiparasitic & Antifungal DrugsAbdullah AlkharsNo ratings yet
- Hyperparathyroidism Concept MapDocument2 pagesHyperparathyroidism Concept MapDeo FactuarNo ratings yet
- Shen Et Al. BMC Nursing (2023) 22:407Document13 pagesShen Et Al. BMC Nursing (2023) 22:407A HNo ratings yet
- Writesonic Chatsonic 1709993519576Document1 pageWritesonic Chatsonic 1709993519576A HNo ratings yet
- Quiz 1DTS 101 - Model Answers - PDF - 109803Document2 pagesQuiz 1DTS 101 - Model Answers - PDF - 109803A HNo ratings yet
- ElectrochemistryDocument4 pagesElectrochemistryA HNo ratings yet
- Presentation1smoking 120603021549 Phpapp02Document12 pagesPresentation1smoking 120603021549 Phpapp02A HNo ratings yet
- Status and Cost Analysis of Sabaki Tilapia FarmingDocument8 pagesStatus and Cost Analysis of Sabaki Tilapia FarmingA HNo ratings yet
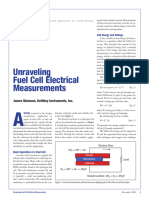
- 2581 Fuel CellDocument6 pages2581 Fuel CellA HNo ratings yet
- Mod. Ans G5 Mid Term Exam DTS 101 Fall 2017.Pdf - 114012Document3 pagesMod. Ans G5 Mid Term Exam DTS 101 Fall 2017.Pdf - 114012A HNo ratings yet
- 4 5915746627611529826Document4 pages4 5915746627611529826A HNo ratings yet
- Nursing Care Plan StrokeDocument2 pagesNursing Care Plan StrokeA HNo ratings yet
- Nursing Care Plan For Ischemic Stoke PDFDocument4 pagesNursing Care Plan For Ischemic Stoke PDFA HNo ratings yet
- Teaching Method-WPS OfficeDocument2 pagesTeaching Method-WPS OfficeA HNo ratings yet
- Practical For StudentsDocument50 pagesPractical For StudentsA HNo ratings yet
- Fuel Cell and Its Applications A ReviewDocument5 pagesFuel Cell and Its Applications A ReviewA HNo ratings yet
- NPSG Chapter HAP Jan2021Document14 pagesNPSG Chapter HAP Jan2021A HNo ratings yet
- Objective 1 - De-WPS OfficeDocument3 pagesObjective 1 - De-WPS OfficeA HNo ratings yet
- PosterDocument2 pagesPosterA HNo ratings yet
- Writing Portfolio 2 - CLO 2.7 - Descriptive ParagraphDocument12 pagesWriting Portfolio 2 - CLO 2.7 - Descriptive ParagraphA HNo ratings yet
- Turner's SyndromeDocument3 pagesTurner's SyndromeA HNo ratings yet
- ExampleDocument1 pageExampleA HNo ratings yet
- WA0054mmmDocument4 pagesWA0054mmmA HNo ratings yet
- Wa0001Document4 pagesWa0001A HNo ratings yet
- PomodoroDocument1 pagePomodoroA HNo ratings yet
- Neurology MCQDocument3 pagesNeurology MCQAlshare NisreenNo ratings yet
- HTN Keith RN Mike Kelly Case Study AnswersDocument13 pagesHTN Keith RN Mike Kelly Case Study AnswersabbieNo ratings yet
- Discharge PlanningDocument4 pagesDischarge PlanningKarl Angelo MontanoNo ratings yet
- Personal Hygiene ChecklistDocument5 pagesPersonal Hygiene ChecklistNISOL HRNo ratings yet
- 2019 Evaluation and Management of The Febrile Young Infant in The Emergency DepartmentDocument31 pages2019 Evaluation and Management of The Febrile Young Infant in The Emergency DepartmentMonica ValderramaNo ratings yet
- Zosyn (Piperacillin/tazobactram)Document2 pagesZosyn (Piperacillin/tazobactram)E67% (3)
- Define Education: Why Education Is Important To SocietyDocument5 pagesDefine Education: Why Education Is Important To SocietyzubairNo ratings yet
- Scientific Framework of Homeopathy Evidence Based HomeopathyDocument62 pagesScientific Framework of Homeopathy Evidence Based HomeopathyIrushaNo ratings yet
- COVID-19 Quarantine and Isolation CDCDocument1 pageCOVID-19 Quarantine and Isolation CDCmayaNo ratings yet
- Gastrointestinal Nursing ReviewerDocument17 pagesGastrointestinal Nursing ReviewerWena Grace NonanNo ratings yet
- CSC BIL Cambridge Manual KM-10224Document28 pagesCSC BIL Cambridge Manual KM-10224pottymouthedNo ratings yet
- Medical Geography - Concepts, Techniques and Approaches: June 2020Document16 pagesMedical Geography - Concepts, Techniques and Approaches: June 2020Andrea RincónNo ratings yet
- Diffuse Toxic GoiterDocument64 pagesDiffuse Toxic GoiterMuftihat IsrarNo ratings yet
- ST 43 PDFDocument1 pageST 43 PDFsorinNo ratings yet
- Dancing Is Fun and HealthyDocument8 pagesDancing Is Fun and HealthyRussel CanuelaNo ratings yet
- 00.docii 2020 Renal - UrogenitalDocument13 pages00.docii 2020 Renal - Urogenitalanderson ndabishakaNo ratings yet
- 10 Reasons Why Sugar Is Bad For YouDocument5 pages10 Reasons Why Sugar Is Bad For YouAgussNo ratings yet
- Rhesus Iso-ImmunizationDocument20 pagesRhesus Iso-Immunizationahmed shorshNo ratings yet
- Seroprevalence of Dengue Imunoglobulins and Awareness of Dengue Fever Among Healthy Blood Donors in Port Harcourt, NigeriaDocument6 pagesSeroprevalence of Dengue Imunoglobulins and Awareness of Dengue Fever Among Healthy Blood Donors in Port Harcourt, Nigeriaijmb333No ratings yet
- Student Health Ambassador Training August 2020Document113 pagesStudent Health Ambassador Training August 2020api-544103218No ratings yet
- Breast Cancer Related Lymphedema2.pdfL P 4Document12 pagesBreast Cancer Related Lymphedema2.pdfL P 4LýNo ratings yet
- Downloadable Test Bank For Introduction To Psychology 10th Edition PlotnikDocument24 pagesDownloadable Test Bank For Introduction To Psychology 10th Edition PlotnikThomasSanderspfcq100% (44)
- Prateek Chhabra - ReportDocument9 pagesPrateek Chhabra - ReportPrateek ChhabraNo ratings yet
- Approach To Abdominal Pain in The Emergency DepartmentDocument27 pagesApproach To Abdominal Pain in The Emergency Departmentdebra_euromNo ratings yet
- The Endocrine System Lesson 1Document44 pagesThe Endocrine System Lesson 1Heaven Dela CruzNo ratings yet
- Exceptional DevelopmentDocument2 pagesExceptional DevelopmentRiza Pepito - Leachon100% (1)
- Immunology in Health and DiseasesDocument7 pagesImmunology in Health and DiseasesLianneRaoNo ratings yet
- DrugsDocument77 pagesDrugsAnkush SharmaNo ratings yet
- Double Lumen Catheter Dr. Ahmad GhozaliDocument20 pagesDouble Lumen Catheter Dr. Ahmad GhozaliastarimediantoNo ratings yet
- Concept of Gara Visha and Dushi VishaDocument3 pagesConcept of Gara Visha and Dushi Vishaashutoshjha529No ratings yet